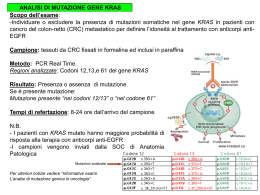
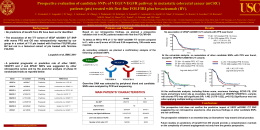
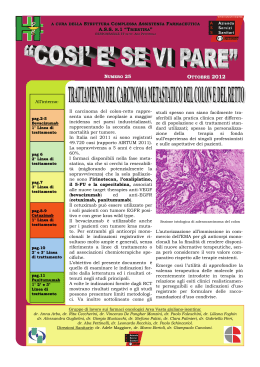
Massimo Zeuli Oncologia Medica A Istituto Regina Elena Roma [email protected] "The best therapeutic approach to patients with KRAS wild type tumors" Roma 4 marzo 2011 EGFR-Targeted Monoclonal Antibodies in mCRC • Cetuximab – IgG1 mAb – Chimeric protein • Panitumumab[1] – IgG2 mAb – Fully humanized • Role of Kirsten-ras (K-ras) mutation 1. Yang XD, et al. Crit Rev Oncol Hematol. 2001;38:17-23. The BOND Study: Survival Data • Addition of cetuximab to irinotecan improved the response rate and time to progression but not overall survival OS Time to Progression 100 80 HR: 0.54 (95% CI: 0.42-0.71) 60 P < .0001 Alive (%) Progression Free (%) 100 40 80 HR: 0.91 (95% CI: 0.68-1.21) 60 P = .48 40 20 20 0 0 0 2 4 6 8 Months 10 12 0 2 Cunningham D, et al. N Engl J Med. 2004;351:337-345. Copyright © 2004 Massachusetts Medical Society. All rights reserved. 4 6 8 10 Months 12 14 16 EPIC Study of Cetuximab in Second-Line mCRC: PFS Progression Free (%) 100 Cetuximab + irinotecan (n = 648) Irinotecan (n = 650) 80 60 40 Median PFS: 4.0 months Median PFS: 2.6 months HR: 0.69 (95% CI: 0.62-0.78) P ≤ .0001 20 0 0 3 6 9 Months 12 15 Sobrero AF, et al. EPIC: Phase III Trial of Cetuximab Plus Irinotecan After Fluoropyrimidine and Oxaliplatin Failure in Patients With Metastatic Colorectal Cancer.J Clin Oncol. 2008;26:2311-2319. Reprinted with permission from the American Society of Clinical Oncology 18 Panitumumab vs BSC in EGFR-Positive CRC: PFS Results 100 90 Panitumumab + BSC (n = 231) BSC (n = 232) Event Free (%)_ 80 70 60 50 HR: 0.54 (95% CI: 0.44-0.66) P < .0001 40 30 20 10 0 0 8 16 24 32 Weeks 40 48 56 Van Cutsem E, et al. Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer.J Clin Oncol. 2007;25:1658-1664. Reprinted with permission from the American Society of Clinical Oncology. Panitumumab vs BSC in mCRC With Wild-Type K-ras: PFS Results 100 Panitumumab + BSC (n = 124) 90 BSC (n = 119) Progression Free (%) 80 70 60 Median PFS: 12.3 weeks 50 40 30 Median PFS: 7.3 weeks HR: 0.45 (95% CI: 0.34-0.59) P < .0001 20 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 Weeks Amado R, et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer.J Clin Oncol 2008;26:1626-1634. Reprinted with permission from the American Society of Clinical Oncology. Panitumumab vs BSC in mCRC With Mutant K-ras: PFS Results 100 Panitumumab + BSC (n = 84) 90 BSC Alone (n = 100) Progression Free (%) 80 70 60 Median PFS: 7.4 weeks 50 Median PFS: 40 7.3 weeks 30 HR: 0.99 (95% CI: 0.73-1.36) 20 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 Weeks Amado R, et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer.J Clin Oncol 2008;26:1626-1634. Reprinted with permission from the American Society of Clinical Oncology. Douillard J et al. JCO 2010;28:4697-4705 Pazienti kras wild type Cetuximab/Panitumumab aumentano l’efficacia del trattamento chemioterapico Pazienti kras wild type Cetuximab/Panitumumab aumentano l’efficacia del trattamento chemioterapico Bevacizumab aumenta l’efficacia del trattamento chemioterapico Which regimen should we use as neoadjuvant treatment for liver metastases? Pozzo C. et al Cancer Treat Rev, 2008 * * Of the 37 patients evaluable for tumour KRAS mutation status, 81% had KRAS wild-type tumours. Resection rates following targeted therapies plus chemotherapy in randomized trials NO16966 LLD CRYSTAL LLD OPUS KRAS wt R0 resection rate 9.8 FOLFOX + ERBITUX 4.1 FOLFOX 9.8 FOLFIRI + ERBITUX 4.5 FOLFIRI FOLFOX/XELOX + bevacizumab 12.3 p=NS 11.6 FOLFOX + XELOX 0 2 4 6 8 10 12 14 Patients (%) Van Cutsem E, et al. N Engl J Med 2009 Bokemeyer C, et al. J Clin Oncol 2009;27:663–671 Saltz LB et al. J Clin Oncol 2008 Pazienti kras wild type Cetuximab/Panitumumab aumentano l’efficacia del trattamento chemioterapico Bevacizumab aumenta l’efficacia del trattamento chemioterapico Cetuximab aumenta la percentuale di resezioni epatiche R0? Massimo Zeuli Oncologia Medica A Istituto Regina Elena Roma [email protected] "The best therapeutic approach to patients with KRAS wild type tumors" Roma 4 marzo 2011 ? FOLFOX4 x 3 mesi Chirurgia FOLFOX4 x 3 mesi (studio EPOC - Lancet 2008): Pazienti k-ras wild-type, chronoIFLO+ Cetuximab (Studio POCHER Br J Cancer 2010). I pazienti che non possono essere trattati con questo schema e sono wild-type ricevono in prima linea FOLFIRI + Cetuximab (Studio Crystal N Engl J Med 2009). C: Gruppo “ NON- RESECTABLE” K-ras Wild Type K-ras Mutant 1° Linea FOLFIRI + BEVA FOLFIRI + BEVA II° Linea FOLFOX FOLFOX III° Linea Panitumumab MMC + fluoro pirimidina*
Scaricare