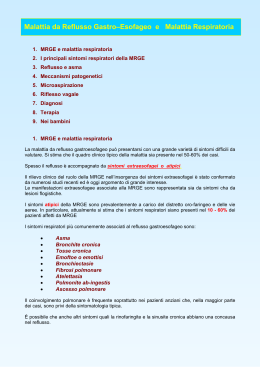
IL REFLUSSO GASTROESOFAGEO E LA MALATTIA DA REFLUSSO GASTROESOFAGEO Annamaria Staiano Dipartimento di Scienze Mediche Traslazionali Università “Federico II” Napoli, Italia Pediatric GERD and acid-related conditions (ARC): trends in incidence of diagnosis and acid suppression therapy • Between 2000 and 2005, annual incidence of GERD/ARC diagnosis among infants (age ≤1 year) more than tripled (from 3.4 to 12.3%) and increased by 30% to 50% in other age groups. • Patients diagnosed by GI specialists (9.2%) were more likely to be treated with PPIs compared to patients diagnosed by primary care physician (PCP). PPI-initiated patients doubled 1999 31.5% 2005 62.6% when compared with H²RA-initiated patients associated with 30% less discontinuation 90% less therapy switching in 1st month higher comorbidity burden pre-treatment total HCU costs when diagnosed 2 Nelson SP. J Med Eco 2009;12:348-55 19-12-2015 Il reflusso gastroesofageo (RGE) • Il reflusso gastroesofageo (RGE) è un fenomeno fisiologico che si verifica in lattanti, bambini e adulti. • Il reflusso fisiologico si presenta solitamente in circa il 70% dei lattanti di 4 mesi di età. • Nella maggior parte dei lattanti il RGE non causa alcun sintomo. “PREVALENCE AND NATURAL HISTORY OF GASTROESOPHAGEAL REFLUX: PEDIATRIC PROSPECTIVE SURVEY” (1/2) • A detailed questionnaire was completed by 59 primary care pediatricians . • 2642 patients (0-12 months) were prospectively enrolled during a 3-month period. • Follow-up at 6, 12, 18 and 24 months of age Campanozzi A. Pediatrics 2009 “PREVALENCE AND NATURAL HISTORY OF GASTROESOPHAGEAL REFLUX: PEDIATRIC PROSPECTIVE SURVEY” (2/2) • 313 infants (12%; 147 girls) affected by infant regurgitation. • Vomiting in 34/313 patients (10.9%). • • • • • Follow-up in 210/313: regurgitation disappeared 56 (27%) at 6 months 128 (61%) at 12 months 23 (11%) at 18 months 3 (1%) at 24 months • Organic disease in 2/210 (0.1%) Campanozzi A. Pediatrics 2009 WHEN GER CAUSES TROUBLESOME SYMPTOMS OR COMPLICATIONS IT IS DEFINED AS GER DISEASE (GERD). Am J Gastroenterol 2009 IN PEDIATRIC PATIENTS, ESOPHAGEAL COMPLICATIONS OF GERD ARE REFLUX ESOPHAGITIS, HEMORRHAGE, STRICTURE, BARRETT’S ESOPHAGUS, AND, RARELY ADENOCARCINOMA. Am J Gastroenterol 2009 2 COME DIAGNOSTICARE LA MRGE: MANIFESTAZIONI GASTRO-INTESTINALI MANIFESTAZIONI RESPIRATORE COME DIAGNOSTICARE LA MRGE: LE MANIFESTAZIONI GASTROINTESTINALI E RESPIRATORE “Non c’è evidenza nel prescrivere trial farmacologici empirici in lattanti e bambini piccoli con sintomi suggestivi di MRGE (Evidenza B) J Pediatr Gastroenterol Nutr 2009; 49:498-547 •162 infants with crying, regurgitation, refuse feed, coughing •Treatment with lansoprazole or placebo for 4 weeks •44/81 infants (54%) in each group were responders, identical for lansoprazole and placebo •Serious adverse events, expecially lower respiratory tract infections, more frequently in the lansoprazole group compared with the placebo group Orenstein SR et al. J Pediatr 2009; 154: 514-20 “STOP THE PPI EXPRESS: THEY DON'T KEEP BABIES QUIET” • Dramatic increase in the use of PPIs in infants (4-fold between 2000 and 2003), but with no evidence suggesting a change in the incidence of GERD • PPIs have become the modern effector in the old instruction to “take two aspirins and call me in the morning” in clinical practice • Given the increasing evidence that they offer little benefit for some of the symptoms for which they are prescribed, a serious effort to curtail their empiric use is warranted Putnam PE. J Pediatr 2009; 154 (4); 514-520 Trends of outpatient prescription drug utilization in US children, 2002-2010. Chai G. Pediatrics 2012;130:23-31 12 19-12-2015 12/19/2015 Introduction Symptoms Prevalence Diagnosis Treatment Colusion Efficacy and safety of once-daily esomeprazole for the treatment of GERD in neonatal patients. There were no significant differences between the esomeprazole and placebo groups in the percentage change from baseline in the total number of GERD-related signs and symptoms (-14.7% vs -14.1%, respectively). Mean change from baseline in total number of reflux episodes was not significantly different between esomeprazole and placebo (-7.43 vs -0.2, respectively); however, the percentage of time pH was <4.0 and the number of acidic reflux episodes >5 min in duration was significantly decreased with esomeprazole vs placebo (-10.7 vs 2.2 and -5.5 vs 1.0, respectively; P ≤ .0017). The number of patients with adverse events was similar between treatment groups. Signs and symptoms of GERD traditionally attributed to acidic reflux in neonates were not significantly altered by esomeprazole treatment. Esomeprazole was well tolerated and reduced esophageal acid exposure and the number of acidic reflux events in neonates. Davidson G. J Pediatr. 2013;163:692-698.e2 Development of food allergies in patients with GERD treated with gastric acid suppressive medications. Children with GERD who were treated with GAS were more likely to be diagnosed with a food allergy (Hazard ratio (HR): 3.67, 95% CI 2.15-6.27), as were children with GERD diagnosis but who were not treated with GAS medications (HR: 2.15, 95% CI: 1.21-3.81). A direct comparison of the two GERD cohorts showed that children with GERD who were treated with GAS had a greater risk of food allergy than those with GERD who were untreated (HR, 1.68, 95%CI, 1.15-2.46). Trikha A. Pediatr Allergy Immunol. 2013;24:582-8 POTENZIALI RISCHI DEGLI INIBITORI DI POMPA PROTONICA (IPP) • Gli effetti collaterali attribuibili agli IPP tra cui cefalea, diarrea, costipazione, nausea si verificano negli adulti fino al 14% dei casi • Aumento del rischio di polmonite acquisita in comunità e gastroenterite acuta nei bambini e negli adulti trattati con IPP • Aumento del rischio di candidemia e di NEC nei neonati prematuri trattati con terapia acido-soppressiva • Nefrite interstiziale • Possibile aumento del rischio di infezione da C. Difficile e di fratture dell'anca negli adulti trattati cronicamente con IPP COME DIAGNOSTICARE LA MRGE: LE MANIFESTAZIONI GASTRO-INTESTINALI E RESPIRATORE « Nei bambini più grandi e negli adolescenti con bruciore e dolore retrosternale, un trial terapeutico con acido inibitori può essere utile per determinare se il reflusso è la causa dei sintomi» (Evidenza C) MANIFESTAZIONI EXTRAINTESTINALI DI MRGE • POLMONITI RICORRENTI • PATOLOGIA LARINGEA • SINUSITE • OTITE MEDIA E OTALGIA • EROSIONI DENTALI • APNEA • ASMA E TOSSE CRONICA PATOLOGIA LARINGEA A B D C E The data linking reflux to chronic hoarseness, chronic cough, sinusitis, chronic otitis media, erythema, and cobblestone appearance of the larynx come mainly from case reports and case series. • In children, based on current data, PPIs should not be used empirically. • The single relatively large high quality study on the utility of PPI for cough associated with GORD found no beneficial effect in infants and those on lansoprazole had significantly increased serious adverse events, in particular lower respiratory infections. • Data on milk modification for infants and cough with GORD is insufficient to make specific recommendations. • Until more evidence is available in the form of well-designed RCTs, other causes of cough should be considered in children with cough and GORD, prior to any consideration of empiric treatment with a prolonged course of GORD medications/interventions. Cochrane Database of Systematic Reviews 2011, Issue 1. Art. No.: CD004823. DOI: 10.1002/14651858.CD004823.pub4. Gastroesophageal reflux disease and childhood asthma. Clinical studies show that GERD is highly prevalent in children with asthma, with estimates as high as 80%, but nearly half of the children are asymptomatic. However, there is no conclusive evidence per se that asymptomatic GERD informs asthma control, and treatment of GERD in the few controlled trials available for review does not substantively improve asthma outcomes. In a recent large controlled clinical trial, treatment with a PPI was not only ineffective, but adverse effects were common, including an increased prevalence of symptomatic respiratory infections. Current evidence does not support the routine use of anti-GERD medication in the treatment of poorly controlled asthma of childhood. Blake K. Curr Opin Pulm Med. 2013;19:24-9 Michele Ghezzi, Michela Silvestri, Edoardo Guida, Angela Pistorio,Oliviero Sacco, Girolamo Mattioli, Vincenzo Jasonni,Giovanni A.Rossi Respiratory Medicine (2011) 105, 972e978 Effect of proton pump inhibition on acid, weakly acid and weakly alkaline GER in children. 90 80 70 60 non-acid weakly acid acid 50 40 30 20 10 0 before therapy on therapy Turk H. World J Pediatr. 2013;9:36-41 Higher rate of bronchoalveolar lavage culture positivity in children with nonacid reflux and respiratory disorders. • ? children with chronic cough or wheezing and with more full-column, nonacid reflux have a higher likelihood of a positive BAL fluid culture • 46 children with cough patients who had a positive culture had significantly more full-column, nonacid GER than those who had a negative culture PPI ? pos culture BAL Rosen R. Pediatr. 2011;159:504-6 Lansoprazole for children with poorly controlled asthma: a RCT (2) Writing Committee for the American Lung Association Asthma Clinical Research Centers. JAMA.2012;307:373-81 … 115 children with pH metries: prevalence of GER was 43% In the subgroup with a positive pH study, no treatment effect for lansoprazole vs placebo was observed for any asthma outcome. Children treated with lansoprazole reported more respiratory infections (relative risk, 1.3 [95% CI, 1.1-1.6]). Children with poorly controlled asthma without symptoms of GER who were using inhaled corticosteroids, the addition of lansoprazole, compared with placebo, improved neither symptoms nor lung function but was associated with increased adverse events. 24 19-12-2015 “PROTON-PUMP INHIBITOR THERAPY INDUCES ACIDRELATED SYMPTOMS IN HEALTHY VOLUNTEERS AFTER WITHDRAWAL OF THERAPY” • RCT with 120 healthy adults volunteers •Random 12 weeks of placebo 8 weeks of esomeprazole 40 mg/die followed by 4 weeks with placebo. PPI therapy for 8 weeks induces acid-related symptoms in healthy volunteers after withdrawal Reimer C et al. Gastroenterology 2009; 137: 80-87 CASO CLINICO: La dispepsia non ulcerosa • Alberto giunge alla ns osservazione all’età di 5 anni e 4 mesi…..(Aprile 2010) • Nessun problema clinico rilevante da segnalare fino a circa 1 anno prima quando manifesta tosse stizzosa • Test allergometrici: positività per aeroallergeni • Avvia profilassi con antileucotrieni. • Dopo qualche mese…..(Maggio 2009) esordio di frequenti eruttazioni, senso di sazietà precoce, vomito episodico (2-3 episodi/mese) di colore scuro (!), sembra avere fastidio allo “stomaco”. CASO CLINICO: La dispepsia non ulcerosa • Dopo 4 mesi (Settembre 2009) la sintomatologia persiste … pratica esami ematochimici Hb 10,8 g/dl MCV 70.6 fl MCH: 22.3 Picogr GR 4.630.000/micrL Ferritina 3 ng/ml Sideremia 21micrg/dl Sierologia per malattia celiaca negativa • Parametri auxologici: nella norma • Per la lieve anemia ipocromica microcitica avvia una profilassi marziale CASO CLINICO: La dispepsia non ulcerosa • Il tempo intanto passa…..Alberto continua a lamentare gli stessi sintomi, la mamma riferisce che riduce l’assunzione di alimenti solidi anche se… continua a mangiare grosse quantità di “junk food” • Siamo a Gennaio 2010, considerata la comparsa di saltuari episodi di rigurgiti e le modifiche del comportamento alimentare, viene consigliato un trial empirico con IPP (pantoprazolo per 28 gg) • Alberto migliora ma non completamente……ad Aprile 2010 bussa alla porta del nostro ambulatorio CASO CLINICO: La dispepsia non ulcerosa • Alberto si presenta estremamente pallido, appare realmente sofferente, organizziamo un Day Hospital urgente E.O • Peso: 20.200 Kg (50°-75° ct.) Altezza: 141 cm (25°-50°ct.) • Cute pallida , mucose visibili ipoemiche. Idratazione sufficiente, refill < 2 sec. P.A. 100/60 mmHg. F.C. 138 battiti/min’. CASO CLINICO: La dispepsia non ulcerosa • Alberto si presenta estremamente pallido, appare realmente sofferente, organizziamo un Day Hospital urgente E.O • Peso: 20.200 Kg (50°-75° ct.) Altezza: 141 cm (25°-50°ct.) • Cute pallida , mucose visibili ipoemiche. Idratazione sufficiente, refill < 2 sec. P.A. 100/60 mmHg. F.C. 138 battiti/min’. CASO CLINICO: La dispepsia non ulcerosa Dopo qualche ora arrivano i primi esami di laboratorio: • RBC: 4.170 (x 106/µL); HB: 7.00 g/dl; HCT: 24.6 (%); MCV: 59.00 fl; MCH: 16.8 picogr; PLT: 663 (x 103/µL); WBC: 7.31 (x103/µL) (NEUT: 33.2 %; LINF: 51.5 %; MON: 7.7 %; EOS: 3.4%; BAS: 0.3%) • Ca: 8.7 mg/dl; Prot: 5.5 g/dl; Albumina: 3.5 g/dl; • Quick, APTT e Fibrinogeno: nella norma Si dispone il ricovero CASO CLINICO: La dispepsia non ulcerosa • Considerata l’assenza di ematemesi e melena ed il buon compenso emodinamico si decide di non trasfondere. • A ricovero pratica….tra l’altro Calprotectina fecale: 29 micrg/g Occult test: negativo Striscio periferico: all’esame dello striscio periferico si evidenziano numerosi microciti ed ipocromia delle emazie, una discreta anisopoichilocitosi Sierologia per celiachia: negativa QPE: lieve aumento delle alfa globuline, ipogammaglobulinemia Ig tot: IgG 2.960 g/l, IgM 1.050 g/l, IgA 0.555 g/l, IgE tot: 99.80 KU/l Carico di ferro: nella norma (T0: 7 micrg/dl, T 120 min: 311 micrg/dl) Test di permeabilità intestinale: rapporto cellobiosio/mannitolo 0.005 (v.n.<0.023) Test del sudore: negativo, Steatocrito: negativo CASO CLINICO: La dispepsia non ulcerosa Ricapitoliamo un attimo….. • Alberto ha un anemia severa ipocromica microcitica: Non presenta segni clinici (ematemesi e/o melena) e/o di laboratorio (occult test e calprotectina fecale: negativi o nella norma) di sanguinamento GI attivo Non presenta malassorbimento (Test di permeabilità intestinale, Carico di Fe: nella norma) o maldigestione (Steatocrito e test del sudore: nella norma) Non presenta alterazioni della coagulazione e/o problemi midollari (striscio periferico nella norma) CASO CLINICO: La dispepsia non ulcerosa A questo punto….sono passati 3 giorni dal ricovero …..decidiamo di eseguire “finalmente” un’EGDS Macroscopicamente: ESOFAGITE SEVERA (III grado sec. Hetzel-Dent) Istologicamente: Mucosa esofagea: tessuto di granulazione attivo ed essudato fibrino-leucocitario. Gastrite severa attiva (H.pylori. Neg) . Mucosa duodenale con normale architettura e segni infiammatori. CASO CLINICO: La dispepsia non ulcerosa • Per escludere alterazioni anatomiche pratichiamo un Rx-digerente con studio fino al cieco • Esofago leggermente ectasico con ispessimento delle pliche mucose come da esofagite. Cardias beante. Stomaco in sede, normale per forma e volume, con ipertrofia del rilievo plicare, che si nota anche a livello del duodeno da riferire a gastro-duodenite. Regolare morfologia, struttura e svolgimento del digiuno ed ileo. Cieco in sede CASO CLINCO: La dispepsia non ulcerosa La terapia di Alberto…. • IPP e.v.: 1 mg/kg/die per 4 gg, quindi esomeprazolo: 20 mg/die per os per 12 settimane • Ferro ev (fabbisogno di ferro calcolato= 338 mg) e quindi per os per 2 mesi (30 mg/die) Dopo un settimana dalla dimissione……Alberto sta bene non lamenta sintomi e la sua Hb: 9.6 mg/dl
Scaricare