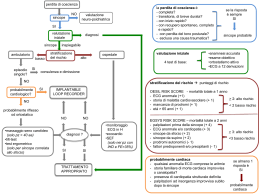
Esami ematochimici e biomarcatori nel paziente con Perdita Transitoria di Coscienza (T-LOC): PRO e CONTRO Gianfranco Cervellin UO Pronto Soccorso e Medicina d’Urgenza Azienda Ospedaliero-Universitaria di Parma www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it Due punti fermi: • 80% delle decisioni terapeutiche (anche quelle sbagliate!), in ambito ospedaliero, sono fondate su risultati di esami di laboratorio • Responsabilità del clinico nella fase pre-analitica! SINCOPE 2 0 1 5 www.gimsi.it Jones BA, Arch Pathol Lab Med, 2009 Brain-to-brain loop Responsabilità clinica Responsabilità clinica Responsabilità clinica Responsabilità del laboratorio Responsabilità clinica Responsabilità clinica Responsabilità organizza3va Il sogno del laboratorista ! Quesito fondato sulla diagnosi “pancrea3te? " lipasi” SINCOPE 2 0 1 5 www.gimsi.it “Lex parsimoniae. Pluralitas non est ponenda sine necessitate.” William of Ockham, 1287-1347 Il sogno del medico d’urgenza ! Quesito fondato sul sospe>o sincope " neuromediata? ipovolemica? gravidanza ectopica? TEP? aritmia? dissecazione aor3ca? aneurisma aorta addominale? etc. etc. Test specifico??? SINCOPE 2 0 1 5 www.gimsi.it “Lex vasti. Pluralitas est ponenda ex necessitate.” Medico di origini veneziane, 1955-vivente È evidente che le due visioni difficilmente si conciliano SINCOPE 2 0 1 5 www.gimsi.it Quindi: i profili! SINCOPE 2 0 1 5 www.gimsi.it I profili di laboratorio in emergenza-‐urgenza. Dubbi: • • • • • • Per diagnosi? Per quadro sindromico? Sono clinicamente efficien3 ed efficaci? Sono economicamente sostenibili? Sono Evidence Based? Sono Pa3ent Based? I profili di laboratorio in emergenza-‐urgenza • • • • • • • • • • • Dolore toracico Dolore addominale Dispnea Stroke Aritmie Sincope Alterazioni stato di coscienza Gastroenterite/Diarrea Trauma maggiore Us3oni ……… I profili di laboratorio in emergenza-‐urgenza • • • • • • • • • • Dolore toracico Dolore addominale Dispnea Stroke Aritmie Sincope Alterazioni stato di coscienza Diarrea Trauma maggiore Us3oni Profilo sincope??? SINCOPE 2 0 1 5 www.gimsi.it Profilo sincope??? SINCOPE 2 0 1 5 www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it Emerg Med Clin N Am 2010 Emerg Med Clin N Am 2010 Piccola parentesi: la gravidanza in PS SINCOPE 2 0 1 5 www.gimsi.it Una diagnosi di gravidanza Inaspe>ata ogni 3.8 giorni! Amer J Med 2015;128: 161-170 SINCOPE 2 0 1 5 www.gimsi.it Amer J Med 2015;128: 161-170 SINCOPE 2 0 1 5 www.gimsi.it Amer J Med 2015;128: 161-170 SINCOPE 2 0 1 5 www.gimsi.it Amer J Med 2015;128: 161-170 SINCOPE 2 0 1 5 www.gimsi.it Amer J Med 2015;128: 161-170 Increased cTnThs levels indicate adverse prognosis in patients with noncardiac causes of syncope, but not in patients with cardiac syncope, being a risk factor for adverse outcome by itself. SINCOPE 2 0 1 5 www.gimsi.it Emerg Med Clin N Am 2010 Di tuV i test diagnos3ci per la sincope, l’approfondita valutazione della storia clinica e l’ esame fisico hanno la più alta “resa” diagnos3ca Cosa cresce invecchiando? SINCOPE 2 0 1 5 www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it D-dimer is an old test: • Early 60s: fibrin(ogen) degradation products (FDP) • Early 80s: first monoclonal antibody-based assay for D-dimer, a specific fibrin(ogen) degradation products Topics • S3ll valid the “posi3ve/nega3ve” rule? Do age, gender, plasma levels ma>er? • Only useful in ruling out venous thromboembolism? • How to use it in the Emergency Department? SINCOPE 2 0 1 5 www.gimsi.it Topics • S3ll valid the “posi3ve/nega3ve” rule? Do age, gender, plasma levels ma>er? • Only useful in ruling out venous thromboembolism? • How to use it in the Emergency Department? SINCOPE 2 0 1 5 www.gimsi.it 2014;25:45-48 • Retrospec3ve inves3ga3on. Year 2012, ED of Academic Hospital of Parma (88958 visits) • All the pa3ents for whom a D-‐dimer test was requested by an EP in order to exclude or reinforce a diagnos3c suspicion of VTE according to clinical signs and symptoms (clinical Gestalt and/or predic3on rule based on Revised Geneva score or on Wells score). • All the cases displaying a value above the 243 ng/mL diagnos3c cut-‐off for VTE of the local immunoassay, regardless of their pre-‐test clinical probability for VTE, were selected. • Final cohort: 1647 pts. (mean age: 77±15 yrs.; 756♂ and 891♀) 2014;25:45-48 • Highly significant correla3on between age and D-‐dimer levels in the en3re cohort of pts. (R=0.08; p=0.010) • Highly significant correla3on between age and D-‐dimer levels in the VTE pts. (n=200; R=0.23; p=0.001) • Highly significant correla3on between age and D-‐dimer levels in the non-‐VTE pts. (n=1447; R=0.08; p=0.005) 2014;25:45-48 Infection: ~2/3 pneumonia VTE: 88 PE, 112 DVT Using the conventional cut-off of 0.5 mg/dl, PE/DVT could be excluded in 68% of patients, whereas the age-adjusted cut-off [(age ×0.016) mg/l] ruled out 77% of patients. Particularly in patients >70 years, the negative prediction accuracy of excluding a PE/DVT increased explicitly. The failure rate of the age-adjusted cut-off value was 0.8% (95% confidence interval 0.3–1.6%). These data suggest that method specific cut-off values calculated according to patient age and gender can be more accurate in identifying patients at a higher risk for VTE recurrence. These method-specific cutoff values are being evaluated in the ongoing prospective management multicenter DULCIS study. Topics • S3ll valid the “posi3ve/nega3ve” rule? Do age, gender, plasma levels ma>er? • Only useful in ruling out venous thromboembolism? • How to use it in the Emergency Department? SINCOPE 2 0 1 5 www.gimsi.it 1990 2014, epub ahead of print • An inverse and highly significant correlation was found between serum potassium and D-dimer (r = −0.21; p < 0.001), even after adjustments for age and sex. • The relative risk for a positive D-dimer value attributed to hypokalemia was 1.64 (95% CI, 1.02 to 2.63; p = 0.040). SINCOPE 2 0 1 5 www.gimsi.it Medicine 2015;94(4):e471) 34 studies. The pooled sensitivity of D-dimer levels in AAD patients was 94.5% (95% confidence interval [CI] 78.1%–98.8%,P<0.001) The specificity was 69.1% (95% CI 43.7%–86.5%,P¼0.136). The pooled area under the receiver-operating characteristic curve for D-dimer levels in AAD patients was 0.916 (95% CI 0.863–0.970, P<0.001). D-dimer levels are best used for ruling out AAD in patients with low likelihood of the disease. SINCOPE 2 0 1 5 www.gimsi.it Topics • S3ll valid the “posi3ve/nega3ve” rule? Do age, gender, plasma levels ma>er? • Only useful in ruling out venous thromboembolism? • How to use it in the Emergency Department? SINCOPE 2 0 1 5 www.gimsi.it Preanalytical issues: remember Rev. Thomas Bayes! Rev. Thomas Bayes 1702 – 1761 2009;16:256-60 • Of 237 patients enrolled, 205 patients had a suitable plasma sample and complete follow-up. • Nearly a half of all patients (n=94; 46%) had a plasma D-dimer concentration above the upper limit of normal. • An elevated plasma D-dimer concentration was found in all patients with a pulmonary embolus. • Plasma D-dimer is frequently raised in patients presenting with syncope to the ED and does not predict 1-month serious outcome or death. • We conclude that there is no role for the routine measurement of D-dimer in themanagement of patients presenting to the ED with syncope. SINCOPE 2 0 1 5 www.gimsi.it a n u è o s r e p o p m e t i d a r o i “Ogn ” e r i n e v v a ’ l r e p o n n a d i d à t i l probabi aparte Napoleone Bon “La tecnologia è considerata – erroneamente -‐ un sos3tuto efficace del tempo.” Bernard Lown, Lituania 1921(inventore del defibrillatore; S. di Lown-Ganong-Levine….) Take your 3me and observe the pa3ent! SINCOPE 2 0 1 5 www.gimsi.it Documento di consenso GIMSI-‐AcEMC (*) Ges3one della sincope di natura inspiegata dopo la valutazione iniziale in Pronto Soccorso I.Casagranda (chairman), M.Brignole, S.CenceV, G. Cervellin, G.Costan3no, R.Furlan, G. Mossini, F. Numeroso, M.Pesen3 Campagnoni , P. Pinna Parpaglia, A Ungar. SINCOPE 2 0 1 5 www.gimsi.it Keywords: 1. OBI 2. Syncope Unit SINCOPE 2 0 1 5 www.gimsi.it Messaggio (scien3fico) finale: Per gli esami di laboratorio u3lizzare un unico percorso clinico… SINCOPE 2 0 1 5 www.gimsi.it Il percorso vena (del paziente) " cervello (del medico) SINCOPE 2 0 1 5 www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it SINCOPE 2 0 1 5 www.gimsi.it
Scaricare