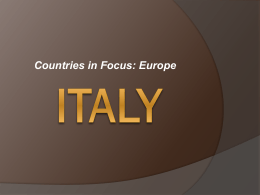
php159 ISPOR 16 Annual European Congress th Dublin 2 - 6 November 2013 Workshop in Pharmacoeconomics: an Italian experience of multi-stakeholder HTA consensus Americo Cicchetti , Antonio Gasbarrini , Matteo Ruggeri , Dario Sacchini , Elena Paola Lanati , on behalf of WEF study group 1 2 1 2 3 Faculty of Economics, Catholic University of Sacred Heart, Rome, Italy 2 Faculty of Medicine, Catholic University of Sacred Heart, Rome, Italy 3 3P Solution S.r.l., Milan, Italy 1 BACKGROUND HTA is a very challenging issue in many countries, including Italy, where it has been officially mentioned for the first time in the National Healthcare Plan 2006-2008. In Italy only few groups are recognized at international level, some pertaining to central and regional Institutions, some being small independent working groups. The Technology Assessment Unit (UVT), situated at the Policlinico Gemelli – Cattolica University in Rome, was the first HTA group and can be considered a pioneer in Italy. Digestive and Liver Disease 2012 (5) 86 Institute of Internal Medicine, Catholic University Medical School, Rome, Italy The working method consists of a series of meetings (at least 4 per year) of the Scientific board (composed by high-profile experts covering all HTA domains: clinicians, pharmacoeconomists, experts in organizational aspects, bioethicists, patients, Institutions) that carries out a nationwide analysis of the topic under examination and focuses on the main clinical, economic, organizational, social, and ethical features. Questionnaire-based surveys and Delphi panel are the main operational tools. WEF adopts standard HTA procedures according to the EUnetHTA Core Model and to avoid any conflict of interests, no fee is paid to any member. ∗ Corresponding author at: Institute of Internal Medicine, Catholic University of Rome, 8 Largo A. Gemelli, 00168 Rome, Italy. Tel.: +39 0630155451; fax: +39 0635502775. E-mail address: [email protected] (M. Biolato) Reference [1] Böhm G, Mossdorf A, Klink C, et al. Treatment algorithm for postoperative upper gastrointestinal fistulas and leaks using combined Vicryl plug and fibrin glue. Endoscopy 2010;42:599–602. Angelo Caruso ∗ Raffaele Manta Gianluigi Melotti Rita Conigliaro Nuovo Ospedale Civile S. Agostino Estense, Modena, Italy ∗ Corresponding Methods author at: Nuovo Ospedale Civile S. Agostino Estense Via Giardini, 1355 41126 Modena, Italy. Fax: +39 059 3961216; mobile: +39 3494986810. E-mail address: [email protected] (A. Caruso) doi:10.1016/j.dld.2011.07.004 Comment on “The role of endoscopic ultrasound in the evaluation of chronic mesenteric ischaemia” Sir, We read with great interest the article by Almansa et al. published in Digestive and Liver Disease regarding the role of Doppler endoscopic ultrasound as a comprehensive test to evaluate patients with chronic upper abdominal pain in order to exclude chronic mesenteric ischaemia [1]. In this study, authors employed, both in Doppler endoscopic ultrasound and Dopper transabdominal ultrasound, measurement of Peak Systolic Velocity (PSV) in celiac artery and superior mesenteric artery as single parameter for the detection of chronic mesenteric ischaemia. We would add that, beside PSV, another Doppler parameter could be considered: EndDiastolic Velocity (EDV) appears comparable or superior to PSV in identify significant arteriography-detected stenosis, and is not influenced by an hyperdynamic circulation as for PSV [2–5]. In the study of Almansa et al., Doppler endoscopic ultrasound (assessed by means of PSV) presented a specificity of 84% in detecting chronic mesenteric ischaemia; this figure could be even more appealing employing EDV. Conflict of interest statement None declared. Reference [1] Almansa C, Bertani H, Noh KW, et al. The role of endoscopic ultrasound in the evaluation of chronic mesenteric ischaemia. Dig Liver Dis 2011;43:470–4. [2] Moneta GL, Yeager RA, Dalman R, et al. Duplex ultrasound criteria for diagnosis of splanchnic artery stenosis or occlusion. J Vasc Surg 1991;14:511–8. [3] Bowersox JC, Zwolak RM, Walsh DB, et al. Duplex ultrasonography in the diagnosis of celiac and mesenteric artery occlusive disease. J Vasc Surg 1991;14:780–6. [4] Zwolak RM, Fillinger MF, Walsh DB, et al. Mesenteric and celiac duplex scanning: a validation study. J Vasc Surg 1998;27:1078–87. [5] Perko MJ, Just S, Schroeder TV. Importance of diastolic velocities in the detection of celiac and mesenteric artery disease by duplex ultrasound. J Vasc Surg 1997;26:288–93. Marco Biolato ∗ Antonio Grieco WEF E 2011 (1) LETTERS TO THE EDITOR Nationwide prediction of future expenditure for protease inhibitors in chronic hepatitis C Effect of discounting on estimation of benefits determined by hepatitis C treatment Dear Editor, Peginterferon plus ribavirin is the current standard of care for chronic hepatitis C, which determines sustained virological response (SVR) in 30–50% of patients. Protease inhibitors (namely boceprevir and telaprevir) are a further advancement that could increase SVR to approximately 60% [1]. Boceprevir and telaprevir have already been approved by the Food and Drug Administration (FDA) and are about to be marketed in Europe (boceprevir is available in France where its cost per patient is around D 22,000 according to the website http://viralmatters.blogspot.com). The globalization of pharmaceutical markets has much increased the international homogeneity of drug prices; hence, transferring the cost of innovative drugs from one country to another is likely to imply a reasonable approximation. Predicting the economic impact of adding a protease inhibitor to patients treated for hepatitis C is a crucial point in terms of pharmaceutical governance, especially in countries like Italy where the national health system provides full economic coverage of all essential treatments. The first step in evaluating an innovative treatment is to determine its cost-effectiveness; if the pharmacoeconomic profile is acceptable and the drug is therefore likely to be used, the next step is to estimate the budget impact. Since preliminary studies [2] indicate that the cost-effectiveness of these protease inhibitors is favourable, a budget impact analysis focused on these agents is worthwhile. The national expenditure for ribavirin in Italy has been D 33 million in 2009; assuming that each patient receives 840 capsules for a whole treatment (considering a cost of D 4.2 per capsule, and including adjustments for treatment interruptions and suboptimal compliance [3]), this figure of national expenditure indicates that 9300 Italian patients/year receive treatment for hepatitis C regardless of their genotype. Given that genotype 1 accounts for 60% of all patients [4], this translates into a prediction of 5500 Italian patients with genotype 1 to be treated yearly with a protease inhibitor. To estimate the economic impact of adding a protease inhibitor to these patients, we used a prediction model described previously [5]. According to this model, the yearly expenditure for the drug is directly proportional to the yearly number of treated patients (where the proportionality factor is the yearly cost per patient). The model is not drug-specific because the mathematical function simply handles an initial phase where expenditure increases as more and more patients of the eligible yearly population are being treated over time. Fig. 1 shows the results of our budget impact analysis for protease inhibitors based on this model. In our base-case prediction, after projecting the expenditure for up to 5500 patients/year from mid-2012 until 2017, the overall budget impact is estimated to be D 115 million per year at steady state (solid line). Two factors affect the above budget impact analysis by acting in opposite directions. The first is that the patients actually receiving Andrea Messori, Sabrina Trippoli, Laboratorio SIFO di Farmacoeconomia, Area Vasta Centro Toscana, 59100 Prato, Italy Valeria Fadda, Dario Maratea, Department of Pharmaceutical Sciences, University of Firenze, 50019 Sesto Fiorentino, Italy Author contributions: All authors were involved in data collection, study design, data analysis and interpretation and all authors were involved in writing of the manuscript. Correspondence to: Dr. Andrea Messori, PhD, Laboratorio SIFO di Farmacoeconomia, c/o Area Vasta Centro Toscana, Regional Health System, Via Guimaraes 9-11, 59100 Prato, Italy. [email protected] Telephone: +39-347-6053933 Fax: +39-574-701319 Received: December 23, 2011 Revised: February 27, 2012 Accepted: March 20, 2012 Published online: June 21, 2012 con il patrocinio di: © 2012 Baishideng. All rights reserved. Key words: Boceprevir; Telaprevir; Cost-effectiveness; Markov model; Hepatitis C Peer reviewers: Chao-Hung Hung, Kaohsiung Chang Gung Memorial Hospital, 123 Ta Pei Road, Niao Sung, Kaohsiung 833, Taiwan, China; Faisal M Sanai, Hepatobiliary Sciences, King Abdulaziz Medical City, King Abdulaziz Medical City, Riyadh 11462, Saudi Arabia Abstract Messori A, Fadda V, Maratea D, Trippoli S. Effect of discounting on estimation of benefits determined by hepatitis C treatment. World J Gastroenterol 2012; 18(23): 3032-3034 Available from: URL: http://www.wjgnet.com/1007-9327/full/v18/i23/3032.htm DOI: http://dx.doi.org/10.3748/wjg.v18.i23.3032 The combination of either boceprevir or telaprevir with ribavirin and interferon (triple therapy) has been shown to be more effective than ribavirin+interferon (dual therapy) for the treatment of genotype 1 hepatitis C. Since the benefit of these treatments takes place after years, simulation models are needed to predict long-term outcomes. In simulation models, the choice of different values of yearly discount rates (e.g., 6%, 3.5%, 2%, 1.5% or 0%) influences the results, but no studies have specifically addressed this issue. We examined this point by determining the long-term benefits under different conditions on the basis of standard modelling and using quality-adjusted life years (QALYs) to quantify the benefits. In our base case scenario, we compared the long-term benefit between patients given a treatment with a 40% sustained virologic response (SVR) (dual therapy) and patients given a treatment with a 70% SVR (triple therapy), and we then examined how these specific yearly discount rates influenced the incremental benefit. The gain between a 70% SVR and a 40% SVR decreased from 0.45 QALYs with a 0% discount rate to 0.22 QALYs with a 6% discount rate (ratio between the two values = 2.04). T he estimated global prevalence of hepatitis C virus (HCV) infection is 2.2%, corresponding to about 130 million HCV-positive persons worldwide, most of whom are chronically infected.1 A recent revision2 reported that the estimated prevalence of HCV infection in Europe ranges from 0.6% to 5.6%. This is of increasing interest because HCV is a leading cause of both cirrhosis and hepatocellular carcinoma (HCC) in Western countries. The prevalence of HCV-related cirrhosis and its complications will TO THE EDITOR The review by Tsubota et al[1] has examined the main options available for the treatment of hepatitis C, including two antiviral drugs that have recently been marketed in many countries. Focusing more thoroughly on these two innovative agents is worthwhile because boceprevir and telaprevir, along with other innovative agents, are thought to be an important advancement in the treatment of this disease[2], although at a high cost. Hepatitis C virus (HCV) genotype 1, which accounts for 60% of all HCV-infected patients[3-5], is the target at which these two new agents are directed in combination with ribavirin + interferon. Considering that the combination of either boceprevor or telaprevir with ribavirin+interferon (triple therapy) has been shown 3032 continue to increase through the next decade, and will mostly affect those above age 60.3 Considering the burden of HCV-related cirrhosis and its complications, the achievement of a sustained virologic response (SVR) is a very important surrogate outcome in the management of chronic hepatitis C (CHC) patients. In fact, viral eradication prevents the development of cirrhosis4 and its complications, such as esophageal varices5 and HCC,6 and leads to a decrease in liver-related death.7 Abbreviations: BOC, boceprevir; CHC, chronic hepatitis C; DT, dual therapy; G1, genotype 1; ICER, incremental cost effectiveness ratio; PI, protease inhibitors; PEG-IFN, pegylated interferon; RBV, ribavirin; TVR, telaprevir. From the 1Sezione di Gastroenterologia, Di.Bi.M.I.S., University of Palermo, Italy; 2Dipartimento di Scienze Statistiche e Matematiche ‘‘S. Vianelli,’’ University of Palermo, Palermo, Italy; 3Division of Infectious and Tropical Diseases, Foundation IRCCS San Matteo Hospital, University of Pavia, Italy; 4Universit a Cattolica del Sacro Cuore, Facolt a di Economia, Roma, Italy; 5University of Pavia, School of Pharmacy, Italy; 6Universit a Cattolica del Sacro Cuore, Facolt a di Medicina e Chirurgia, Gastroenterologia Roma, Italy. Received December 20, 2011; accepted March 12, 2012. This study was entirely funded by 3P Solution. The funding agency was not involved in the study design or its execution, data management or analysis, article preparation or review, or the decision to submit the article for publication. 850 June 21, 2012|Volume 18|Issue 23| Journal of Hepatology 2013 (9) Cost-Effectiveness of Boceprevir or Telaprevir for Untreated Patients With Genotype 1 Chronic Hepatitis C Value in Health 2013 (10) Available online at www.sciencedirect.com Cost-effectiveness of boceprevir or telaprevir for previously treated patients with genotype 1 chronic hepatitis C journal homepage: www.elsevier.com/locate/jval Calogero Cammà1,⇑, Salvatore Petta1, Giuseppe Cabibbo1, Matteo Ruggeri2, Marco Enea3, Raffaele Bruno4, Vincenza Capursi3, Antonio Gasbarrini5, Alfredo Alberti6, Antonio Craxì1, on behalf of the WEF Study Group Calogero Camma,1 Salvatore Petta,1 Marco Enea,2 Raffaele Bruno,3 Fabrizio Bronte,1 Vincenza Capursi,2 Americo Cicchetti,4 Giorgio L. Colombo,5 Vito Di Marco,1 Antonio Gasbarrini,6 and Antonio Craxı̀,1 on behalf of the WEF Study Group he estimated global prevalence of hepatitis C virus (HCV) infection is 2.2%, corresponding to about 130 million HCV-positive persons worldwide, most of whom are chronically infected.1 A recent revision2 reported that the estimated prevalence of HCV infection in Europe ranges from 0.6% to 5.6%. This is of increasing interest because HCV is a leading cause of both cirrhosis and hepatocellular carcinoma (HCC) in Western countries. The prevalence of HCV-related cirrhosis and its complications will I QUADERNI DI MEDICINA Testing the other discounting assumptions confirmed that the discount rate has a marked impact on the magnitude of the model-estimated incremental benefit. In conclusion, the results of our analysis can be helpful to better interpret cost-effectiveness studies evaluating new treatment for hepatitis C. Research Article T I QUADERNI DI MEDICINA Randomized controlled trials (RCTs) show that triple therapy (TT) with peginterferon alpha, ribavirin, and boceprevir (BOC) or telaprevir (TVR) is more effective than peginterferon-ribavirin dual therapy (DT) in the treatment of previously untreated patients with genotype 1 (G1) chronic hepatitis C (CHC). We assessed the cost-effectiveness of TT compared to DT in the treatment of untreated patients with G1 CHC. We created a Markov Decision Model to evaluate, in untreated Caucasian patients age 50 years, weight 70 kg, with G1 CHC and Metavir F2 liver fibrosis score, for a time horizon of 20 years, the cost-effectiveness of the following five competing strategies: 1) boceprevir response-guided therapy (BOCRGT); 2) boceprevir IL28B genotype-guided strategy (BOC-IL28B); 3) boceprevir rapid virologic response (RVR)-guided strategy (BOC-RVR); 4) telaprevir response-guided therapy (TVR-RGT); 5) telaprevir IL28B genotype-guided strategy (TVR-IL28B). Outcomes included life-years gained (LYG), costs (in 2011 euros) and incremental cost-effectiveness ratio (ICER). In the base-case analysis BOC-RVR and TVR-IL28B strategies were the most effective and cost-effective of evaluated strategies. LYG was 4.04 with BOC-RVR and 4.42 with TVR-IL28B. ICER compared with DT was €8.304 per LYG for BOC-RVR and €11.455 per LYG for TVR-IL28B. The model was highly sensitive to IL28B CC genotype, likelihood of RVR and sustained virologic response, and BOC/TVR prices. Conclusion: In untreated G1 CHC patients age 50 years, TT with first-generation protease inhibitors is costeffective compared with DT. Multiple strategies to reduce costs and improve effectiveness include RVR or genotype-guided treatment. (HEPATOLOGY 2012;56:850-860) VALUE IN HEALTH 16 (2013) 965–972 WEF E 2012 (2) APRILE 2012 Calogero Camma,1 Salvatore Petta,1 Marco Enea,2 Raffaele Bruno,3 Fabrizio Bronte,1 Vincenza Capursi,2 Americo Cicchetti,4 Giorgio L. Colombo,5 Vito Di Marco,1 Antonio Gasbarrini,6 and Antonio Craxı̀,1 on behalf of the WEF Study Group Andrea Messori, Valeria Fadda, Dario Maratea, Sabrina Trippoli 1 Economic Assessment of an Anti-HCV Screening Program in Italy Matteo Ruggeri1,*, Silvia Coretti1, Antonio Gasbarrini2, Americo Cicchetti1 2 Sezione di Gastroenterologia, Di.Bi.M.I.S., University of Palermo, Italy; Institute of Policy and Economics, Graduate school of Health Economics and Management, Università Cattolica del Sacro Cuore, Roma, Italy; 3Dipartimento di Scienze Statistiche e Matematiche ‘‘S. Vianelli’’, University of Palermo, Palermo, Italy; 4Division of Infectious and Tropical Diseases, Foundation IRCCS San Matteo Hospital, University of Pavia, Italy; 5Università Cattolica del Sacro Cuore, Facoltà di Medicina e Chirurgia, GastroenteroLogia, e Economica, Università Cattolica del Sacro Cuore, Roma, Italy; 6Department of Histology, Microbiology and Medical Biotechnologies, Venetian Institute of Molecular Medicine, University of Padova, Italy Randomized controlled trials (RCTs) show that triple therapy (TT) with peginterferon alpha, ribavirin, and boceprevir (BOC) or telaprevir (TVR) is more effective than peginterferon-ribavirin dual therapy (DT) in the treatment of previously untreated patients with genotype 1 (G1) chronic hepatitis C (CHC). We assessed the cost-effectiveness of TT compared to DT in the treatment of untreated patients with G1 CHC. We created a Markov Decision Model to evaluate, in untreated Caucasian patients age 50 years, weight 70 kg, with G1 CHC and Metavir F2 liver fibrosis score, for a time horizon of 20 years, the cost-effectiveness of the following five competing strategies: 1) boceprevir response-guided therapy (BOCRGT); 2) boceprevir IL28B genotype-guided strategy (BOC-IL28B); 3) boceprevir rapid virologic response (RVR)-guided strategy (BOC-RVR); 4) telaprevir response-guided therapy (TVR-RGT); 5) telaprevir IL28B genotype-guided strategy (TVR-IL28B). Outcomes included life-years gained (LYG), costs (in 2011 euros) and incremental cost-effectiveness ratio (ICER). In the base-case analysis BOC-RVR and TVR-IL28B strategies were the most effective and cost-effective of evaluated strategies. LYG was 4.04 with BOC-RVR and 4.42 with TVR-IL28B. ICER compared with DT was €8.304 per LYG for BOC-RVR and €11.455 per LYG for TVR-IL28B. The model was highly sensitive to IL28B CC genotype, likelihood of RVR and sustained virologic response, and BOC/TVR prices. Conclusion: In untreated G1 CHC patients age 50 years, TT with first-generation protease inhibitors is costeffective compared with DT. Multiple strategies to reduce costs and improve effectiveness include RVR or genotype-guided treatment. (HEPATOLOGY 2012;56:850-860) GIUGNO 2011 © 2012 Baishideng. All rights reserved. doi:10.1016/j.dld.2011.07.011 WJG|www.wjgnet.com Since 2011, three HTA reports have been produced on hepatology, focusing in 2011 and 2012 respectively on HBV/HCV screening strategies and HCV new Direct Antiviral Agents (DAA)-based therapies and extending in 2013 to hepatocellular carcinoma. In 2013 a second therapeutical area was assessed, dealing with gastroenterology and inflammatory bowel diseases (IBDs), in particular with Crohn’s disease and its treatment with biological high-cost drugs. For 2014, a fourth edition on hepatology and a second on IBDs are being developed. A first WEF edition on HIV is also coming up next year. Cost-Effectiveness of Boceprevir or Telaprevir for Untreated Patients With Genotype 1 Chronic Hepatitis C World J Gastroenterol 2012 June 21; 18(23): 3032-3034 ISSN 1007-9327 (print) ISSN 2219-2840 (online) Online Submissions: http://www.wjgnet.com/1007-9327office [email protected] doi:10.3748/wjg.v18.i23.3032 Hepatology 2013 (8) Results Hepatology 2012 (7) Correspondence / Digestive and Liver Disease 44 (2012) 85–87 Conflict of interest statement No conflict of interest. Objectives The objective of the Italian Workshop in Pharmacoeconomics (WEF), born as a practical application of HTA, is to validate an innovative experience that aims at being recognized by Institutions as a national and independent HTA assessor, thus supporting both national and regional healthcare decision-makers. This experience consists of a multi-stakeholder working group that, in the field of new technologies proposed for critical clinical areas, discusses and develops guide-lines and decision rules and comparatively examines local real practice data, directly collected by the members of the Scientific Board. World Journal of Gastroenterology 2012 (6) Background & Aims: Randomised controlled trials (RCTs) show that triple therapy (TT) with peginterferon alfa, ribavirin, and boceprevir (BOC) or telaprevir (TVR) is more effective than peginterferon-ribavirin dual therapy (DT) in the treatment of genotype 1 (G1) chronic hepatitis C (CHC) patients with previous relapse (RR), partial response (PAR), and null-response (NR). We assess the cost-effectiveness of TT compared to no therapy in the treatment of patients previously treated with G1 CHC. Methods: The available published literature provided the data source. The target population was made up of previously treated Caucasian patients with G1 CHC and these were evaluated over a lifetime horizon by Markov model. The study was carried out from the perspective of the Italian National Health Service. Outcomes included discounted costs (in euro at 2012 value), life years gained (LYG), quality adjusted life year (QALY), and incremental cost-effectiveness ratio (ICER).The robustness of the results was evaluated by one-way deterministic and multivariable probabilistic sensitivity analyses. Results: In RR patients, ICER per LYG compared to no therapy was €9555 for BOC-LEAD-IN-RR and €7910 for TVR-LEAD-IN-RR, being BOC dominated by TVR. In PAR patients, ICER for LYG was €11,947 for BOC-LEAD-IN-PAR and €14,931 for TVR-PAR, being TVR cost-effective compared to BOC (ICER for QALY €22,258). In NR patients, ICER for LYG was €26,499 for TVR-LEAD-IN-NR. The models were sensitive to likelihood of sustained virological response and to BOC/TVR prices. continue to increase through the next decade, and will mostly affect those above age 60.3 Considering the burden of HCV-related cirrhosis and its complications, the achievement of a sustained virologic response (SVR) is a very important surrogate outcome in the management of chronic hepatitis C (CHC) patients. In fact, viral eradication prevents the development of cirrhosis4 and its complications, such as esophageal varices5 and HCC,6 and leads to a decrease in liver-related death.7 Keywords: Boceprevir; Telaprevir; Cost-effectiveness. Received 25 December 2012; received in revised form 9 May 2013; accepted 14 May 2013; available online 23 May 2013 ⇑ Corresponding author. Address: Sezione di Gastroenterologia, University of Palermo, Piazza delle Cliniche, 2, 90127 Palermo, Italy. Tel.: +39 091 655 2145; fax: +39 091 655 2156. E-mail address: [email protected] (C. Cammà). Abbreviations: CHC, chronic hepatitis C; G1, genotype 1; DT, dual therapy; PegIFN, pegylated interferon; RBV, ribavirin; PI, protease inhibitors; BOC, boceprevir; TVR, telaprevir; ICER, incremental cost-effectiveness ratio; NR, non-response; PAR, partial response; RR, relapse. 1 Faculty of Economics, Catholic University of Sacred Heart, Rome, Italy; 2Faculty of Medicine, Catholic University of Sacred Heart, Rome, Italy AB STR A CT Conclusions: 1st generation HCV PI is highly cost-effective compared to no therapy in RR and PAR G1 CHC patients. TVR dominated BOC in RR, and was cost-effective compared to BOC in PAR patients. In NR patients an assessment of the response after a lead-in period should be performed to improve safety and costeffectiveness. 2013 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Introduction Approximately 50% of all patients with genotype 1 chronic hepatitis C (G1 CHC) treated with dual therapy (DT) with peginterferon (PegIFN) plus ribavirin (RBV) experience treatment failure [1]. This means they represent a growing cohort of individuals at higher risk of liver-related complications [2]. Considering the high likelihood of disease progression of CHC patients failing DT [3,4], and the burden of hepatitis C virus (HCV)-related cirrhosis and its related complications, the achievement of a sustained virological response (SVR) is a very important surrogate outcome in patient management. In fact, viral eradication prevents the development of cirrhosis [5] and its related complications, such as oesophageal varices [6] and hepatocellular carcinoma (HCC) [7], and reduces liver-related death [8]. Two large randomized controlled trials (RCTs) [3,4], studying long-term maintenance therapy with low-dose PegIFN in CHC patients failing DT, showed no benefit in terms of progression of liver disease. Several RCTs [9,10] and a recent meta-analysis [11] showed that re-treatment of G1 non-responders with DT favours SVR achievement in only 15% of patients. Guidelines of the European Association for the Study of the Liver (EASL) [12] and of the American Association for the Study of Liver Disease (AASLD, 2011) [13] recommended that patients infected with G1 HCV and who failed to eradicate HCV after prior DT should not be re-treated with the same drug regimen. It was suggested were discounted by 3.5%. Results were expressed as cost/qualityadjusted life-year (QALY) gained through the screening program compared with the treatment of symptomatic patients. Deterministic and probabilistic sensitivity analysis was performed. Results: The incremental cost-effectiveness ratio of the ‘‘Test Strategy’’ is €5171/QALY, definitively below the cost/QALY of other approved treatments in Italy. Model results turned out as sensitive to the age of the target population, the prevalence of HCV infection, and the time horizon adopted. Conclusions: The anti-HCV screening program is a valid health-related investment improving patients’ quality of life and survival with an acceptable expenditure increase for the National Health Service. Keywords: cost-effectiveness, Italy, liver disease, Markov model. Introduction benefits to health many years later. A recent systematic review [2] summarized the results of seven studies about hepatitis C screening programs carried out in France, Great Britain, and the United Kingdom on subgroups of patients. The incremental costeffectiveness ratio (ICER) of screening compared with treatment of symptomatic patients was found to range between €3,900 and €243,700 per life-year gained, or €18,000 and €1,151,000 per quality-adjusted life-year (QALY) gained. The authors concluded that screening was cost-effective in populations with a high prevalence of HCV infection but excessively costly in populations with a low prevalence. The purpose of this study was to evaluate the costeffectiveness of a screening strategy aimed at identifying HCVpositive patients in comparison with the treatment of patients who have developed cirrhosis or HCC following undiagnosed chronic hepatitis. Viral hepatitis is a chronic condition with a latent, nonlinear disease progression. Hepatitis C virus (HCV) disease can remain asymptomatic for decades and resolves spontaneously only in exceptional cases. The disease normally takes over a decade to progress, although this may be accelerated by the presence of various cofactors including alcohol use, diabetes mellitus (for which HCV is a risk factor), the age at which the disease was developed, and coinfection with HIV or other hepatotropic viruses. Between 10% and 40% of patients with chronic HCV infection will develop cirrhosis, depending on the occurrence of these cofactors. The annual incidence of death due to cirrhosis complications is around 4%, while the annual incidence of hepatocarcinoma (HCC) among patients with chronic HCV infection is 1% to 5%. Patients with HCC have a 33% chance of surviving beyond 1 year after its onset [1]. Early diagnosis following a screening test for chronic hepatitis is an effective tool for the prompt treatment of HCV infection, stopping the progression of any liver disease. Numerous studies have been conducted in recent years to investigate the costeffectiveness ratio of screening for viral hepatitis. Many of these studies have used decisional models because these tools are wellsuited to the design of early diagnosis programs, which usually require considerable investment in the present but pay back their Journal of Hepatology 2013 vol. 59 j 658–666 Abbreviations: BOC, boceprevir; CHC, chronic hepatitis C; DT, dual therapy; G1, genotype 1; ICER, incremental cost effectiveness ratio; PI, protease inhibitors; PEG-IFN, pegylated interferon; RBV, ribavirin; TVR, telaprevir. From the 1Sezione di Gastroenterologia, Di.Bi.M.I.S., University of Palermo, Italy; 2Dipartimento di Scienze Statistiche e Matematiche ‘‘S. Vianelli,’’ University of Palermo, Palermo, Italy; 3Division of Infectious and Tropical Diseases, Foundation IRCCS San Matteo Hospital, University of Pavia, Italy; 4Universit a Cattolica del Sacro Cuore, Facolt a di Economia, Roma, Italy; 5University of Pavia, School of Pharmacy, Italy; 6Universit a Cattolica del Sacro Cuore, Facolt a di Medicina e Chirurgia, Gastroenterologia Roma, Italy. Received December 20, 2011; accepted March 12, 2012. This study was entirely funded by 3P Solution. The funding agency was not involved in the study design or its execution, data management or analysis, article preparation or review, or the decision to submit the article for publication. Background: The progression of hepatitis C virus (HCV) disease usually occurs over a 10-year period. HCV-related complications as well as the highly debilitating effects on patients represent a significant item of expenditure for the National Health Service. Early detection of HCV infection is an excellent opportunity to improve patients’ quality of life and to rationalize resource allocation. Objective: The aim of this study was to provide a cost-effectiveness evaluation of an anti-HCV screening program in the Italian National Health Service perspective. Methods: We built a Markov model made up of two arms. The ‘‘Test Strategy’’ arm involves a screening program based on the enzyme immunoassay for detection of antibodies as first-level test and the research of HCV RNA as second-level detection; patients with positive test results are treated with peg-interferon alfa in combination with ribavirine. Parameters were derived from the literature and validated through experts’ opinion. Costs and benefits Copyright & 2013, International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. Methods Model Structure We studied HCV disease progression up to death, simulating the observation of a cohort of 100,000 individuals from the general * Address correspondence to: Matteo Ruggeri, Faculty of Economics, Catholic University of Sacred Heart, l.go F.Vito 1, Rome 00168, Italy. E-mail: [email protected]. 1098-3015/$36.00 – see front matter Copyright & 2013, International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. 850 http://dx.doi.org/10.1016/j.jval.2013.07.005 Primo WorkshoP naZionale di economia e Farmaci in ePatoloGia WeF-e 2011 dalle epatiti all’epatocarcinoma: epidemiologia e costi associati to pubblicato grazie ad un unrestricted grant di Questo report è stato pubblicato grazie ad un unrestricted grant di: roma, 27-28 aprile 2011 secondo WorkshoP naZionale di economia e Farmaci in ePatoloGia WeF-e 2012 il trattamento delle epatiti virali in italia: la sostenibilità di un modello vincente per il bene del paziente roma, 2 febbraio 2012 Reduc+on in +me-‐to-‐market WEF E 2013 (3) WEF IBD 2013 (4) xxxxxxxxxxxx 2013 I QUADERNI DI MEDICINA GIUGNO 2013 I QUADERNI DI MEDICINA con il patrocinio di: con il patrocinio di: TERZO WORkshOp di EcOnOmia E FaRmaci in EpaTOlOgia WEF-E 2013 ROma 7 - 8 FEBBRAIO 2013 ITALY Veneto Umbria Toscana Sardegna Lazio Emilia-‐Romagna Mean HCV DAAs 0 PRIMO WORKSHOP DI ECONOMIA E FARMACI PER LE MALATTIE INFIAMMATORIE CRONICHE INTESTINALI WEF-IBD 2013 50 100 150 200 250 300 Days from na+onal authoriza+on ROMA 6 FEBBRAIO 2013 Conclusions Along with 6 publications in international journals (mean impact factor 7,1), there have also been auditions at the Italian Drug Agency (AIFA) and at the Healthcare Commission in Parliament that have facilitated the approval of new HCV drugs. Furthermore, the analysis of available data about delays in approvals by regional formularies have been reduced by about 55% (from 221 days after national marketing authorization to 101 days; Farmindustria data). 1) Primo Workshop Nazionale di Economia e Farmaci in Epatologia WEF-E 2011 - Roma, 27-28 aprile 2011. I quaderni di medicina Il 24 ore Sanità. Giugno 2011 2) Secondo Workshop Nazionale di Economia e Farmaci in Epatologia WEF-E 2012 - Roma, 2 febbraio 2012. I quaderni di medicina Il 24 ore Sanità. Aprile 2012 3) Terzo Workshop Nazionale di Economia e Farmaci in Epatologia WEF-E 2013 - Roma, 7-8 febbraio 2013. I quaderni di medicina Il 24 ore Sanità. Luglio 2013 4) Primo Workshop Nazionale di Economia e Farmaci per le Malattie Infiammatorie Croniche Intestinali -WEF-IBD 2013 - Roma, 6 febbraio 2013. I quaderni di medicina Il 24 ore Sanità. Giugno 2013 5) Maratea D, Messori A, Fadda V; WEF-E Study Group. Nationwide prediction of future expenditure for protease inhibitors in chronic hepatitis C. Dig Liver Dis. 2012 Jan;44(1):86-7. 6) Messori A, Fadda V, Maratea D, Trippoli S. Effect of discounting on estimation of benefits determined by hepatitis C treatment. World J Gastroenterol. 2012 Jun 21;18(23):3032-4. This new multidisciplinary and multistakeholder approach proved to be well-accepted, and the “WEF method” is already recognized as a milestone in the Italian HTA landscape, by Institutions (e.g. AIFA and Italian MoH), Scientific Societies and pharma industries, thus helping payers in making rational decisions based on HTA methods. This is the proof that HTA, if well built and following a scientific evidence-based process, is a very useful tool that, considering all aspects concerning the healthcare system, may pragmatically improve prescriptive appropriateness of drugs/technologies and facilitate access to cures. 7) Cammà C, Petta S, Enea M, Bruno R, Bronte F, Capursi V, Cicchetti A, Colombo GL, Di Marco V, Gasbarrini A, Craxì A; WEF Study Group. Cost-effectiveness of boceprevir or telaprevir for untreated patients with genotype 1 chronic hepatitis C. Hepatology. 2012 Sep;56(3):850-60. 8) Cammà C, Cabibbo G, Petta S, Enea M, Iavarone M, Grieco A, Gasbarrini A, Villa E, Zavaglia C, Bruno R, Colombo M, Craxì A; WEF study group; SOFIA study group. Cost-effectiveness of sorafenib treatment in field practice for patients with hepatocellular carcinoma. Hepatology. 2013 Mar;57(3):1046-54. 9) Cammà C, Petta S, Cabibbo G, Ruggeri M, Enea M, Bruno R, Capursi V, Gasbarrini A, Alberti A, Craxì A; WEF Study Group. Cost-effectiveness of boceprevir or telaprevir for previously treated patients with genotype 1 chronic hepatitis C. J Hepatol. 2013 Oct;59(4):658-66. 10) Ruggeri M, Coretti S, Gasbarrini A, Cicchetti A. Economic assessment of an anti-HCV screening program in Italy. Value Health. 2013 Sep-Oct;16(6):965-72. 3P SOLUTION s.r.l. MILAN - ITALY www.3psolution.it - [email protected] +390236631574
Scarica