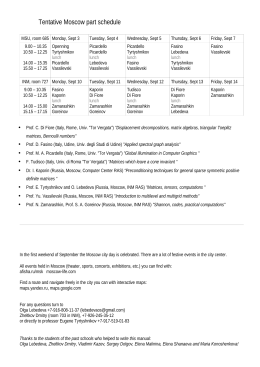
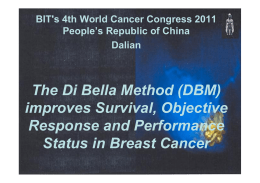
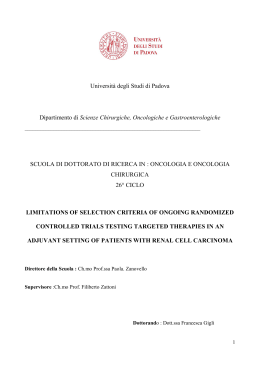
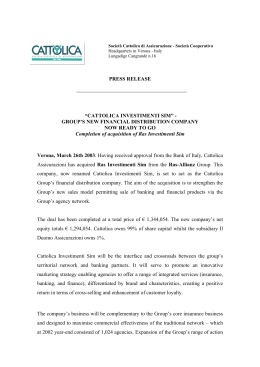
JNEPHROL 2011; 24 ( 03 ) : 274-281 THOROUGH CRITICAL APPRAISAL DOI:10.5301/JN.2011.7763 The Remission Clinic approach to halt the progression of kidney disease The Remission Clinic Task Force* 1, 2, Clinical Research Center “Aldo e Cele Daccò” 1 * See “Appendix” Abstract Randomized multicenter studies in diabetic and nondiabetic patients with chronic proteinuric nephropathies have clearly demonstrated that renin-angiotensin system (RAS) inhibitors, such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) used alone or in combination, effectively retard renal disease progression. Proteinuria reduction, in addition to arterial blood pressure control, largely mediates the nephroprotective effect of RAS inhibitor therapy. Despite RAS inhibition, however, most patients with chronic kidney disease (CKD) progress to end-stage renal disease (ESRD). This highlights the importance of innovative therapies to halt or revert CKD progression in those at risk. Along this line, a multimodal strategy (Remission Clinic) targeting urinary proteins by dual RAS inhibition with ACE inhibitors and ARBs up-titrated to maximum tolerated doses, by intensified blood pressure control, amelioration of dyslipidemia by statins, smoking cessation and healthy lifestyle implementation was safely and effectively applied at our outpatient clinic to normalize urinary proteins and prevent renal function loss in patients otherwise predicted to rapidly progress to ESRD because of nephrotic-range proteinuria refractory to standard antihypertensive dosages of an ACE inhibitor. This approach achieved remission or regression of proteinuria and stabilized kidney function in most cases, and almost fully prevented progression to ESRD. Provided patients are closely monitored and treatment is cautiously up-titrated according to tolerability, this 274 Mario Negri Institute for Pharmacological Research and Unit of Nephrology, Bergamo - Italy 2 Azienda Ospedaliera «Ospedali Riuniti di Bergamo», Bergamo - Italy 1 approach might be safely applied in day-by-day hospital practice. Effective prevention of ESRD would reduce costs of renal replacement therapy by dialysis or transplantation and would be life-saving where these are not available for all patients in need. Key words: ACE inhibitor, Angiotensin II receptor blocker, Blood pressure, Chronic kidney disease, Proteinuria, Remission Clinic Introduction End-stage renal disease (ESRD) is a major public health problem. A forecast analysis based on data from the US Renal Data System and Medicare predicts that by the year 2020, the total number of patients on renal replacement therapy will almost double, approximating 785,000, which is expected to significantly increase public expenditure for dialysis (1). Since most of the current ESRD patients progressively lost their kidney function over years, retarding or even halting the progression of chronic nephropathies is instrumental in substantially decreasing the need and costs for renal replacement therapy. Many studies in animals and humans suggest that progression of renal damage is independent from the initial disease and follows pathogenic mechanisms that are common among different nephropathies (2, 3). After an initial renal injury, remnant intact nephrons undergo hypertrophy with concomitant lowering of arteriolar resistance and increased © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 JNEPHROL 2011; 24 ( 03 ) : 274-281 glomerular plasma flow (4). Since the tone of afferent arterioles drops more than that of efferent ones, hydraulic pressure of glomerular capillaries rises, increasing the filtrate per nephron. These changes enhance the filtration capacity of remaining nephrons to minimize the functional consequences of their reduced number, but they are ultimately detrimental. Indeed, the high intraglomerular capillary pressure enlarges the radii of glomerular pores and, along with podocyte cytoskeleton rearrangement secondary to increased angiotensin II levels, impairs the size selectivity of the membrane and induces protein ultrafiltration (4, 5). An excess of proteins in the lumen of the tubules eventually results in a nephritogenic effect, through a direct tubular toxicity and a secondary process of tubular epithelial endocytosis (2, 6). On the basis of this background, reduction of protein traffic, along with strict blood pressure (BP) control, should play a central role in intervention strategies aimed to prevent or revert renal disease progression. In animals, renin-angiotensin system (RAS) blockers reduce intraglomerular hydraulic pressure and improve the selectivity of the glomerular barrier, an effect that translates into a reduction of proteinuria and prevention of glomerulosclerosis and kidney scarring (3). Prospective randomized placebo-controlled trials found that, at comparable BP control, angiotensin-converting enzyme (ACE) inhibitors (7) are more effective than non-ACE inhibitor therapy in limiting progression to ESRD in diabetic and nondiabetic patients with chronic proteinuric nephropathies (8). Notably, the Ramipril Efficacy In Nephropathy (REIN) trial found that reduction in urinary protein excretion rate with the ACE inhibitor ramipril was the only time-dependent covariate that predicted a lower rate of glomerular filtration rate (GFR) decline and progression to ESRD in patients with nondiabetic chronic nephropathies, clearly indicating that reduction of protein traffic is renoprotective (9). Hence, minimizing urinary protein excretion should represent the primary goal to retard/stabilize renal progression of chronic renal disease. Dual RAS inhibition: a strategy to maximize antiproteinuric effect of ACE inhibitors and angiotensin II receptor blockers The combination of an ACE inhibitor and angiotensin II receptor blockers (ARBs) has been suggested as a way to maximize RAS inhibition by affecting both the bioavailability of angiotensin II through ACE inhibition and also its activity at the receptor level. Moreover, an ACE inhibitor may prevent the compensatory increase in angiotensin II synthesis frequently observed during ARB therapy. On the other hand, an ARB may inhibit the activity of angiotensin II produced via ACE-independent pathways. Animal (10, 11) and human (12, 13) studies have consistently found that ACE inhibitors and ARBs in combination reduce proteinuria more effectively than the 2 agents alone (14). Of note, a meta-analysis of 425 patients with chronic proteinuric nephropathies found that the reduction achieved by dual RAS inhibition exceeded the reduction achieved by ACE inhibitors or ARB therapy alone, by 60% and 54%, respectively (15). In these studies, however, dual RAS blockade had a more consistent antihypertensive effect than single ACE inhibitor or ARB therapy, which did not allow the studies to address the issue of whether the superior antiproteinuric effect of combined therapy really reflected more effective RAS blockade or, rather, was just a function of more BP reduction. To address this issue, the antiproteinuric effect of fixed doses of the ACE inhibitor benazepril and of the ARB valsartan given alone were compared with that of halved doses of the 2 drugs used in combination in a cross-over study in patients with nondiabetic chronic kidney disease (16). With this approach, BP reduction was similar in the 3 treatment groups, but proteinuria reduction was more consistent with dual therapy. This provided evidence that the superior antiproteinuric effect of dual compared with single-drug RAS blockade was not explained by a higher antihypertensive effect, but by a more effective inhibition of the RAS (16). On the basis of these results, patients were maintained on dual RAS inhibitor therapy (benazepril 10 mg/day plus valsartan 80 mg/day) and prospectively followed up. Their outcome at 6 years was compared with that of matched reference patients maintained on single-drug RAS blockade with a full dose of an ACE inhibitor (ramipril 5 mg/day). Decline of estimated GFR (eGFR) was significantly lower in patients compared with reference patients (Fig. 1), and proteinuria reduction independently predicted the rate of eGFR decline. In patients, GFR (measured by iohexol clearance), filtration fraction, renal vascular resistances and urinary protein to creatinine ratio decreased at 1 year, were stable up to 6 years and recovered to baseline after treatment withdrawal. No patient versus 6 reference patients (log-rank test: p=0.01) had a renal or cardiovascular event (2 reference patients suffered a myocardial infarction, 1 stroke, 1 heart failure, 1 ESRD and 1 a doubling of serum creatinine plus ESRD). Notably, there were no drug-related adverse events. These data confirm and extend evidence that in patients with proteinuric nephropathies, dual RAS blockade is the most efficient way to reduce proteinuria and therefore slow or even halt the progression of chronic kidney disease (3, © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 275 Ruggenenti et al: The Remission Clinic Fig. 1 - Change in estimated glomerular filtration rate (ΔeGFR) over 6 years of follow-up in 20 nondiabetic patients with chronic proteinuric nephropathies on angiotensin-converting enzyme (ACE) inhibitor (benazepril, 10 mg/day) plus angiotensin II receptor blocker (ARB) (valsartan, 80 mg/day) therapy and in 20 reference patients on ACE inhibitor therapy alone (ramipril, 10 mg/day). Physiological decline of eGFR for patients over 40 years of age is -0.1 ml/min per 1.73 m2 per month (17). Data are medians with interquartile range. 17). Conversely, dual RAS blockade is not expected to confer any additional renoprotective effect as compared with ACE inhibitors or ARB therapy alone and even compared with non-RAS inhibitor therapy in patients without proteinuria (18). Analyses of the REIN study results found that most of the protective effect of RAS inhibition against progressive renal function loss is seen in patients with heavy proteinuria to start with (19). It progressively wanes at decreasing levels of proteinuria and tends to vanish when 24hour proteinuria ranges between 1 and 2 g (Fig. 2). At lower levels of proteinuria, no specific protective effect of RAS inhibitor therapy against renal disease progression is expected. This is consistent with trials of ACE inhibitor therapy in patients with chronic kidney disease, but cases with a 24hour urinary protein excretion rate lower than 1 g showed no appreciable treatment effect in this population (20, 21). Actually, patients with nonproteinuric renal disease are expected to have no specific advantages in term of nephroprotection from ACE inhibitor or ARB therapy and, at the same time, are exposed to the risks of RAS inhibition such as hyperkalemia and acute renal function deterioration (22), events that may be particularly frequent in elderly subjects and in patients with type 2 diabetes and concomitant kidney vascular disease (23). These risks are even increased when RAS inhibition is maximized by ACE inhibition and 276 ARB combination therapy. Thus, safety concerns raised by the results of the Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET) (18) were largely expected. This study assigned 25,620 patients with established atherosclerotic vascular disease or diabetes with end-organ damage to the ACE inhibitor ramipril, the ARB telmisartan, or a combination of the 2. Over 56 months, the incidence of cardiovascular events was similar in the 3 treatment groups, as well as the incidence of ESRD or doubling of serum creatinine. Indeed, renal events were extremely rare in all groups, which reflected the remarkably slow rate of renal function loss that, independent of treatment allocation, was close to that observed in the general population as an effect of aging (24). This can be largely explained by the fact that only 4% of patients had overt proteinuria and, in turn, may also explain why RAS inhibitor therapy did not appear to affect renal outcomes in this population. Conversely, the need for acute dialysis to treat acute renal function deterioration and/or hyperkalemia was more frequent in patients on dual RAS blockade than in those on ACE inhibitor or ARB therapy alone. This conceivably reflected transient kidney hypoperfusion in patients with excessive BP reduction, hypovolemia or ischemic kidney disease that improved with treatment withdrawal. Thus, it was a treatment-related adverse effect facilitated © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 JNEPHROL 2011; 24 ( 03 ) : 274-281 Fig. 2 - Rate of glomerular filtration rate (GFR) decline in 352 patients with nondiabetic proteinuric nephropathies included in the REIN trial according to treatment and range of 24-hour proteinuria at baseline. The 2 equations describe the curves interpolating the points showing GFR decline within each treatment group (solid circles for ramipril and empty circles for non-RASinhibiting antihypertensive therapy) at different ranges of proteinuria. Dashed circles show the estimated GFR declines for patients with proteinuria <1 g per 24 hours. RAS = renin-angiotensin system. by maximized RAS inhibition and could not be considered as a renal outcome related to proteinuria or renal disease progression (19). The Remission Clinic approach Experimental and clinical data converge to indicate that optimal BP control and maximized RAS inhibition are key components of nephroprotective strategy in patients with proteinuric chronic nephropathies. Other tools are, however, available to further decrease proteinuria and improve renal outcomes in those patients with persistent urinary protein loss. Indeed, evidence has been provided that hydroxymethylglutaryl-CoA reductase inhibitors (statins) may reduce proteinuria regardless of their effect on serum lipids (25), though their antiproteinuric effect has been recently questioned (26, 27). Low salt intake, smoking cessation and optimal metabolic control in diabetics represent other crucial tools to retard progression of chronic nephropathies. Analogous to cancer and AIDS therapy, where the integrated use of different treatments against the same target, such as uncontrolled cell or viral replication, has dramatically improved patients’ outcomes, experimental data suggest that combined therapies targeted to proteinuria reduction may further retard renal disease progression as compared with single treatments (10). This formed the rationale for the establishment of a multimodal intervention strategy, the “Remission Clinic” program, using all available pharmacological tools and lifestyle rules to reduce urinary proteins in patients with chronic renal disease and heavy proteinuria despite ACE inhibitor therapy (28). Each step of the Remission Clinic protocol is implemented according to a predefined sequence until 24-hour proteinuria is consistently lower than 0.3 g or the protocol has to be stopped because of safety/tolerability reasons. The first step consists in the administration of a fixed dosage (5 mg/day) of ramipril or of an equivalent dosage of any other ACE inhibitor. When tolerated, the dosage is uptitrated to full antihypertensive dosage, and thereafter a fixed dosage (50 mg/day) of losartan or an equivalent dosage of another ARB is added on and progressively up-titrated to full antihypertensive dosage. Then patients © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 277 Ruggenenti et al: The Remission Clinic are maintained on dual RAS blockade, with ramipril and losartan doses progressively up-titrated to maximum tolerated dosages or with full remission of proteinuria (24hour urinary protein excretion <0.3 g) is achieved. A statin is also prescribed independently from cholesterol levels, to further reduce proteinuria (29) and limit the excess cardiovascular risk in this population. Patients are recommended a low-sodium diet (30) with a controlled (0.8 g/kg body weight per day) protein content and are invited to refrain from smoking. Strict metabolic control is recommended to patients with diabetes. Adjustments of antihypertensive agents are allowed to target BP ≤120/80 mm Hg without inducing symptomatic hypotension. Diastolic BP should not be reduced to less than 60 mm Hg, to avoid an excess cardiovascular risk possibly associated with target organ hypoperfusion. Thiazide (if serum creatinine ≤1.4 mg/dL) or loop (if serum creatinine >1.4 mg/dL) diuretics are first-line therapy to target BP, prevent hyperkalemia and/or control edema. Aldosterone antagonists may help to further reduce urinary proteins (31, 32), but are associated with an increased risk of life-threatening hyperkalemia, in particular in elderly patients and in those with diabetes and more severe renal insufficiency (24), and thus these must be used with caution and under close patient monitoring. Alpha or beta-blockers (in case of an heart rate >60 bpm), along with nondihydropyridine calcium channel blockers (CCB) are second-line therapy (33). Dihydropyridine CCB are used for safety reasons in those with BP >140/90 mm Hg despite the other treatments, as evidence exists that they may increase proteinuria and accelerate loss of renal function. Minoxidil is considered as rescue therapy. The Remission Clinic program has been applied since 1999 to all consecutive patients who were referred to the Bergamo Nephrological Outpatient Clinic because of chronic renal disease and heavy proteinuria despite ACE inhibitor therapy (28). The Remission Clinic approach in day-by-day clinical practice To assess the safety/efficacy profile of the Remission Clinic strategy, the rate of eGFR decline and the incidence of ESRD in a cohort of 56 patients with chronic proteinuric nephropathies treated according to this approach were compared with outcomes of 56 matched historical reference patients who had received ACE inhibitor therapy titrated to target BP (28). Over a median follow-up of 4 years, the median monthly rate of eGFR decline was significantly lower in the Remission Clinic 278 cohort (−0.17 vs. −0.56 ml/min per 1.73 m2; p<0.0001), and ESRD events were significantly reduced (Fig. 3) compared with the reference cohort. Follow-up BP, cholesterol and proteinuria were lower in Remission Clinic patients than in reference subjects, and disease remission or regression was achieved in up to 50% of patients who would have been otherwise expected to progress rapidly to ESRD on conventional therapy. Proteinuria reduction independently predicted a lower rate of eGFR decline and ESRD incidence, further highlighting its crucial pathogenic role in renal disease progression. Importantly, therapy was well tolerated, and no patient was withdrawn because of hyperkalemia (28). This was the first evidence that a multidrug treatment titrated to urinary protein level can be safely and effectively applied to normalize proteinuria and to slow the loss of renal function in day-by-day clinical practice. Importantly, this study also pointed out the importance of the early beginning of nephroprotective strategies. Indeed, in patients with overt diabetic nephropathy, response to Remission Clinic therapy was incomplete, in line with experimental evidence that ACE inhibitor treatment has limited efficacy in advanced phases of diabetic nephropathy (34). A potential explanation is that renal structural changes in these patients are so advanced and diffuse that they prevent pharmacological treatments from achieving the desired effect on proteinuria and disease progression. Experimental data show that RAS inhibitor therapy may fully prevent renal lesions of diabetes when treatment is started early, at induction of diabetes, but is marginally affected when RAS inhibition is started when structural changes are already severe (34). The findings that in the Bergamo Nephrologic Diabetes Complications Trial (BENEDICT), ACE inhibitor therapy with trandolapril delayed the onset of microalbuminuria – taken as an early marker of renal disease and a major risk factor for cardiovascular events – in patients with type 2 diabetes, arterial hypertension and normoalbuminuria can be taken to suggest that early intervention, before overt nephropathy is established, is needed in people with diabetes to maximize renoprotection (35). The potential large-scale impact of the Remission Clinic approach Hopefully, extension of the Remission Clinic approach to clinical practice will translate into a reduced incidence of new patients requiring renal replacement therapy, with an obvious economical benefit for health care systems (http://clinicalweb.marionegri.it/remission/index.php). © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 JNEPHROL 2011; 24 ( 03 ) : 274-281 Fig. 3 - Cumulative incidence of end-stage renal disease (ESRD) in 56 patients with chronic proteinuric nephropathies treated according to a multidrug treatment titrated to urinary proteins (the Remission Clinic approach) and 56 matched reference patients receiving a conventional angiotensinconverting enzyme (ACE) inhibitor treatment titrated to blood pressure. HR = hazard ratio. This would be of utmost importance especially for developing countries, where dialysis and kidney transplantation are available only for a small minority of patients in need. In these countries, 10% to 20% of subjects are estimated to be at risk of ESRD (36), and effective renoprotection could be life-saving in a large fraction of this population. Availability of out-of-patent drugs in a fixed combination (polypill) (37), in addition to enhancing patient compliance, would dramatically reduce treatment costs, allowing implementation of cost-effective programs of prevention and treatment of renal disease, in particular in limited resource settings. Appendix Financial support: None. Conflict of interest statement: None. Address for correspondence: Piero Ruggenenti, MD “Mario Negri” Institute for Pharmacological Research Centro Anna Maria Astori Science and Technology Park Kilometro Rosso Via Stezzano, 87 IT-24126 Bergamo, Italy [email protected] References 1. The remission clinic task force 2. Coordination: Piero Ruggenenti, Andrea Remuzzi, Giuseppe Remuzzi. Patient selection and care: Elena Perticucci, Roberto Trevisan, Alessandro Dodesini. Data handling and monitoring: Vincenzo Gambara, Bogdan Ene-Iordache, Sergio Carminati, Nadia Rubis, Giulia Gherardi. Data analysis: Annalisa Perna, Paolo Cravedi. 3. 4. United States Renal Data System (USRDS), Annual Data Report 2007:92. Abbate M, Zoja C, Remuzzi G. How does proteinuria cause progressive renal damage? J Am Soc Nephrol. 2006;17:2974-2984. Remuzzi G, Benigni A, Remuzzi A. Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes. J Clin Invest. 2006;116:288-296. Ruggenenti P, Perna A, Mosconi L, Pisoni R, Remuzzi G; Gruppo Italiano di Studi Epidemiol. Urinary protein excre- © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 279 Ruggenenti et al: The Remission Clinic 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 280 tion rate is the best independent predictor of ESRF in nondiabetic proteinuric chronic nephropathies. Gruppo Italiano di Studi Epidemiologici in Nefrologia (GISEN). Kidney Int. 1998;53:1209-1216. Macconi D, Abbate M, Morigi M, et al. Permselective dysfunction of podocyte-podocyte contact upon angiotensin II unravels the molecular target for renoprotective intervention. Am J Pathol. 2006;168:1073-1085. Remuzzi G, Bertani T. Pathophysiology of progressive nephropathies. N Engl J Med. 1998;339:1448-1456. Cravedi P, Ruggenenti P, Remuzzi G. Intensified inhibition of renin-angiotensin system: a way to improve renal protection? Curr Hypertens Rep. 2007;9:430-436. Campbell RC, Ruggenenti P, Remuzzi G. Halting the progression of chronic nephropathy. J Am Soc Nephrol. 2002;13(Suppl 3):S190-S195. The GISEN Group (Gruppo Italiano di Studi Epidemiologici in Nefrologia). Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. Lancet. 1997;349:1857-1863. Zoja C, Corna D, Camozzi D, et al. How to fully protect the kidney in a severe model of progressive nephropathy: a multidrug approach. J Am Soc Nephrol. 2002;13:2898-2908. Cao Z, Bonnet F, Davis B, Allen TJ, Cooper ME. Additive hypotensive and anti-albuminuric effects of angiotensin-converting enzyme inhibition and angiotensin receptor antagonism in diabetic spontaneously hypertensive rats. Clin Sci (Lond). 2001;100:591-599. Russo D, Minutolo R, Pisani A, et al. Coadministration of losartan and enalapril exerts additive antiproteinuric effect in IgA nephropathy. Am J Kidney Dis. 2001;38:18-25. Mogensen CE, Neldam S, Tikkanen I, et al. Randomised controlled trial of dual blockade of renin-angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: the candesartan and lisinopril microalbuminuria (CALM) study. BMJ. 2000;321:1440-1444. Taal MW, Brenner BM. Combination ACEI and ARB therapy: additional benefit in renoprotection? Curr Opin Nephrol Hypertens. 2002;11:377-381. Catapano F, Chiodini P, De Nicola L, et al. Antiproteinuric response to dual blockade of the renin-angiotensin system in primary glomerulonephritis: meta-analysis and metaregression. Am J Kidney Dis. 2008;52:475-485. Campbell R, Sangalli F, Perticucci E, et al. Effects of combined ACE inhibitor and angiotensin II antagonist treatment in human chronic nephropathies. Kidney Int. 2003;63:10941103. Ruggenenti P, Schieppati A, Remuzzi G. Progression, remission, regression of chronic renal diseases. Lancet. 2001;357:1601-1608. Mann JF, Schmieder RE, McQueen M, et al; ONTARGET investigators. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. a multicentre, randomised, double-blind, controlled trial. Lancet. 2008;372:547-553. Ruggenenti P, Remuzzi G. Proteinuria: Is the ONTARGET renal substudy actually off target? Nat Rev Nephrol. 2009;5:436437. Maschio G, Alberti D, Janin G, et al; The Angiotensin-Converting-Enzyme Inhibition in Progressive Renal Insufficiency Study Group. Effect of the angiotensin-converting-enzyme inhibitor benazepril on the progression of chronic renal insufficiency. N Engl J Med. 1996;334:939-945. Locatelli F, Carbarns IR, Maschio G, et al; The AngiotensinConverting-Enzyme Inhibition in Progressive Renal Insufficiency Study Group. Long-term progression of chronic renal insufficiency in the AIPRI Extension Study. Kidney Int Suppl. 1997;63:S63-S66. Ruggenenti P, Cravedi P, Remuzzi G. Proteinuria: increased angiotensin-receptor blocking is not the first option. Nat Rev Nephrol. 2009;5:367-368. Takaichi K, Takemoto F, Ubara Y, Mori Y. Analysis of factors causing hyperkalemia. Intern Med. 2007;46:823-829. Davies DF, Shock NW. Age changes in glomerular filtration rate, effective renal plasma flow, and tubular excretory capacity in adult males. J Clin Invest. 1950;29:496-507. Sandhu S, Wiebe N, Fried LF, Tonelli M. Statins for improving renal outcomes: a meta-analysis. J Am Soc Nephrol. 2006;17:2006-2016. Conley J, Olafsson A, Djamali A. Do statins delay the incidence of ESRD in diabetic patients with moderate CKD? J Nephrol. 2010;23:321-327. Ruggenenti P, Perna A, Tonelli M, et al. Effects of add-on fluvastatin therapy in patients with chronic proteinuric nephropathy on dual renin-angiotensin system blockade: The ESPLANADE Trial. Clin J Am Soc Nephrol. 2010;5:1928-1938. Ruggenenti P, Perticucci E, Cravedi P, et al. Role of remission clinics in the longitudinal treatment of CKD. J Am Soc Nephrol. 2008;19:1213-1224. Bianchi S, Bigazzi R, Caiazza A, Campese VM. A controlled, prospective study of the effects of atorvastatin on proteinuria and progression of kidney disease. Am J Kidney Dis. 2003;41:565-570. Heeg JE, de Jong PE, van der Hem GK, de Zeeuw D. Efficacy and variability of the antiproteinuric effect of ACE inhibition by lisinopril. Kidney Int. 1989;36:272-279. Bianchi S, Bigazzi R, Campese VM. Long-term effects of spironolactone on proteinuria and kidney function in patients with chronic kidney disease. Kidney Int. 2006;70:21162123. Perico N, Benigni A, Remuzzi G. Present and future drug treatments for chronic kidney diseases: evolving targets in renoprotection. Nat Rev Drug Discov. 2008;7:936-953. Egan CG, Pontremoli R. Role of the fixed-dose combination lercanidipine-enalapril in renal protection. J Nephrol. 2011 Jan 24 (Epub ahead of print). Perico N, Amuchastegui SC, Colosio V, Sonzogni G, Bertani © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 JNEPHROL 2011; 24 ( 03 ) : 274-281 T, Remuzzi G. Evidence that an angiotensin-converting enzyme inhibitor has a different effect on glomerular injury according to the different phase of the disease at which the treatment is started. J Am Soc Nephrol. 1994;5:1139-1146. 35. Ruggenenti P, Fassi A, Ilieva AP, et al; Bergamo Nephrologic Diabetes Complications Trial (BENEDICT) Investigators. Preventing microalbuminuria in type 2 diabetes. N Engl J Med. 2004;351:1941-1951. 36. Codreanu I, Perico N, Sharma SK, Schieppati A, Remuzzi G. Prevention programmes of progressive renal disease in developing nations. Nephrology (Carlton). 2006;11:321-328. 37. Yusuf S, Pais P, Afzal R, et al; Indian Polycap Study (TIPS). Effects of a polypill (Polycap) on risk factors in middle-aged individuals without cardiovascular disease (TIPS): a phase II, double-blind, randomised trial. Lancet. 2009;373:13411351. Accepted: March 18, 2011 © 2011 Società Italiana di Nefrologia - ISSN 1121-8428 281
Scaricare