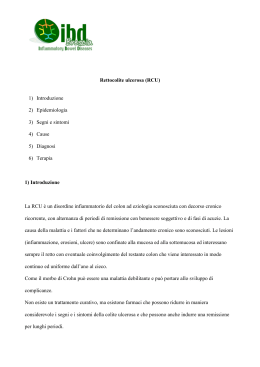
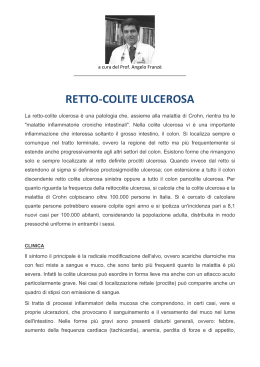
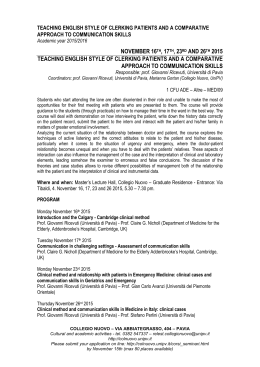
U.O.C Gastroenterologia Direttore: Prof..essa M. Chiaramonte U.O.S. “Centro per le malattie retto-perineali” -IBD UNITResponsabile: Dr.A. Geccherle Attualità terapeutiche nella RCU Verona 15/6/2012 Epidemiology and demographics ● Incidence – 10–20 per 100,000 per year ● Prevalence – 100–200 per 100,000 (vs CD: 50–100/100,000) – Jewish whites > non-Jewish whites > Blacks > Hispanics > Asians – Males = Females ● Diagnosis – At any age, but most commonly 15–30 or 60–80 years – By clinical history and endoscopy or radiographic findings, confirmed by biopsy Kornbluth A, et al. Am J Gastroenterol. 2010;105:501–23; Loftus CG, et al. Inflamm Bowel Dis 2007;13:254 –261; Friedman S, et al. Harrison’s 15th ed. 2001:1679–92; ECCO consensus guidelines for UC. JCC 2008;2:1–23 Company Confidential © 2011 Abbott 2 Regione Veneto Anno Classe Esenzione 2011 2010 009 Colite Ulcerosa e Crohn 009 Colite Ulcerosa e Crohn Sesso MASCHIO DONNA MASCHIO DONNA N. Pazienti N. Pazienti N. Pazienti 1.137 1.112 266 1.167 1.144 1.291 411 874 901 256 890 932 958 314 Provincia di Residenza Pazienti N. Verona Vicenza Belluno Treviso Venezia Padova Rovigo 1.198 1.169 271 1.210 1.204 1.354 429 934 951 257 939 992 1.032 335 TOTALE 6.835 5.440 TOTALE GENERALE 12.275 6.528 11.653 5.125 Colite Ulcerosa •Diffusa ed uniforme distribuzione dell’infiammazione •Iperemia intensa ed aspetto emorragico della mucosa •Scomparsa del reticolo vascolare •Friabilità della mucosa Estensione 2/3 dei casi sono limitati al colon sinistro Pancolite Colite sinistra Proctosigmoidite Proctite Storia Naturale della Colite Ulcerosa • All’esordio – Attività lieve – Attività moderata – Attività severa % Pazienti 55 30 15 L’andamento della malattia dipende dl grado di coinvolgimento del colon • Dopo una fase di attività – Probabilità nuova recidiva entro il primo anno 30 % – Probabilità nuova recidiva entro il secondo anno 20 % Truelove and Witts Severity Index* Variable Mild Disease Severe Disease <4 >6 Intermittent Frequent Temperature (°C) Normal >37.5 Pulse (beats/minute) Normal >90 Hemoglobin Normal <75% of normal value <30 >30 Stools (number/d) Blood in stool Erythrocyte sedimentation rate (mm/hr) * Moderate disease intermediate between mild and severe Reprinted with permission from: Truelove SC, Witts LT. Cortisone in ulcerative colitis: final report on a therapeutic trial BMJ 1955;2:1041-1048. Signs & symptoms: Mayo Score (DAI) ● Stool frequency – 0 (normal) to 3 (5 or more over normal) ● Rectal bleeding – 0 (no blood) to 3 (blood alone passed) ● Findings of flexible sigmoidoscopy – 0 (normal) to 3 (severe active disease) ● Physician’s global assessment (often correlates with above) – 0 (normal) to 3 (severe disease) Schroeder KW et al. N Engl J Med 1987;317:1625–9 Signs & symptoms: Mayo Score (DAI) ● Total Mayo Score ranges from 0-12 points – Clinical remission: ≤2 points with no individual subscore > 1 – Mildly active disease: 3-5 points – Moderately active disease: 6-10 points – Severely active disease: 11-12 points Schroeder KW et al. N Engl J Med 1987;317:1625–9 Attraverso quali parametri ottimiziamo la terapia ? 1. Diagnosi corretta 2. Selezione pazienti ad alto vs basso rischio 3. Terapia tempestiva e aggressiva in casi selezionati 4. Verifica risposta nella fase acuta e nel mantenimento 5. In casi dubbi,valutare un rapido cambiamento di strategia Ulcerative colitis as a progressive disease: The forgotten evidence. Torres J, Billioud V, Sachar DB, Peyrin-Biroulet L, Colombel JF. Inflamm Bowel Dis. 2011 Dec 11. ● Nella gestione della malattia di Crohn, all'inizio trattamento aggressivo è diventando accettato come una strategia per prevenire o ritardare la progressione a danni irreversibili dell'intestino. Non è ancora chiaro, tuttavia, se questo stesso concetto dovrebbe essere applicato per la colite ulcerosa. ● La progressione della malattia nella colite ulcerosa prende sei forme principali: estensione prossimale, stenosi, pseudopolipi, alterazione della motilità, disfunzione ano-rettali e alterata permeabilità. L'incidenza precisa di queste complicazioni e l’uso di un trattamento più aggressivo per impedirle sono ancora da determinare. Disease activity Approximately half of patients with UC will have chronic or relapsing symptoms 0 55% 6% 1% 37% Years 10 0 Solberg IC, et al. Scand J Gastroenerol 2009;44:431–40. 12 Years 10 Therapeutic Pyramid for Active UC Severe Surgery Cyclosporine Moderate Infliximab Systemic Corticosteroids AZA/6-MP Oral Steroids Mild Aminosalicylates Cosa fare e non fare per l’ottimizzazione della terapia convenzionale Cosa fare Cosa non fare Identificare pazienti con caratteristiche predittive di decorso di malattia disabilitante Ripetuti o prolungati trattamenti con corticosteroidi Intervenire precocemente con immunomodulatori Sottostimare gli effetti collaterali Rivalutare il paziente con tempistica appropriata (es. 2-4 settimane per CS; 36 mesi per IS) Prolungare la terapia con immunomodulatori se non viene raggiunta la remissione clinica Obiettivo da porsi: remissione senza corticosteroidi Trattare non solo i sintomi (“deep remission”) Ottimizzare precocemente la dose degli immunomodulatori Storia naturale della terapia con corticosteroidi nella CU Breve termine Attività della malattia Attività della malattia Attività della malattia Risposta completa 54% (41%–67%) Risposta parziale 30% (19%–43%) Nessuna risposta 16% Lungo termine (8%–27%) Risposta prolungata 49% (36%–62%) Dipendenza da CS 22% (13%–34%) Strategie terapeutiche convenzionali nella colite ulcerosa con 5-ASA formulations 5-ASA Oral formulations pH-dependent pH, time-dependent Topical formulations Foam Gel Enema Azoderivatives Suppository Efficacy of Oral vs. Topical, or Combined Oral and Topical 5-Aminosalicylates, in Ulcerative Colitis: Systematic Review and Meta-Analysis.Ford AC, Khan KJ, Achkar JP, Moayyedi P. Am J Gastroenterol. 2012;107:167-76. CONCLUSIONI: Mesalazina: piu' efficace la terapia combinata orale/topica della sola terapia orale (sia in fase attiva, sia nel mantenimento) Once daily oral mesalamine compared to conventional dosing for induction and maintenance of remission in ulcerative colitis: A systematic review and meta-analysis. Feagan BG, Macdonald JK. Inflamm Bowel Dis. 2012 May 29. ● Sistematicamente, si è esaminato e confrontato l'efficacia e la sicurezza di mesalazina una volta al giorno (OD) e mesalazina a posologia convenzionale per indurre e mantenenere la remissione nella colite ulcerosa (UC). ● Nessuna differenza significativa è stata dimostrata nei tassi di adesione farmaco o eventi avversi tra OD e dosaggio convenzionale. SPD476 uses MMX technology to deliver 5-ASA to the entire colon • Delayed and extended drug release formulation containing 1.2g 5-ASA • Highest 5-ASA drug loading per tablet MMX = MMX Multi Matrix System™ Gastro-resistant layer Hydrophilic polymers 5-ASA Lipophilic excipients Impact of MMX® mesalamine on improvement and maintenance of health-related quality of life in patients with ulcerative colitis. Hodgkins P, Yen L, Yarlas A, Karlstadt R, Solomon D, Kane S. Inflamm Bowel Dis. 2012 May 30 ● The sizeable burden of active mild-to-moderate UC on HRQoL was eliminated following 8 weeks' treatment with MMX mesalamine 2.4-4.8 g/day. HRQoL remained stable over 12 months of maintenance treatment in patients with quiescent UC Adacolum: agranulocitoferesi A randomized, double-blind, sham-controlled study of granulocyte/monocyte apheresis for active ulcerative colitis. Sands BE, Sandborn WJ, Feagan B, Löfberg R, Hibi T, Wang T, Gustofson LM, Wong CJ, Vandervoort MK, Hanauer S; Adacolumn Study Group. Gastroenterology. 2008 Aug;135(2):400- Conclusions: In this study, granulocyte/monocyte apheresis was well tolerated but did not demonstrate efficacy for induction of clinical remission or response in patients with moderateto-severe ulcerative colitis. Daily granulocyte and monocyte adsorptive apheresis in patients with active ulcerative colitis: a prospective safety and feasibility study. Yamamoto T, Umegae S, Matsumoto K. J Gastroenterol. 2011 Aug;46(8):1003-9 Conclusioni Questo è il primo rapporto sull’uso quotidiano GMA nel trattamento dei pazienti con UC. GMA quotidiana è sicura e ben tollerata senza gravi AE. Inoltre, GMA quotidiana è associata a rapido miglioramento dei sintomi clinici in pazienti con UC moderatamente attiva Anti-TNF e Rettocolite Ulcerosa RCU cronicamente attiva RCU severa, refrattaria alla terapia steroidea Anti-TNF: come utilizzarli e ottimizzarne l’uso • Conoscere le controindicazioni! • Curare solo la malattia infiammatoria attiva (endoscopia) • Definire endpoint che si vuole ottenere: l'interruzione di steroidi, portare il paziente in remissione profonda, il controllo di manifestazioni extraintestinali . • Pianificare attentamente le strategie di salvataggio per ogni farmaco • Individuare per la prima linea quale tipo di anti-TNF Approcci possibili per raggiungere e mantenere la remissione nella pratica clinica? • Identificare i pazienti che possono avere una prognosi sfavorevole e che possono trarre beneficio dalla terapia intensiva • Ottimizzare la terapia convenzionale in fretta • Introdurre terapia anti-TNF in modo tempestivo ai pazienti appropriati Select the patient Best responders Midium responders Poor responders Giovane paziente Malattia recente Diarrea Perdita di peso Alta CRP Ulcere della mucosa Nessun MDR Diarrea Add dolore Ostruzione Bassa CRP Ulcere della mucosa Lunga steroide-dip Paz. di vecchia data Lunga malattia Sintomatico No CRP MDR Approcci possibili per raggiungere e mantenere la remissione nella pratica clinica? • Identificare i pazienti possono avere una prognosi sfavorevole che possono trarre beneficio dalla terapia intensiva • Ottimizzare la terapia convenzionale in fretta • Introdurre terapia anti-TNF in modo tempestivo ai pazienti appropriati • Il paziente inizia con una dose piena di steroidi e mesalazina • Se la remissione è raggiunta entro 2-4 settimane ma diventano steroide-dipendente, iniziare IMM immediatamente • Se non è raggiunta remissione entro 2-4 settimane in corso di terapia convenzionale o se i pazienti sono intolleranti agli IMM iniziare biologici Approcci possibili per raggiungere e mantenere la remissione nella pratica clinica? • Identificare i pazienti possono avere una prognosi sfavorevole che possono trarre beneficio dalla terapia intensiva • Ottimizzare la terapia convenzionale in fretta • Introdurre terapia anti-TNF in modo tempestivo ai pazienti appropriati RCU e anti-TNF Linee guida italiane IG-IBD 2010 FX induction regimen can be used in pts with moderateI to severe UC who are refractory to systemic steroids [EL 1b, RG A] and in steroid dependent pts who are intolerant/refractory to thiopurines [EL 2b, RG C]. St 6A One year scheduled treatment with IFX can be used in pts who have responded to IFX induction. [EL 1b, RG A] The duration of the tp over 1 year should be carefully evaluated on a case-by-case basis. St 6B [EL 4, RG C] IG-IBD Statement 2 · RESPONSE: Clinical and endoscopic improvement according to the activity index use REMISSION: Stool frequency≤3/day with no bleeding or urgency · RELAPSE: Flare of symptoms in a patient who is in clinical remission · ORAL STEROID-REFRACTORY UC: Active disease in spite of an adequate dose and duration of prednisone therapy · (0.75–1 mg/kg/day or equivalent for at least 2 weeks) · I.V. STEROID-REFRACTORY UC: Persistent active disease or worsening despite equivalent methylprednisolone · 1mg/kg/day i.v. over a period of 1 week · STEROID-DEPENDENT UC: inability to stop steroids within 3 months of starting therapy, without clinical relapse, or relapse within 3 months after steroid weaning Results of the 2nd scientific workshop of the ECCO (IV): therapeutic strategies to enhance intestinal healing in inflammatory bowel disease. Armuzzi A, Van Assche G, Reinisch W, Pineton de Chambrun G, Griffiths A, Sladek M, Preiss JC, Lukas M, D'Haens G. J Crohns Colitis. 2012 May;6(4):492-502. Nella colite ulcerosa, la capacità dei corticosteroidi di indurre la guarigione della mucosa è ben riconosciuta. 5-ASA, thiopurine e gli agenti biologici sono in grado di indurre la guarigione della mucosa e, inoltre, di mantenerla. La guarigione mucosale va considerata nella pratica clinica, quando i sintomi persistono nonostante la terapia o quando si deve interrompere il trattamento. Al contrario, nei pazienti in cui la remissione clinica non è associata con la guarigione della mucosa,il protrarre il trattamento non è attualmente raccomandato. Rettocolite ulcerosa e Infliximab - ACT I e ACT II - Risposta clinica alla settimana 8 Guarigione mucosa: 62.0% (ACT1) e 60.3% (ACT 2). Rutgeerts P et al, N Eng J Med, 2005; 353: 2462-76. Rettocolite ulcerosa e Infliximab - ACT I e ACT II - Risposta clinica sostenuta alla settimana 30 e 54. Rutgeerts P et al, N Eng J Med, 2005; 353: 2462-76. Long-term infliximab maintenance therapy for ulcerative colitis: the ACT-1 and -2 extension studies. Reinisch W, Sandborn WJ, Rutgeerts P, Feagan BG, Rachmilewitz D, Hanauer SB, Lichtenstein GR, de Villiers WJ, Blank M, Lang Y, Johanns J, Colombel JF, Present D, Sands BE. Inflamm Bowel Dis. 2012 Feb;18(2):201-11. • Valutare l’efficacia, la qualità di vita e la sicurezza a lungo termine di infliximab in pazienti con CU attiva arruolati nell’estensione degli studi ACT-1 e ACT-2 nella terapia di mantenimento fino a 3 anni. Long-term infliximab maintenance therapy for ulcerative colitis: the ACT-1 and -2 extension studies. I risultati hanno dimostrato la superiorità di infliximab rispetto al placebo in termini di risposta clinica, remissione clinica, guarigione mucosale e riduzione nell’utilizzo di corticosteroidi: pazienti con RCU lieve o assente (PGA ≤ 1): 70,9%-90% pazienti in remissione (PGA = 0): 46,4%-65% • • Attività di malattia, valutata mediante il punteggio PGA (Physician• fs Global Assessment). Sub-scala a 4 punti (0 = normale; 1 = lieve; 2 = moderata e 3 = grave) del punteggio Mayo totale. Recommendations for the treatment of ulcerative colitis with infliximab: a gastroenterology expert group consensus. Reinisch W, Van Assche G, Befrits R, Connell W, D'Haens G, Ghosh S, Michetti P, Ochsenkühn T, Panaccione R, Schreiber S, Silverberg MS, Sorrentino D, van der Woude CJ, Vermeire S, Panes J. J Crohns Colitis. 2012 Mar;6(2):248-58. Epub 2012 Jan 10 This consensus statement provides useful and practical information on how to achieve evolving treatment goals with infliximab in moderate to severe UC. ULTRA 1: clinical remission at week 8 Mayo score remission (%) 35 30 *p=0.031, ADA 160/80 vs placebo 25 18.5% 20 15 10 9.2% 10.0% N=130 N=130 N=130 Placebo ADA 80/40 mg ADA 160/80 mg 5 N=390 0 ITT-A3 analysis set (NRI) Clinical remission: Mayo score ≤2 with no individual subscore >1 Reinisch W, et al. Gut, 2011; 60:780-787 41 Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: results of a randomised controlled trial. W Reinisch,WJ Sandborn, DW Hommes,G D’Haens, S Hanauer,S Schreiber, R Panaccione,RN Fedorak, MB Tighe,B Huang,W Kampman,A Lazar, R Thakkar. Gut 2011;60:780-787 • Efficacia dell'adalimumab nei pazienti con colite ulcerosa refrattaria a steroidi e immunosoppressori. • Il primo trial controllato nella colite ulcerosa mostra, nei pazienti con malattia moderata-severa refrattaria a steroidi ed immunosoppressori trattati con adalimumab, percentuali di remissione ad 8 settimane significativamente superiori al placebo ma piuttosto basse in termini assoluti (18,5%). Si rimane in attesa dei risultati di un second trial che ha valutato l'efficacia a 52 settimane. • Ultra 1 ULTRA 2: primary efficacy analysis for all patients Clinical remission at Week 8 and Week 52 Clinical remission (%) 25 p=0.019 p=0.004 20 17.3% 16.5% 15 10 9.3% 8.5% 5 n=246 n=248 n=246 n=248 0 Week 8 Week 52 ITT analysis set (NRI) Clinical remission: Mayo score ≤2 with no individual subscore >1 Sandborn WJ, et al. Gastroenterology 10.1053/j.gastro.2011.10.032 43 Placebo ADA 160/80/40 mg Adalimumab Induces and Maintains Clinical Remission in Patients With Moderate-to-Severe Ulcerative Colitis. Sandborn WJ, van Assche G, Reinisch W, Colombel JF, D'Haens G, Wolf DC, Kron M, Tighe MB, Lazar A, Thakkar RB. Gastroenterology. 2012;142:257-265. • Sostanzialmente confermati i dati a breve termine del precedente studio ULTRA 1: • Percentuale di remissione a un anno superiore al placebo ma in termini assoluti ferma al 22 per cento nei pazienti non precedentemente trattati con infliximab. • Nessun beneficio invece nei pazienti refrattari o intolleranti all'infliximab. • Da notare comunque che i pazienti arruolati in questo studio sembrerebbero ben rappresentativi della popolazione di pazienti con malattia refrattaria alle terapie codificate DDW 2012 Adalimumab in Active Ulcerative Colitis: A Real-Life Observational Study. Abstract Sa1887 • Adalimumab (ADA) appears to be effective in active ulcerative colitis (UC), according to a study presented here at Digestive Disease Week (DDW) 2012. A new Italian study has found that up to 25% of UC patients may achieve clinical remission within 3 months. • “We looked at efficacy data in patients with active colitis, and at 1 year, 65% were still on adalimumab,” said Alessandro Armuzzi, MD, Catholic University, Rome, Italy, on May 19. “It starts to work a little better after 12 weeks and then slowly increases the rate of remission.” • Dr. Armuzzi said the effectiveness of ADA in treating active UC is controversial. ADA is significantly better than placebo for both induction and maintenance of remission, according to controlled trials, but with little absolute benefit. Gestione della Colite Ulcerosa attiva severa refrattaria a terapia Severe ulcerative colitis of any extent ECCO statement 5F The response to intravenous steroids is best assessed objectively (by stool frequency, CRP and abdominal radiography) on or about the third day [EL2b, RGB]. Surgical options should be considered and discussed at this stage or earlier. Second line therapy with either ciclosporin [EL1b, RG B], or infliximab [EL1b, RG B] or tacrolimus [EL1b, RG B] will often be appropriate. If there is clinical deterioration colectomy is recommended. If there is no improvement within a further 4– 7 days, colectomy should usually be recommended Cyclosporine or infliximab as rescue therapy in severe refractory ulcerative colitis: Early and long-term data from a retrospective observational study. Mocciaro F, Renna S, Orlando A, Rizzuto G, Sinagra E, Orlando E, Cottone M. J Crohns Colitis. 2012 Jan 13 Infliximab or cyclosporine as rescue therapy in hospitalized patients with steroid-refractory ulcerative colitis: a retrospective observational study. Sjöberg M, Walch A, Meshkat M, Gustavsson A, Järnerot G, Vogelsang H, Hertervig E, Novacek G, Friis-Liby I, Blomquist L, Angelberger S, Karlen P, Grännö C, Vilien M, Ström M, Verbaan H, Hellström PM, Dejaco C, Magnuson A, Halfvarson J, Reinisch W, Tysk C. Inflamm Bowel Dis. 2012 Feb;18(2):212-8 Update on the management of ulcerative colitis. Hoentjen F, Sakuraba A, Hanauer S. Curr Gastroenterol Rep. 2011 Oct;13(5):475-85. Review ECCO: the European Crohn’s and Colitis Organisation Barcelona, Spain, February 16–18, 2012 ● Abstracts of the 7th Congress of ECCO ● the European Crohn’s and Colitis Organisation ● Barcelona, Spain, February 16–18, 2012 Severe ulcerative colitis Gastroenterology Department Negrar Hospital (Vr – Italy) January 2009 – December 2010 Metilprednisolone 7 days 1 mg/Kg iv. N= 14 64.2% Infliximab 5 mg/Kg N= 8 Responders N= 5 Non Responders N= 9 Urgent colectomy N= 1 35.7% Infliximab 5 mg/Kg N= 8 week: 0, 2, 6 87.5% Responder N= 7 Failure N= 1 Elective colectomy 12.5% week: 52 71.4% Sustained clinical response N= 5 Stop for complication Failure N= 1 N=1 Elective colectomy 14.3% Infliximab as rescue therapy for patients with severe ulcerative colitis refractory to systemic corticosteroids: A single centre open-label study M. Fortuna *, R. Montanari, A. Geccherle, A. Sartori,G. Ruffo, M.Chiaramonte Ospedale Sacro Cuore Don Calabria Negrar VR, Italy Conclusions Our study confirms the efficacy of Infliximab as analternative to colectomy in patients refractory to i.v. steroids. After one year of maintenance therapy with Infliximab, 5 patients who showed a response to induction treatment avoided colectomy. Both colectomies, in the patients with lackof clinical response, were performed on an elective regime. QUALE TERAPIA PER IL FUTURO ? New therapies for inflammatory bowel disease: from the bench to the bedside. Danese S. Gut. 2012 Jun;61(6):918-32. Epub 2011 Nov 23 . Components of the pathological response in IBD include the adaptive and innate immune systems, as well as the intestinal epithelium and endothelium. This study systematically reviews the mechanisms of action, efficacy and safety of new and emerging therapies that are currently in clinical trials and discusses future directions in the treatment of IBD. Failed therapies in UC Name Target Outcome Abatacept T-cell- inhibit costimulation RCT no effect in induction of remission AG011 GM bacteria that secretes human IL-10 Lack of clinical benefit MDX-110 Anti-IP-10- inhibit T-cell migration RCT failed to meet primary endpoint Rituximab Anti-CD20 on B cells Failed primary endpoint Natalizumab Anti α4-integrin adhesion molecule 1 study completed. Results diminished by 8wk- no further studies on plan Daclizumab & basilixumab Anti-IL-2 receptor - inhibits T-cell proliferation and activation No advantage over placebo and lack of efficacy Interferons immunomodulators Varied response. No advantage over conventional therapy Nicotine Various and mechanism unknown No more effective than placebo or conventional therapy. More SE 54 DDW 2012: Colitis Responds to Anti-TNF Therapy Nancy Walsh, Staff Writer, MedPage Today Published: May 24, 2012 ● Note that in this randomized controlled study, induction regimens of subcutaneous golimumab produced clinical response, mucosal healing, and improved quality of life in antiTNF naive patients with moderately to severely active ulcerative colitis despite current adequate treatment. ● Patients with ulcerative colitis treated with golimumab, a tumor necrosis factor (TNF) inhibitor, had robust clinical responses compared with placebo ● It's not yet possible to compare infliximab with golimumab because the drugs have not been studied head to head, but an advantage to golimumab may be its subcutaneous admission, while infliximab requires an infusion DDW 2012: A phase 2/3 randomized, placebo-controlled, double-blind study to evaluate the safety and efficacy of subcutaneous golimumab induction therapy in patients with moderately to severely active ulcerative colitis (UC): Pursuit SC (Abstract #943d) ● The data demonstrated that golimumab administered subcutaneously was significantly better than a placebo in inducing clinical response, clinical remission, mucosal healing and improving quality of life in patients participating in the study. DDW 2012: Colitis Responds to Anti-TNF Therapy: Vedolizumab Nancy Walsh, Staff Writer, 24 May 2012 ● Un nuovo anticorpo gut-selettivo monoclonale ha mostrato significativi benefici nei pazienti con colite ulcerosa refrattaria. ● A 6 settimane, il 47,1% dei pazienti trattati con vedolizumab aveva raggiunto una risposta clinica, rispetto al 25,5% di quelli randomizzati a placebo (P <0,0001). ● Vedolizumab si rivolge in modo specifico all’alpha-4/beta-7 integrina nel tratto gastrointestinale senza provocare l'immunosoppressione sistemica associata a meno specifici anticorpi monoclonali alfa 4-integrina come il natalizumab IBD UNIT Negrar Clinical effectiveness of selective granulocyte, monocyte adsorptive apheresis with the Adacolumn device in ulcerative colitis Habermalz B, Sauerland S. Dig Dis Sci. 2010 May;55(5):1421-8. Conclusions: Homogeneous evidence from seven RCTs shows that GMA apheresis induces a clinical remission in a higher proportion of UC patients as compared to conventional medical therapy.
Scaricare