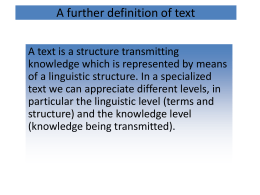
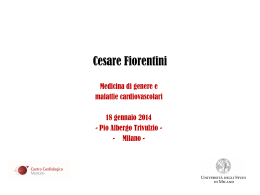
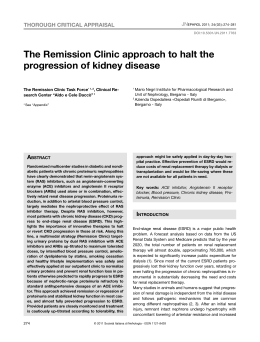
Calciphylaxis in a patient with POEMS syndrome without renal failure and/or hyperparathyroidism. A case report Ileana De Roma, Raffaele Filotico*, Michele Cea, Pasquale Procaccio, Federico Perosa POEMS (Crow-Fukase) syndrome is a rare plasma cell lymphoproliferative disorder associated with polyneuropathy (P), organomegaly (O), endocrinopathy (E), monoclonal (M) gammopathy and skin (S) abnormalities. The latter are usually not specific and include hyperpigmentation, hypertrichosis, cutaneous angioma and skin-thickening. A 45-year-old Italian woman was admitted to hospital because of muscle weakness, marked fatigue and paresthesia of the upper and lower extremities. Two and a half years earlier, a POEMS syndrome had been diagnosed on the basis of a history of organomegaly and mild lymphadenopathy, IgAλ monoclonal gammopathy, hypothyroidism, severe lower and upper limb sensory-motor peripheral neuropathy and a single osteosclerotic lesion in the left humerus. Eight weeks later, she developed skin lesions bioptically shown to be due to calciphylaxis-induced cutaneous vasculitis. To our knowledge, this is the first case of POEMS syndrome with this peculiar type of vasculitis. The absence of predisposing conditions, namely renal failure, hyperparathyroidism or clotting disorders renders the pathogenetic mechanism(s) of this severe type of vasculitis more intriguing. (Ann Ital Med Int 2004; 19: 283-287) Key words: Calciphylaxis; Monoclonal gammopathy; POEMS syndrome; Vasculitis. Introduction Case report POEMS (Crow-Fukase) syndrome1 is a rare plasma cell lymphoproliferative disorder presenting as osteosclerotic myeloma associated with polyneuropathy (P), organomegaly (O), endocrinopathy (E), monoclonal (M) gammopathy and skin (S) abnormalities2. The latter are usually not specific and include hyperpigmentation, hypertrichosis, cutaneous angioma and a sclerodermiform-like skin thickening. Additional skin abnormalities have also been observed as the result of cutaneous vasculitis and may vary in their clinical presentation from small-vessel hypersensitivity to necrotizing vasculitis2. Calciphylaxis is a vasculitis characterized by a systemic deposition of calcium salts in the small and medium-size vessels of end-renal stage patients3 or patients with hyperparathyroidism4. We here report a unique case of a patient with POEMS syndrome who developed calciphylaxis in the absence of predisposing conditions. The possible pathogenetic role of inflammatory cytokines, believed to be responsible for many signs and symptoms of POEMS syndrome, is briefly discussed. A 45-year-old Italian woman was admitted to our hospital in October 2003 with a 3-year history of autoimmune thyroiditis and hypothyroidism, weakness, fatigue, night sweats and weight loss in addition to a 1-year history of pleural effusion, ascites and sensory-motor neuropathy. In February 2001, a POEMS syndrome had been diagnosed on the basis of the following features: hepatosplenomegaly with ascites, a sensory-motor neuropathy defined both clinically and by sural nerve biopsy, IgAλ monoclonal gammopathy, a single osteosclerotic lesion and mild lymphadenopathy. At discharge, she was prescribed 75 mg/day prednisone that she continued until May 2002, when she spontaneously discontinued this therapy because of a worsening of her neurological symptoms. In September 2003, the onset of peripheral edema, ascites, dyspnea and renal failure led to her admission to an emergency department where she was treated with dopaminergics, plasma expanders and diuretics. After 3 weeks, her clinical picture and renal function improved and she was discharged on low doses of corticosteroids as maintenance therapy. However, because of continued worsening of her neurological symptoms and weight loss, she was admitted to our department in October 2003. Her history was negative for alcohol consumption and she was a non-smoker. She was cachectic, though not completely anorexic. She complained of marked asthenia. Her skin was brownish throughout and she also had severe Dipartimento di Scienze Biomediche e Oncologia Umana (Direttore: Prof. Franco Dammacco), *Dipartimento di Dermatologia (Direttore: Prof. Luigi Vena), Università degli Studi di Bari This work was supported by grants from the “Associazione Italiana per la Ricerca sul Cancro”, Milan, Italy and by a research grant from the University of Bari Medical School. © 2004 CEPI Srl 283 Ann Ital Med Int Vol 19, N 4 Ottobre-Dicembre 2004 muscle atrophy. A pitting lower limb edema (+-) was present. In addition, a mild systemic lymphadenopathy was detected with only one palpable 2-cm, left-supraclavicular lymph node, which was subsequently excised for biopsy. Her blood pressure was 110/80 mmHg on both arms. A grade 2 systolic murmur was audible on the aortic and pulmonary auscultation sites. The lungs were clear. The liver was palpable 2 cm below the right costal margin on the midclavicular line, and the spleen was enlarged to 3.5 cm below the left costal margin. Neurological examination confirmed the presence of paresthesia and a marked decrease of muscle strength rated as 4 of 5 for the lower and 2 of 5 for the upper extremities. The laboratory findings are summarized in table I. The hemoglobin level was 12 g/dL. The creatinine level was normal and the urea nitrogen was slightly increased. The erythrocyte sedimentation rate, conjugated and total bilirubin, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, serum calcium and phosphate were within normal limits. The fasting plasma glucose was 104 mg/dL and an oral glucose tolerance test was normal. The patient was negative for HBsAg and anti-hepatitis C virus. The prothrombin time was slightly prolonged, while the activated partial thromboplastin time was normal. Thyrotropin was increased, FT3 decreased, and FT4 in the normal range. Estrone levels were below the normal range. Calcitonin and parathyroid hormone levels were normal (Table I). Serum protein electrophoresis confirmed the presence of a monoclonal component characterized as IgAλ at immunoelectrophoresis. The serum IgA concentration was 523 mg/dL, whereas that of serum IgG was 487 mg/dL and the IgM levels were within the normal range. The levels of beta-2-microglobulin were increased. Urinalysis for proteinuria and free-light chains was unremarkable. Nested polymerase chain reaction (PCR) for human herpes virus 85 and qualitative PCR for hepatitis C virus were negative. Abdominal ultrasound revealed enlargement of liver and spleen without focal lesions, while the abdominal lymph nodes were of normal size. Systemic skeletal X-ray confirmed the presence of an osteosclerotic lesion in the proximal portion of the humerus. The rectal mucosa, on the other hand, was Congo red negative, though a widespread infiltration of plasma cells (λ 60% and κ 40%) was found. A similar (mostly λ) pattern was seen on a left latero-cervical lymph node biopsy, which also served to rule out Castleman’s disease. Eight weeks after our first observation, symmetrical livedo reticularis-like skin changes on the inner upper part of the thighs rapidly and locally extended to become painful and tender (Fig. 1 A and B). These lesions were initially cyanotic. After 1 week they became necrotic and TABLE I. Hematological, serum chemistry and hormone laboratory values on admission in October 2003. Variable Hemoglobin (g/dL) Hematocrit (%) White blood cells (mm3) Differential count (%) Neutrophils Lymphocytes Monocytes Platelets (mm3) MCV (µm3) Serum iron (µmol/L) Ferritin (µg/L) ESR (mm/h) PT (INR) aPTT (INR) Beta-2-microglobulin (mg/L) Total protein (g/L) Albumin Sodium (mmol/L) Potassium (mmol/L) Calcium (mmol/L) Phosphate (mmol/L) Creatinine (µmol/L) Urea nitrogen (mmol/L) Fasting plasma glucose (mg/dL) Thyrotropin (mUI/L) Free triiodothyronine (ng/L) Free thyroxine (ng/L) PTH (ng/L) Calcitonin (ng/L) Estrone (ng/L) Value (normal range) 12 (13-16.5) 36 (38-48) 8890 (4000-10 000) 70 (49-84) 24 (12-42) 6 (≤ 12) 357 000 (150 000-500 000) 83 (82-98) 4.83 (6.26-26.85) 55 (11-120) 14 (1-20) 1.4 (≤ 1.2) 0.94 (≤ 1.2) 5.2 (0.8-2) 50 (64-82) 32 (34-36) 138 (136-145) 4.7 (3.5-5.1) 2 (2-2.62) 0.96 (2.4-4.7) 70.72 (53.04-97.24) 31.48 (3.57-17.85) 104 (70-110) 6.06 (0.34-4.82) 0.89 (2.2-4.2) 10.3 (8.1-17.1) 11 (10-65) 4 (< 10) < 13 (14-103) aPTT = activated partial thromboplastin time; ESR = erythrocyte sedimentation rate; MCV = mean corpuscular volume; PT = prothrombin time; PTH = parathyroid hormone. resembled dry gangrene. Similar cyanotic lesions later developed above the pubis and on the back (Fig. 2), but did not progress to dry gangrene. Laboratory tests were performed, with particular emphasis on coagulation studies, proteins C and S and homocysteine, calcium/phosphate homeostasis as well as parathyroid hormone and calcitonin (Table II). All values were within the normal range apart from a slight homocysteine and creatinine increase. Biopsy, performed early following the appearance of the lesions, revealed occlusive vasculitis mostly involving the medium- and small-size vessels, with microthrombi and an impressively widespread calcification of the mediumand small-size vessel walls (Fig. 2), suggesting a calciphylaxis-induced cutaneous vasculitis. Mammography performed because of the appearance of pseudo-nodules in both breasts showed vascular calcification with an arborization-like pattern (Fig. 3). Indirect evidence of widespread calcification of the subcutaneous vessels was also observed at ultrasound in the form of hyperechogenic spots in the abdominal wall. 284 Ileana De Roma et al. FIGURE 1. Calciphylaxis-induced skin changes of the thighs (panels A and B) and dorsum (panel C). The thigh lesions evolved to dry gangrene. FIGURE 2. Histology of the skin biopsy specimen from the thighs taken soon after the appearance of the lesions. Periodic Acid-Schiff reagent (PAS) staining showing the presence of microthrombi in the small- (A) and medium-size vessels and calcium salt deposition in their walls (original magnification 200) (A and B). Recanalization of the occluded vessels may also be observed (arrows). case described here met the two major criteria (plasma cell dyscrasia and sensory-motor peripheral neuropathy) and more than one minor criterion (dark skin, hypothyroidism, osteosclerotic lesion, pleural effusion and/or ascites). The clinical spectrum of vasculitis described in this syndrome2,6-8 ranges from asymptomatic, small-vessel hypersensitivity-type vasculitis with complement and immune complex deposits disclosed by muscle and nerve biopsy6 to systemic necrotizing vasculitis8,9. In one report, however, vasculitis occurred in a POEMS patient with renal carcinoma7, which is known to be associated with paraneoplastic vasculitis. Calciphylaxis-induced cutaneous vasculitis is a rare disorder which mainly manifests in patients with endstage renal disease (1 to 4%)3 and is associated with a mortality of 60 to 80%. Proximal lesions (thighs and trunk) occur more often than distal ones (below the knee) and have a worse prognosis. Indeed, septicemia from infected lesions is the most frequent cause of death. Since the patient had only mild renal insufficiency, we explored addi- TABLE II. Reevaluation of the coagulation status and calcium-phosphate homeostasis following the development of calciphylaxis. Variable Value (normal range) Sodium (mmol/L) Potassium (mmol/L) Calcium (mg/dL) Phosphate (mg/dL) Creatinine (µmol/L) Urea nitrogen (mmol/L) PT (INR) aPTT (INR) C protein (%) S protein (%) Homocysteine (µmol/L) PTH (ng/L) Calcitonin (ng/L) 135 (136-145) 4.3 (3.5-5.1) 8.6 (8-10.5) 3.6 (2.5-4.9) 106.08 (53.04-97.24) 37.84 (3.57-17.85) 1.25 (≤ 1.2) 1.2 (≤ 1.2) 122 (67-140) 99 (62-145) 20.84 (5-15) 10 (10-65) 1.5 (< 10) Abbreviations as in table I. Discussion The major and minor criteria for the definition of POEMS syndrome have been previously outlined2 and the 285 Ann Ital Med Int Vol 19, N 4 Ottobre-Dicembre 2004 Riassunto La sindrome di POEMS (sindrome di Crow-Fukase) è un raro disordine linfoproliferativo associato a polineuropatia (P), organomegalia (O), endocrinopatia (E), gammopatia monoclonale (M) e manifestazioni cutanee (S). Queste ultime sono in genere aspecifiche e includono un ispessimento della cute con iperpigmentazione, ipertricosi ed angiomi cutanei. Una donna di 45 anni con sindrome di POEMS si ricovera nel nostro reparto per una rivalutazione della sua patologia e per una persistente debolezza muscolare associata a parestesie riferite alle estremità degli arti superiori ed inferiori. La sindrome di POEMS le era stata diagnosticata 30 mesi prima sulla base di un epatosplenomegalia, linfoadenomegalia, la presenza di una gammopatia IgAλ, ipotiroidismo, una marcata polineuropatia sensitivo-motoria ed una lesione osteosclerotica solitaria all’omero di sinistra. Otto settimane dopo la nostra prima osservazione, comparvero delle lesioni cutanee molto dolenti e ben delimitate che una biopsia rivelò essere dovute a calcifilassi. Questo rappresenta il primo caso di sindrome di POEMS associata a questo tipo di vasculite. L’assenza di condizioni predisponenti la calcifilassi quali l’insufficienza renale, l’iperparatiroidismo o disordini della coagulazione, sottolineano la complessità della patogenesi di questa vasculite a decorso infausto. FIGURE 3. X-ray of the mammary glands showing widespread calcification of the small- and medium-size vessels. tional factors reported to trigger or be associated with this vasculitis. Hypercoagulability10-12 was excluded because, apart from the prolongation of the prothrombin time and a slight increase in homocysteine levels, the activated partial thromboplastin time and the levels of the S and C proteins were normal. We also excluded calcium-phosphate dysfunction4,13,14 as the serum levels of parathyroid hormone, calcium and phosphate were normal. Finally, reports describing the onset of calciphylaxis in a patient with rheumatoid arthritis receiving immunosuppressive drugs for long periods of time15, suggest that the previous assumption of corticosteroids by our patient might have contributed to her calciphylaxis. Dysregulation of the secretion of pro-inflammatory cytokines, namely tumor necrosis factor (TNF)-α, interleukin (IL)-6, IL-1β and vascular endothelial growth factor (VEGF), has been suggested to explain many signs and symptoms related to POEMS syndrome16-18. Notably, increased levels of TNF-α and IL-6 with their osteoclastogenic properties may account for the osteolysis sometimes observed in this syndrome16. Increased levels of VEGF18 may account for the ascites, pleural effusion or cutaneous angioma often observed in these patients17. VEGF also displays osteoblastogenic properties19,20 and may be involved in the formation of osteosclerotic lesions17. Inasmuch as we found none of the known calciphylaxis-inducing conditions in our patient, we propose that a disequilibrium between TNF-α/IL-616 and VEGF20 levels, respectively with their osteoclastogenic and osteoblastogenic properties, may have induced calcium mobilization and calciphylaxis. Parole chiave: Calcifilassi; Gammopatia monoclonale; Sindorme di POEMS; Vasculite. Acknowledgments The authors are grateful to Mr. Vito Iacovizzi for his excellent secretarial assistance. References 01. Crow RS. Peripheral neuritis in myelomatosis. BMJ 1956; 12: 802-4. 02. Dispenzieri A, Kyle RA, Lacy MQ, et al. POEMS syndrome: definitions and long-term outcome. Blood 2003; 101: 2496-506. 03. Mazhar AR, Johnson RJ, Gillen D, et al. Risk factors and mortality associated with calciphylaxis in end-stage renal disease. Kidney Int 2001; 60: 324-32. 04. Khafif RA, DeLima C, Silverberg A, et al. Acute hyperparathyroidism with systemic calcinosis. Report of a case. Arch Intern Med 1989; 149: 681-4. 05. Belec L, Mohamed AS, Authier FJ, et al. Human herpesvirus 8 infection in patients with POEMS syndrome-associated multicentric Castleman’s disease. Blood 1999; 93: 3643-53. 06. Gherardi RK, Amiel H, Martin-Mondiere C, et al. Solitary plasmacytoma of the skull revealed by a mononeuritis multiplex associated with immune complex vasculitis. Arthritis Rheum 1989; 32: 1470-3. 07. Pasqui AL, Bova G, Saletti M, et al. POEMS syndrome with vascular lesions and renal carcinoma - possible role of cytokines. Eur J Med Res 1998; 3: 304-6. 286 Ileana De Roma et al. 08. Shibata M, Yamada T, Tanahashi N, et al. POEMS syndrome with necrotizing vasculitis: a novel feature of vascular abnormalities. Neurology 2000; 54: 772-3. 15. Korkmaz C, Dundar E, Zubaroglu I. Calciphylaxis in a patient with rheumatoid arthritis without renal failure and hyperparathyroidism: the possible role of long-term steroid use and protein S deficiency. Clin Rheumatol 2002; 21: 66-9. 09. Melikoglu M, Apaydin S, Hamuryudan V, et al. Calciphylaxis: a condition mimicking necrotizing vasculitis. Clin Rheumatol 1996; 15: 498-500. 16. Gherardi RK, Belec L, Soubrier M, et al. Overproduction of proinflammatory cytokines imbalanced by their antagonists in POEMS syndrome. Blood 1996; 87: 1458-65. 10. Mehta RL, Scott G, Sloand JA, et al. Skin necrosis associated with acquired protein C deficiency in patients with renal failure and calciphylaxis. Am J Med 1990; 88: 252-7. 17. Watanabe O, Arimura K, Kitajima I, et al. Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome. Lancet 1996; 347: 702. 11. Rostaing L, el Feki S, Delisle MB, et al. Calciphylaxis in a chronic hemodialysis patient with protein S deficiency. Am J Nephrol 1995; 15: 524-7. 18. Soubrier M, Dubost JJ, Serre AF, et al. Growth factors in POEMS syndrome: evidence for a marked increase in circulating vascular endothelial growth factor. Arthritis Rheum 1997; 40: 786-7. 12. Perez-Mijares R, Guzman-Zamudio JL, Payan-Lopez J, et al. Calciphylaxis in a haemodialysis patient: functional protein S deficiency? Nephrol Dial Transplant 1996; 11: 1856-9. 19. Midy V, Plouet J. Vasculotropin/vascular endothelial growth factor induces differentiation in cultured osteoblasts. Biochem Biophys Res Commun 1994; 199: 380-6. 13. Ahmed S, O’Neill KD, Hood AF, et al. Calciphylaxis is associated with hyperphosphatemia and increased osteopontin expression by vascular smooth muscle cells. Am J Kidney Dis 2001; 37: 1267-76. 20. Furumatsu T, Shen ZN, Kawai A, et al. Vascular endothelial growth factor principally acts as the main angiogenic factor in the early stage of human osteoblastogenesis. J Biochem (Tokyo) 2003; 133: 633-9. 14. Levin NW, Hoenich NA. Consequences of hyperphosphatemia and elevated levels of the calcium-phosphorus product in dialysis patients. Curr Opin Nephrol Hypertens 2001; 10: 563-8. Manuscript received on 15.10.2004; accepted on 26.10.2004. Address for correspondence: Prof. Federico Perosa, Sezione di Medicina Interna, Dipartimento di Scienze Biomediche e Oncologia Umana, Università degli Studi, Piazza Giulio Cesare 11, 70124 Bari. E-mail: [email protected] 287
Scaricare