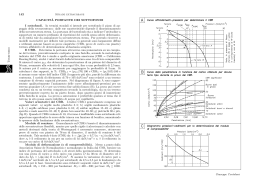
Lunedì 8 marzo 17.30 - 19.00 II SESSIONE Quando iniziare Raccomandazioni internazionali a confronto sul management terapeutico del paziente HIV 18.00 - 18.10 Expert opinion Iniziare con CD4>500 cell: vantaggi e svantaggi Cristina Mussini linica di Malattie Infettive, Azienda Ospedaliera Universitaria, C Policlinico di Modena In un mondo ideale L’approccio terapeutico all’infezione da HIV non dovrebbe differire da quello usato nei confronti delle altre infezioni e cioè la terapia dovrebbe essere iniziata immediatamente dopo la diagnosi. Risk of death associated with deferral of ART, according to CD4+ count at baseline, with adjustment for HIV-RNA level, age, and sex Kitahata MM, et al. N Engl J Med, 2009 Hazard ratios for AIDS or death for deferral of cART to a lower CD4 cell count range versus initiation at a higher CD4 cell count range When To Start Consortium, Lancet, 2009 -24-24-18 -18-12 -12 -6-6 (A) n = 403 median: - 182 range: (-626; -124) -24-24-18 -18-12 -12 -6-6 (B) n = 800 median:- 56 range: (-125; -5) -24 -24-18 -18 -12 -12-6 -6 (C) months n = 411 median: +20 range: (-4; + 883) Legend figure 2: Box-plots showing CD4 24 months before HAART according to 3 different pre-HAART CD4 patterns (A, B and C: steeper, in-between and constant, respectively). Group A (steepest pre-HAART CD4 rate) pre-HAART CD4 slope: - 10.8 cells/mm3 /month (95% CI: from -12.7 to -8.9) post-HAART CD4 slope: + 23.0 cells/month (95% CI: from +19.2 to 26.9) Group B (moderate pre-HAART CD4 rate ) pre-HAART CD4 slope: - 3.9 cells//mm3 month (95% CI: from -4.6 to -3.1) post-HAART CD4 slope: + 14.8 cells/month (95%CI: from +13.3 to 16.2) Group C (shallowest pre-HAART CD4 rate) pre-HAART CD4 slope: + 0.11 cells//mm3 month (95% CI: from -2.0 to +2.2) post-HAART CD4 slope: + 11.1 cells/ month (95% CI: from +7.1 to +15.1) Legend fig 3: graphs representing pre- and post-HAART CD4 slopes estimated by linear mixed models for the three groups (A, B and C) Duration of first STI period according to CD4 nadir P < 0.0001 Off therapy (days) Mean 95%CI 1306 1194 - 1419 1026 866 - 1187 538 350 - 725 259 162 - 356 CD4 naïve/memory cell ratios in patients with incomplete immunological response STRATUM 1: CD4 nadir 50 cell/L STRATUM 2: CD4 nadir 50 – 200 cell/L Robbins et al. CID 2009 T Cell Activation Declines Further During ART-mediated VL Suppression Hunt et al, JID, 2003 and 2008 La vita reale CD4 counts are low at start of HAART 2003–2005 • 42 countries • 176 sites • 33,008 patients Adapted from Egger M, 14th CROI Los Angeles, CA, USA, 25–28 Feb 2007. Abstract 62. ART Cohort Collaboration. http://www.art-cohort-collaboration.org Conclusions Regimens containing TDF/FTC or ABC/3TC increased limb fat and trunk fat and were not significantly different ATV/r led to greater gain in limb fat and trunk fat than EFV Lipoatrophy, even the mild protocol-defined form, occurred in 16% (95% CI 12-22 %) of the participants and was not significantly different between TDF/FTC and ABC/3TC or between EFV and ATV/r A5224s HIV Highlights From San Francisco clinicaloptions.com/hiv Cumulative ARV Exposure and Risk of Chronic Kidney Disease in EuroSIDA s6843 HIV-infected patients with ≥ 3 serum creatinine measures and corresponding body weight measures from EuroSIDA study – 21,482 patient-yrs of follow-up Cumulative exposure to TDF, ATV, LPV/RTV, or IDV each associated with increased risk of chronic kidney disease Risk of chronic kidney disease after stopping TDF remained elevated for 1 yr – Within 12 mos, IRR: 4.05 (2.51-6.53) – After 12 mos, IRR: 1.12 (0.63-1.99) Risk of chronic kidney disease after stopping ATV or LPV/RTV similar to patients never exposed Kirk O, et al. CROI 2010. Abstract 107LB. Giambattista Vico (1668–1744) Corsi e ricorsi storici • Antiretroviral Therapy for HIV Infection in 1996: Recommendations of an International Panel Charles C. J. Carpenter; Margaret A. Fischl; Scott M. Hammer; Martin S. Hirsch; Donna M. Jacobsen; David A. Katzenstein; Julio S. G. Montaner; Douglas D. Richman; Michael S. Saag; Robert T. Schooley; Melanie A. Thompson; Stefano Vella; Patrick G. Yeni; Paul A. Volberding JAMA. 1996;276(2):146-154 Giambattista Vico (1668–1744) Corsi e ricorsi storici Il senso della storia è, per Vico, sia nella storia che, nello stesso tempo, fuori di essa: gli effetti delle azioni umane vanno sempre oltre l’intenzionalità specifica degli uomini; l’uomo fa più di quanto sa e spesso non sa quello che fa. La storia è caratterizzata, secondo Vico, da un andamento progressivo ma non nel senso che tutto quello che viene dopo sia migliore di quello che viene prima, ma solo nel senso che la storia procede in un modo non meccanico né uniforme verso l’idealità CONCLUSIONI I clinici hanno sempre avuto buon senso nel seguire le linee guida e in questi anni hanno iniziato la terapia antiretrovirale senza seguire gli opposti estremismi. Vi sono ancora molte cose che non sappiamo e per rispondere non basterà uno studio randomizzato ma a breve termine. Certamente abbiamo spostato nella nostra pratica clinica l’inizio della terapia verso i 400 CD4 e non credo che i dati in nostro possesso siano in grado di far spostare il limite più in alto.
Scaricare