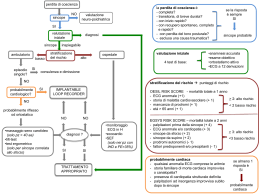
Anamnesi ed esame obiettivo rodolfo sbrojavacca AOU Udine SINCOPE 2 0 1 1 The initial evaluation of a patient presenting with T-LOC consists of careful history, physical examination, including orthostatic BP measurements and electrocardiogram (ECG). measurements, (ECG) Based on these findings, additional examinations may be performed. Task Force ESC, Guidelines (verison 2009) European Heart Journal (2009) 30, 2631–2671 SINCOPE 2 0 1 1 Perché ci facciamo i fatti degli altri? SINCOPE 2 0 1 1 La anamnesi per definire una probabilità à SINCOPE 2 0 1 1 Pretest probability of disease T- T+ 0% 100% rule OUT grey zone + rule IN Worster A CJEM vol.4, n.5, sept 2002 SINCOPE 2 0 1 1 SINCOPE 2 0 1 1 Pretest Post-test Probability Probability Many tests for syncope have a low diagnostic yield. A careful f l history, hi t physical h i l examination, i ti and electrocardiography will provide a diagnosis or determine whether diagnostic testing is necessary in most patients. Linzer M et al Ann Intern Med 1997;126:989-96 SINCOPE 2 0 1 1 di diagnostic i yield i ld the number of p pts. with positive test results divided by th number the b off patients ti t ttested. t d Linzer M et al Ann Intern Med 1997;126:989-96 SINCOPE 2 0 1 1 Generating gp pre-test p probabilities: a neglected area in clinical decision making Attia JR et al MJA, 2004,;180(9)449-454 SINCOPE 2 0 1 1 Experienced physicians, in response to the same clinical scenarios, gave a wide range of estimates for pre-test pre test probability. The developement and dissemination of clinical decision rules is needing to support decision making by practising clinicians. Attia JR et al MJA, 2004,;180(9)449-454 SINCOPE 2 0 1 1 Q l lluogo più Quale iù adatto, d tt per una anamnesii attenta tt t e dettagliata, di un silenzioso box di PS mentre trenta pazienti attendono tranquillamente in sala d’ attesa conversando amabilmente con i loro familiari? Un q questionario standardizzato o l’ aiuto del computer p sono un insulto per l’ arte medica? SINCOPE 2 0 1 1 European Heart Journal (2009) 30, 2631–2671 SINCOPE 2 0 1 1 Ogni uomo racconta una storia. Ma ha bisogno di tempo. SINCOPE 2 0 1 1 In una videoregistrazione di 93 visite in ED di pazienti non critici, i 24 medici che hanno partecipato allo studio hanno interrotto i pazienti prima che finissero di spiegare il motivo del loro accesso nell’80% nell 80% dei casi casi, in media dopo 12 secondi. Resuscitating the physician-patient relationship Ann Emerg Med 2004;44:262-67 SINCOPE 2 0 1 1 The initial evaluation should answer three key questions: (1) Is it a syncopal episode or not? (2) Has the aetiological diagnosis been determined? (3) Are there data suggestive of a high risk of cardiovascular events or death? European Heart Journal (2009) 30, 2631–2671 SINCOPE 2 0 1 1 La a T-LOC OC è il p problema? ob e a SINCOPE 2 0 1 1 McDermott Quinn McDermott, Quinn, 2011 SINCOPE 2 0 1 1 Fu vera sincope? Lasciare la sentenza ai posteri può essere pericoloso SINCOPE 2 0 1 1 European Heart Journal (2009) 30, 2631–2671 SINCOPE 2 0 1 1 Questions about background Family history of sudden death, congenital arrhythmogenic heart disease or fainting Previous cardiac disease Neurological history (Parkinsonism, epilepsy, narcolepsy) Metabolic disorders (diabetes, etc.) Medication (antihypertensive, antianginal, antidepressant agent, antiarrhythmic, diuretics and QT prolonging agents) (I case off recurrentt syncope)) Information (In I f ti on recurrences such h as the time from the firstsyncopal episode and on the number of spells ESC SINCOPE 2 0 1 1 Tre domande chiave • Perché sei qui? • Chi sei? • Cosa p possiamo fare p per te? SINCOPE 2 0 1 1 We feel there is little utility in using any specific age threshold for increased risk when assessing patients with syncope. Risk of adverse outcomes after syncope y p gradually g y increases with age, and should be considered in the context of other risk factors, particularly heart disease. McDermott, Quinn 2007 SINCOPE 2 0 1 1 SINCOPE 2 0 1 1 Questions about circumstances just prior to attack • Position (supine, sitting or standing) • Activity (rest (rest, change in posture, posture during or after exercise, exercise during or immediately after urination, defaecation, cough or swallowing) • Predisposing factors (e.g. crowded or warm places, prolonged standing, post-prandial d l period) d) and d off precipitating i i i events (e.g. ( ffear, intense pain, neck movements); ESC SINCOPE 2 0 1 1 In patients with certain or suspected heart disease the most specific predictors of a disease, cardiac cause were syncope y p in the supine p position or during effort, blurred vision and convulsive syncope. Alboni P et al. J Am Coll Cardiol 2001;37:1921-8 SINCOPE 2 0 1 1 The absence of nausea or vomiting before the syncopal episode was a predictor of higher risk for o arrhythmic a yt c causes o of syncope, sy cope, but no o other ot e symptoms were helpful. Oh J. Et al Arch Intern Med. 1999;159:375-380. SINCOPE 2 0 1 1 Significant and specific predictors of a neurally mediated cause were time between the first and last syncopal episode >4 years, abdominal discomfort before the loss of consciousness and nausea and diaphoresis p during the recovery phase. Alboni P et al. J Am Coll Cardiol 2001;37:1921-8 SINCOPE 2 0 1 1 Questions about attack (eyewitness) Way of falling (slumping or kneeling over), skin colour (pallor, cyanosis, flushing), duration of loss of consciousness, breathing pattern (snoring), movements (tonic, clonic, tonic-clonic or minimal myoclonus, l automatism) t ti ) and d their th i duration, d ti onsett off movement in relation to fall, tongue biting ESC SINCOPE 2 0 1 1 SINCOPE 2 0 1 1 Imparare a gestire l’ ansia dei familiari e a convertirli da nemici ad alleati. Una testimonianza decisiva può a volte essere raccolta solo in PS. SINCOPE 2 0 1 1 Hoefnagels, WA, Padberg, GW, Overweg, J, et al. Syncope or seizure? A matter of opinion. Clin Neurol Neurosurg 1992; 94:153. SINCOPE 2 0 1 1 SINCOPE 2 0 1 1 Questions about end of attack Nausea vomiting, Nausea, vomiting sweating, sweating feeling of cold, cold confusion, muscle aches, skin colour, injury, chest h pain, palpitations, l urinary i or faecal incontinence Task Force on Syncope, ESC SINCOPE 2 0 1 1 Symptoms and signs of syncope: a review of the link between physiology and clinical clues Wieling et al SINCOPE 2 0 1 1 Brain 2009: 132; 2630–2642 Il ritorno dell’ emigrante SINCOPE 2 0 1 1 Il gioco dell dell’ indiano F i ti Fainting llark k SINCOPE 2 0 1 1 La sincope del Farmacista (La notte porta consiglio) SINCOPE 2 0 1 1 Non importa quanto sia stata accurata la tua anamnesi. anamnesi Il paziente terrà sempre in serbo qualcosa solo per il primario. SINCOPE 2 0 1 1 Next time take a better history! SINCOPE 2 0 1 1 The initial evaluation should answer three key questions: (1) Is it a syncopal episode or not? (2) Has the aetiological diagnosis been determined? (3) Are there data suggestive of a high risk of cardiovascular events or death? European Heart Journal (2009) 30, 2631–2671 SINCOPE 2 0 1 1 Three key questions should be addressed during the initial evaluation: • Is loss of consciousness attributable to syncope or not? • Are there features in the history that suggest the diagnosis? • Is heart disease present or absent? Brignole Heart 2007; 93: 130-136. SINCOPE 2 0 1 1 “ L’ anamnesi è la parte più importante d ll’ esame obiettivo” dell’ bi tti ” SINCOPE 2 0 1 1 L’ esame obiettivo è obiettivo? SINCOPE 2 0 1 1 Anamnesi ed esame obiettivo sono metodiche operatore-dipendente SINCOPE 2 0 1 1 Il fattore k Q Quante t volte lt medici di i diversi, di i visitando i it d llo stesso t paziente,, concordano sulla presenza p p o sulla assenza di un segno clinico? • definizione • modesta dei segni clinici vaga capacità del medico • evanescenza • mancanza • bias d segni dei di concentrazione (PS) Interobserver agreement: physical signs McGee, EB Phisical Diagnosis, 2002 SINCOPE 2 0 1 1 Interobserver agreement: diagnostic standards McGee, EB Phisical Diagnosis The presence of suspected or certain heart disease after the initial evaluation is a strong predictor of a cardiac cause of syncope. p y p Alboni P et al. J Am Coll Cardiol 2001;37:1921-8 SINCOPE 2 0 1 1 Murmurs indicative of valvular heart disease or obstruction to flow may prompt further evaluation ACEP SINCOPE 2 0 1 1 L’ ECG è parte dell’esame obiettivo SINCOPE 2 0 1 1 Ip parametri vitali sono vitali SINCOPE 2 0 1 1
Scaricare