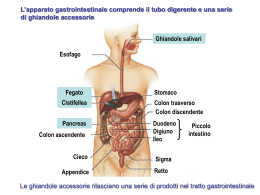
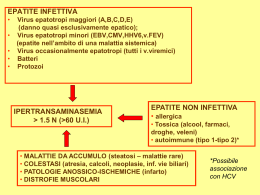
Epatite virale Lezione Scuola di Specializzazione in Medicina del Lavoro Caratteristiche essenziali dell’infezione da virus dell’epatite B DNA virus Non direttamente epatotossico Il danno epatocellulare è generato dalla risposta immunitaria dell’ospite Maggior parte delle infezioni asintomatiche( specie soggetti giovani) Maggior parte delle infezioni autolimitantesi con sviluppo di immunità In circa il 5% dei casi si sviluppa un’infezione persistente. Storia naturale epatite B persistente non trattata HBsAg per tutta la vita HBeAg tende a scomparire quando compare anti HBe DNA virale si riduce fortemente con comparsa anti Hbe, ma non scompare Implicazioni per immunoprofilassi:dopo puntura con ago contenente sangue di soggetto HBsAg positivo l’immunoprofilassi va fatta indipendentemente dallo status Hbe del soggetto Carrier HBeAg negativi Nella gran parte dei casi:a) bassi livelli di DNA virale;b)aminotransferasi normale;c)prognosi favorevole In Italia, nel 15-20% dei casi questi pazienti hanno alti livelli di DNA virale in circolo e aminotransferasi elevate. In questi pazienti è indicata la terapia antivirale Epatite B cronica ed epatocarcinoma Aumento del rischio di 100 volte HBeAg positivi hanno il rischio massimo Screening semestrale con alfafetoproteina e/o ecografia Alfafetoproteina ha un alto valore predittivo negativo, ma un valore predittivo positivo compreso tra il 9 e il 30% Infezione persistente da virus B -Viremia continua (a titolo variabile) -Forme sintomatiche o asintomatiche -ALT e AST normali e biopsia normale: carriers -Alterazioni della funzione e dell’istologia: epatite cronica -Cirrosi si sviluppa nel 20% dei casi di epatite cronica Strategie per la prevenzione di HBV Evitare comportamenti ad alto rischio Prevenire l’esposizione a sangue e fluidi corporei Screening delle gravide al III trimestre Immunizzazione attiva e passiva Vaccinazione epatite B (1) L’OMS raccomanda un programma di vaccinazione per tutti i bambini e gli adolescenti Altri gruppi a rischio: lavoratori della sanità espostial sangue Disabili ospitati in strutture e lavoratori delle strutture Vaccinazione epatite B (2) Emodializzati Soggeti che ricevono trasfusioni fattori della coagulazione concentrati Conviventi e partner sessuali di soggetti HBV positivi Adottati provenienti da paesi con endemia da HBV Vaccinazione da epatite B (3) Viaggiatori che trascorrono più di 6 mesi in paesi con endemia da HBV in stretto contatto con popolazioni locali Viaggiatori che hanno contatto con sangue o rapporti sessuali in paesi con alta o intermedia diffusione di HBV Soggetti che hanno più di un partner sessuale nell’arco di 6 mesi Vaccinazione epatite B (4) Omosessuali Tossicodipendenti Ricoverati in strutture psichiatriche Rischi della vaccinazione Nessuno Virus epatite B: immunizazione passiva Candidati: neonati da madri HBsAg +,soggetti a contatto con sangue o fluidi corporei HBsAg+,partner sessuali di soggetti HBsAg+,bambini di età inferiore ad 1 anno a contatto con soggetti in cui si sia sviluppata un’epatite acuta tipo B. Immunizzazione passiva: somministrazione Tempi: neonati entro 24 ore, contatto ago entro 7 giorni, rapporto sessuale entro 14 giorni Modalità: somministrato assieme alla prima dose di vaccino Efficacia: neonati 95%, altre categorie 75% Caratteristiche del virus dell’epatite C Centosettanta milioni di persone infette (2% popolazioni mediterranee) Cronicizza nella gran parte dei casi Trasmissione via ago o trasfusioni (in alcuni casi non identificabile la via di trasmissione) Trasmissione materno-fetale e sessuale rara Definizioni Tempi vaccinazione: 0,1,6 mesi Responders: 1-2 mesi dopo il ciclo hanno livelli di anti-HBsAg non inferiori a 10 mUI/ml Non responders: quelli con livelli inferiori a 10 mUI/ml Follow-up post-vaccinazione Responders: nulla Follow-up post-vaccinazione Non responders HBsAg/anti HBc negativi:quarta dose di vaccino e quindi nuova valutazione 1-2 mesi dopo. Se ancora non responders, quinta e sesta dose di vaccino e nuovo test 1-2 mesi dopo l’ultima dose. Possibili strategie alternative di vaccinazione (nuovi vaccini,tre dosi a dosaggio ridotto ogni 2 settimane,vaccino A e B combinato, vaccinazione standard ad alte dosi, etc…) Lavoratori con isolata presenza di anti HBc (1) Testare per IgM antiHBc e HBV DNA Se negativi, praticare la prima dose di vaccino e testare 30 giorni dopo. Un titolo anti HBsAg non inferiore a 50 mUI/ml è segno di risposta anamnestica e non richiede prosecuzione della vaccinazione. Questi soggetti sono protetti da reinfezione e non necessitano di immunoprofilassi in caso di esposizione Lavoratori con isolata presenza di anti HBc (2) Se anti HBsAg inferiore a 50 mUI/ml, completare la vaccinazione con 3 dosi e comportarsi come nei soggetti sierologicamente negativi. Questi soggetti vanno trattati con immunoprofilassi in caso di esposizione Gestione dopo esposizione occupazionale Esposizione percutanea: incoraggiare sanguinamento e lavare con acqua e sapone (eventuale aggiunta di antisettici/disinfettanti). Contaminazione cutanea: lavare con acqua e sapone (eventuale aggiunta di antisettici/disinfettanti) Contaminazione oculare: lavaggio con acqua Valutazione del rischio dopo esposizione Valutazione dello status HBV e HCV nell’esposto e nel paziente Conservare un campione di sangue dell’esposto e del paziente Valutare la potenzialità di trasmissione in base al tipo e al materiale biologico Se lo status HBV e HCV del paziente rimane ignoto considerarlo infetto. Status HBV Anti HBs HBIg(0.0 Vaccino 6 ml/kg) HBV Non vaccinato >10mUI/ml Nulla <10mUI/ml Schema 0-1 mese Vaccinazione incompleta o non sa se ha completato >10mUI/ml Nulla <10mUI/ml Schema 0 Non responder Vaccinato. Risposta ignota Schema 0-1 mese >10mUI/ml Nulla <10mUI/ml Schema 0 Già fatte 4 dosi o 2 cicli Responder a precedente vaccinazione no commento Vaccino e HBIG Schema 0-1- simultaneamente 2-12 mesi Come sopra Completare o schema 01-2-12 mesi Schema 0-1- Come sopra 2-12 mesi Come sopra Scema 0 Schema 0-1 mese Vaccinazione alternativa? no no Status HBV Anti HBs Vaccino HBV commento Non vaccinato Schema standard Valutare risposta 1-2 mesi dopo l’ultima dose Vaccinazione incompleta o non sa se ha completato Completare o ricominciare secondo schema standard Come sopra Non responder Schema standard Come sopra Nulla 1 booster e test a 1-2 mesi. Se ancora <10 schema standard Come sopra Vaccinato. Risposta ignota >10mUI/ml <10mUI/ml Già fatte 4 dosi o 2 cicli Responder a precedente vaccinazione Vaccinazione alternativa? no no Rischio di trasmissione con ago contaminato HBV: 30% HCV: 3% HIV: 0.3% HBV DNA virus Cronicizzazione: rara Contagiosità: elevata Trasmissione perinatale: frequente Contagio sessuale:frequente Vaccino: si HCV RNA virus frequente bassa Rara Raro no Genotipi HCV 6 genotipi, denominati in numeri arabi da 1 a 6 Genotipo 1a e 1b: i più comuni in USA ed Europa Occidentale Genotipo 2 e 3: predittivi di migliore risposta alla terapia Genotipo 4: comune in Egitto, genotipo 5 comune in Sud-Africa, genotipo 6 comune nel Sud-Est Asiatico Caratteristiche essenziali del virus C Non direttamente epatotossico Infezione per lo più asintomatica Cronicizzazione frequentissima (80%), con epatite cronica Nel 20% degli infetti si sviluppa cirrosi Fattori che accelerano la progressione della malattia: alcool, coinfezione con HBV,sesso maschile, infezione in età avanzata. Manifestazioni extraepatiche HCV Crioglobuline nel 50%. Vasculite (porpora, altralgia, astenia) nel 10-15%. Glomerulonefrite membrano-proliferativa Manifestazioni neurologiche Crioglobulinemia essenziale mista (tipo II) Tests diagnostici per HCV Enzyme immunoassay: in popolazioni a basso rischio, i falsi negativi sono meno dell’1%. Rischio di falsi negativi in immunocompromessi, insufficienza reanale, crioglobulinemia essenziale mista. Rischio di falsi positivi in soggetti senza fattori di rischio e senza segni di epatopatia quali donatori e lavoratori dela sanità. Tests confermativi per HCV Immunoblot ricombinante: può essere indicato nei positivi a basso rischio Test qualitativo per HCV-RNA con PCR: indicato nei pazienti con enzyme immunoassay con sospetta epatite acuta, in soggetti con epatite da causa non identificata, e in quelli con cause note di falsa negatività al test anticorpale Linee guida europee prevenzione epatite B e C in lavoratori sanità Programmi educazionali e training Protocolli scritti per una rapida trasmissione dei casi, valutazione, consulenza,trattamento e follow-up in caso di esposizione occupazionale che può porre i lavoratori della sanità a rischio di contrarre l’infezione Training e programmi educazionali Informazione Implementazione delle precauzioni standard Fornitura di mezzi di protezione adeguati Miglioramento delle procedure di sicurezza Vaccinazione Gestione post-esposizione Training e programmi educazionali Formale identificazione di un addetto a cui il lavoratore può fare urgente riferimento in caso di esposizione e che è responsabile del management post-esposizione,della somministrazione della profilassi e del follow-up clinico e sierologico Training e programmi educazionali L’accesso a medici che possono provvedere alla cura post-esposizione dovrebbe essere possibile durante tutte le ore lavorative, incluse notti e week-end I lavoratori dovrebbero essere informati dell’importanza clinica e medico-legale di riportale l’esposizione, come riportarla e a chi riportarla Vaccinazione Tutti i lavoratori della sanità dovrebbero essere vaccinati contro l’HBV secondo uno schema standard. Prima dell’assunzione sul lavoro è fortemente raccomandata la vaccinazione o la dimostrazione di immunizzazione Lo screening pre-vaccinazione non ha indicazione routinaria Vaccinazione Il titolo anticorpare anti HBsAg dovrebbe essere valutato 1-2 mesi dopo il completamento delle tre dosi di vaccino La vaccinazione combinata A e B è raccomandata in lavoratori suscetibili con HCV o altre epatopatie Esposizione ad HCVAb+ o non identificabile Testare il lavoratore esposto per HCVAb (EIA) a 0-3(?)-6 ed ev. 12 mesi. Confermare test positivo con HCV RNA ALT a tempo 0 e quindi mensilmente per 4 mesi (Se aumenta HCV RNA) Esposizione ad HCVAb- Se possibilità di falso negativo, comportarsi come esposizione ad HCVAb Angina - Carbon monoxide Sources of incomplete combustion: Furnaces, boilers Internal combustion engine (warehouses, auto plants) Hazards increased in cold weather with closed doors and windows Carbon monoxide carboxyhemoglobin Binds to hemoglobin more avidly than O2 (CO has 200x oxygen’s affinity) Shifts oxygen dissociation curve to “left”: Tissue anoxia the result Binds mitochondrial enzymes and myoglobin Increases platelet stickiness Deceases arrhythmia threshold CO and hemoglobin oxygen-dissociation curve 100 % Saturation CO Normal 75 50 25 0 0 20 40 60 80 100 Partial Pressure Oxygen Reduced oxygen-carrying capacity of carboxyhemoglobin at high CO levels 20 0% COHgb 16 O2 content (ml/dL) 60%COHgb 12 Anemia (40% nl) 8 4 0 0 20 40 60 PO2 (mm Hg) 80 100 Angina : Carbon monoxide CarboxyHgb levels and symptoms: Cardiac compensatory effects seen at carboxyHgb levels 8 -10%: HA, lightheadedness, some chest pain EKG disturbances (extrasystoles, PVCs, atrial fibrillation) at higher levels (10-25%) Dependent on previous cardiac status and susceptibility: Cigarette smokers chronically at ~5% Individuals with pre-existing CAD may develop angina with moderate activity at carboxyHgb levels as low as 3 - 5% Carbon monoxide: Exposure limits NIOSH REL: 35 ppm for 10-hour TWA Equivalent to 5% COHgb level Uptake will increase with physical exertion: Exposure should be correspondingly limited in jobs with high physical demands OSHA STANDARD: 50 ppm /TWA8 ® ACGIH: TLV : 25 ppm/ TWA8 BEI : 3.5% COHgb ® More protective of sensitive groups. BEI may be useful in documentation of significant exposure. Carbon monoxide Methylene Chloride CH2Cl2 Solvent: degreasing, paint stripping Absorption through respiratory route or through skin Metabolized in bloodstream to CO Methylene Chloride May elevate carboxyhemoglobin to 10% or more especially in poorly ventilated space Probably not significant to healthy person; may become mildly symptomatic Cigarette smokers, those with angina or current CHD a concern: excess CO may trigger symptoms Methylene Chloride OSHA Standard: 25 ppm/ TWA8: STEL 125 ppm NIOSH: As low as can be achieved (carcinogen) ! Because of metabolic conversion to CO, the biological life of COHgb from methylene chloride is longer than that from direct CO exposure Chronic exposure to CO associated with cardiovascular mortality: NYC bridge and tunnel officers Carbon monoxide:Long-term exposure effects SMRs for death from cardiovascular disease of bridge (low-COexposure) and tunnel (high) officers in NYC: Duration of Employment <10 years >10 years Total Bridge Officers 0.87 (0.70-1.07) 0.81 (0.56-1.15) 0.85 (0.71-1.02) Tunnel Officers 1.07 (0.77-1.44) 1.88 (1.36-2.56) 1.35 (1.09-1.68) Stern FB et al: Heart disease mortality among bridge and tunnel officers exposed to carbon monoxide. Am. J Epidemiol. 1988; 128: 1276-1288 Angina: Nitrates Noted to have vasodilatory effects in explosives workers Tolerance to absorbed nitrate symptoms (headaches, tachycardia, diastolic HTN) develops quickly Dynamite and other explosives manufacture Ethylene glycol Glycerin Nitrator HNO3 H2SO4 Dynamite HandPacking House “Dope” Dynamite Mix House Machine Packing (Cartridge-filling) Houses Liquid NTG / EGDN storage and supply “Dope” Dynamite Case Houses Gelatin Mix House Gelatin Packing (Cartridge-filling) Houses Magazine and Shipping Gelatin Case House H2C-O-NO2 H-C-O-NO2 H2C-O-NO2 nitroglycerin H2C-O-NO2 H2C-O-NO2 ethylene glycol dinitrate Acute effects in workers noted in early 1960s: Sudden death: 24-96 hours after exposure ceased (weekends/holidays) “Monday Morning Angina”: Relieved by RTW, nitrate meds: coronary spasm in absence of CAD Three-fold increase in acute deaths in younger men from ischemic CHD Angina: Nitrates Mechanism of acute effects not clear: Rebound vasospasm vs. arrhythmias (VF) triggered by re-exposure CAD risk increased 2-3x after 20 years exposure: persists after removal Possible HTN after cessation of exposure Atherogenesis Carbon disulfide (CS2) • Cellulose-derived materials • Rayon • Cellophane • • • • Solvent for rubber, oils Pesticides Fumigant for grain, books Microelectronics industry Viscose process for Rayon manufacture CS2 Lye Wood Flakes Raw Cellulose Cellulose Xanthate H + Solution Viscose Zn++ “Ripening” H2SO4 Rayon Filaments Spinning CS2 Filtering CS2 Cellulose flakes after lye treatment Viscose emerging from spinneret. CS2 is given off when viscose cross-links to form rayon Deaths among operatives and staff aged 45-64 with > 10 yr employment in rayon factories Occupation P-Y at risk Coronary Heart Disease Other CV Disease Obs Exp Obs Exp Operatives Viscose Making 2221 5 7.2 2 5.0 Viscose Spinning 4585 28* 14.6 15 9.9 Non-process 1997 6 8.0 10 6.1 Spinning 1502 9** 4.3 1 2.8 Non-process 752 3 2.3 2 1.6 Staff * 2 = 12.2 p<0.001 ** 2 = 5.2 p<0.05 Tiller JR, Schilling RS, Morris JN. Occupational toxic factor in mortality from coronary heart disease. Br Med J 1968; 4:407-11 Carbon Disulfide and Atherogenesis RR of 2 to 5x for death from CAD Epidemiologic evidence suggests a direct role in atherogenesis in blood vessels: Enzyme inhibition by metabolites of CS2 • React with amino acids to form dithiocarbamates: these chelate trace metals and react with enzyme cofactors • May interfere to increase elastase activity, disrupting blood vessel walls • May decrease fibrinolytic activity and enhance thrombosis Japanese CS2 workers: Retinal microaneurysms Japanese CS2 workers: Retinal hemorrhages Carbon Disulfide OSHA Standard: 20 ppm TWA8 MAC: 100 ppm/30 minutes NIOSH REL: 1 ppm TWA10 STEL: 15 ppm/15 minutes ® ACGIH BEI : Urine TTCA: 5mg/g creatinine End of workshift urine sample. Dysrhythmias Chlorofluorocarbons (Freon® etc) • Refrigeration, air conditioning, propellants • May sensitize myocardium to catechol effects Other solvents implicated in sudden death: • Trichloroethylene, toluene, benzene Findings at autopsy usually unremarkable: c/w sudden death from arrhythmias Cardiomyopathy Cobalt: used to stabilize beer foam (1960’s: Canada, Belgium) Cardiomyopathy reported in beer drinkers several months afterward Cardiomyopathy: Cobalt Dose-related: seen in heavy drinkers greatest risk in those drinking >10L/day (!) 22 - 50% mortality in some series Why this group? CM not seen in cobalt therapy for anemia Probable synergistic effect with alcohol, poor diet Hypertension Associations with several occupational exposures and agents Mechanisms are varied and depend on action of agent Hypertension Lead Probable mechanism is via renal injury May also increase vascular tone and resistance Chelation may improve HTN in acute Pb intoxication, but will not reverse if longstanding renal damage is present Cadmium possibly associated with HTN; noted to occur at levels below nephrotoxic dose Hypertension Carbon disulfide Vascular nephropathy and accelerated atherogenesis appear to be mechanisms Noise, shiftwork Postulated effects mediated by stress response (increase sympathetic and hormonal mediator release) Job Strain and Cardiovascular Disease Body of evidence suggests relationship between job strain and cardiovascular mortality Main associations are with exposure to high psychological demands and low control over job Professional drivers (especially urban transport) have the most consistent evidence of increased risk Social Class and Cardiovascular Disease Unskilled manual workers (Class V) have considerably increased risk when compared with professionals (Class I) STANDARDIZED MORTALITY RATIO Pioneering work of Marmot showed increased CHD mortality related to social status. 190 170 150 130 110 90 70 50 I II III IV V Cardiovascular effects on work Some figures on heart disease in US: 1.5 million MI each year Nearly 200,000 CABG per year Over 80% of workers are generally able to return to work after initial MI or CABG Cardiovascular effects: Return-to-Work after MI Medical Factors Major predictors of RTW: • LV dysfunction • persistent ischemia / angina after treatment Non-Medical Factors • • • • Coping styles Perception of work (demands, satisfaction) Age, gender, education Benefits/incentives Cardiovascular effects of work Reinfarction and death NOT more frequent at work Many workers older (>50) and have moved into sedentary roles even preinfarction Longshoremen study: Lowest rates of CAD mortality linked to heaviest jobs: Activity level CV Mortality Sudden Death High 26.9 5.6 Medium 46.3 19.9 Low 49.0 15.7 Assessing work capacity /capabilities History: Review of prior and current symptoms • CP, dyspnea, orthopnea, etc Evidence of improvement with treatment? Descriptions of exertional tolerance (routine activities, work simulations) Current medicines Physical: Signs on examination • • • • arrhythmias JVD edema chest exam Review previous and current records Assessing work capacity /capabilities Exercise EKG • May help refine judgement about RTW, in jobs requiring high exertion • Ability to reach Bruce Stage 4 on treadmill (12 minutes; ~8-9 METs) indicates low risk of subsequent cardiac event • Most individuals after single uncomplicated MI can generate 8+ METs before fatigue or discomfort Exercise EKG Better for assessing isotonic exercise/work (walking, running etc) Results in cardiac output, BP remains stable through peripheral vascular resistance, Exercise testing may not yield good estimate of capabilities for isometric work (lifting, static exertion) BP elevates without reduction in PVR Assessing work capacity: Some numbers 3.5 METs : Bartending, frequent walking with 10lb objects (many office jobs) 4 - 5 METs : Painting, masonry work, light carpentry 5 - 6 METs : Lighter digging, shoveling 6 - 7 METs : Heavier or more frequent shoveling 7 - 8 METs : Carrying 50-60 lbs; sawing hardwood Assessing work capacity /capabilities Job description: Always request Assess static vs dynamic work Other stressors (temperature, psych) Other exposures (CO, cigarette smoke) Simulated work (+/- exercise EKG) may be better in judgment of capabilities than testing in lab setting Specialist opinion: but beware of conservatism Work capacity: Some guidance Average energy demands of job can safely be 40% of peak workload Peak energy demands of job should be < maximum workload achieved on testing Thus individual generating 8+ METs can be reasonably asked to work at light-medium physical demand level Over half of post-CABG patients considered “totally disabled” could have safely performed their normal duties or equivalent work, based on exercise testing results Lundbom J, et al. Exercise tolerance and work abilityfollowing aorto-coronary bypass surgery. Scand J Soc Med 1994;22:303-8. Consider in the disabled individual: Inadequate treatment Depression Whether accommodation or changing nonessential requirements of job will allow return Socio-economic explanations What about exercise-testing of asymptomatic workers?? Predictive value of positive test is low in younger asymptomatic individuals: High false-positive rate requires additional work-up in many cases May have better predictive value in > 40yo with other risk factors (smoking, obesity, +FH, hypercholesterolemia, etc) Fitness-for-Duty Evaluations Many safety-sensitive jobs (fire, police) have qualification requirements based on exercise testing or physical fitness standards Principles outlined in last slide apply: predictive value may be low in younger/healthier workers Be careful not to exclude asymptomatic workers on basis of positive exercise test only ADA conflicts: May not be limited in performance of job Other issues in job assessment Statutory / Regulatory Dept. of Transportation (DOT) Commercial Driver’s License (CDL) exams • Exclusionary criteria: “Current” CAD accompanied (or likely to be) by angina, syncope, collapse or congestive heart failure Federal Aviation Administration (FAA) more stringent ADA • Accommodations • Direct threat Attribution and Workers’ Compensation Heart disease multifactorial: risk from work exposures is superimposed on a high baseline Firefighters, Police: Often a statutory presumption that CAD arose from work, if worker has required years of service Acknowledgments The author would particularly like to thank Glenn Pransky MD MOccH for the prior edition of this module as well as for photographs of rayon manufacture and retinal abnormalities Other photos courtesy National Archives and Library of Congress Beer photograph courtesy FreeFoto.com
Scaricare