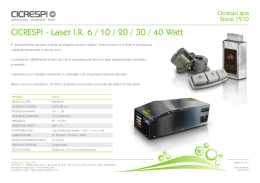
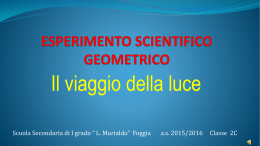
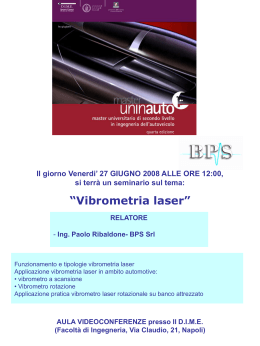
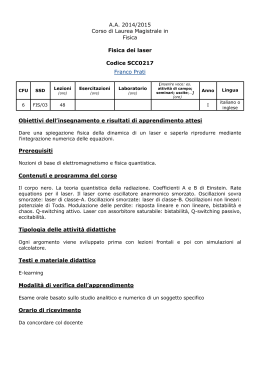
caso clinico Trattamento dell’edema maculare diabetico con bevacizumab intravitreale e fotocoagulazione laser FAG-guidata Treatment of diabetic macular edema with intravitreal bevacizumab and fluorescein angiography guided laser photocoagulation M. Leozappa, T. Micelli Ferrari Riassunto Scopo: valutare l’efficacia della terapia combinata con bevacizumab intravitreale (IVB) e fotocoagulazione laser a guida fluorangiografica nel trattamento dell’edema maculare diabetico (EMD). Metodi: 44 pazienti con EMD; 24 (gruppo A) trattati con IVB (1,25 mg) seguita da fotocoagulazione laser FAG-guidata; 20 pazienti (gruppo B) trattati con sola IVB. Il follow-up è stato di 10 ± 4 mesi. Risultati: un mese dopo il trattamento l’AV era significativamente migliorata e lo spessore medio foveale era diminuito (p < 0,001) in entrambi i gruppi. All’ultimo controllo, nel gruppo A, l’AV era migliorata significativamente (p = 0,01) e il valore medio dello spessore della retina era significativamente diminuito (p < 0,01) rispetto al pre-operatorio; nel gruppo B, il miglioramento morfologico e funzionale non era significativo rispetto al pre-operatorio. Conclusioni: nel trattamento del EMD, il trattamento combinato con bevacizumab e fotocoagulazione laser appaiono garantire una maggiore e più duratura efficacia rispetto alla sola iniezione di bevacizumab. UOC Oculistica, Ospedale Generale Regionale “F. Miulli”, Acquaviva delle Fonti (BA) Parole chiave: edema maculare diabetico, bevacizumab, Fotocoagulazione laser FAG-guidata. Summary Background: to evaluate the efficacy of combined therapy with intravitreal bevacizumab (IVB) and fluorescein angiography (FA)-guided-laser photocoagulation for the treatment of diabetic macular edema (DME). Methods: 44 patients with DME: 24 (group A) were treated with IVB (1.25 mg) and FA-guided laser photocoagulation; 20 patients (group B) were treated with IVB alone. Follow-up was 10 ± 4 months. Results: one month after treatment mean visual acuity (VA) was improved, and mean retinal thickness was significantly decreased in both groups (from 284 µm to 209 µm). At the last control visit, in group A the mean VA was significantly improved (p = 0.01), and mean retinal thickness was significantly (p < 0.01) decreased compared to preoperative values; in group B, the improvement of retinal thickness and VA were not statistically different from preoperative values. Conclusion: a greater and longer lasting efficacy may be expected when bevacizumab is combined with FA-guided laser photocoagulation in the treatment of DME. Key words: diabetic macular edema; bevacizumab; FA-guided laser photocoagulation. Indirizzo per la corrispondenza: Marco Leozappa UOC Oculistica, Ospedale Generale Regionale “F. Miulli” SP127, km 4,1 70021 Acquaviva delle Fonti (BA) Fax +39 0831 951439 E-mail: [email protected] 33 M. Leozappa, T. Micelli Ferrari. Introduzione Materiali e metodi L’edema maculare diabetico (EMD) è la più importante causa di perdita visiva nei pazienti diabetici. Il beneficio della fotocoagulazione laser per il trattamento dell’EMD è stato dimostrato nell’ETDRS Study: la fotocoagulazione focale è efficace nel ridurre il rischio di moderata perdita visiva, con bassa incidenza di effetti avversi 1 2. In questo studio erano utilizzati sia il trattamento laser focale diretto verso singoli microaneurismi sia il laser a griglia per le aree di leakage diffuso e non perfusione capillare. Tuttavia, i pazienti mostravano un minimo miglioramento visivo dopo il trattamento laser; il 12% degli occhi sviluppano una moderata perdita visiva in 3 anni, nonostante il trattamento 3. Diversi studi hanno dimostrato l’efficacia di iniezione intravitreale di triamcinolone acetonide (TA) associato o meno a fotocoagulazione laser 4-6. Il trattamento con TA, con o senza laser a griglia, mostrerebbe migliori risultati anatomo-funzionali rispetto al solo trattamento laser 7. Tuttavia, non vi sono differenze significative in termini di spessore foveale e di acuità visiva tra occhi trattati con solo TA e occhi trattati con TA+ laser 8. La maggior parte delle complicazioni legate al diabete, come l’edema maculare e neovascolarizzazione, si verificano a seguito del rilascio di fattori di crescita in risposta alla ischemia retinica. Il VEGF stimola l’infiammazione inducendo l’espressione della molecola di adesione intracellulare-1 (ICAM-1), e l’adesione dei leucociti 9. L’inibizione della attività VEGF è in grado di prevenire la neovascolarizzazione retinica e le anomalie del flusso sanguigno associate. L’uso di bevacizumab endovitreale ha dimostrato efficacia nel trattamento dell’edema maculare diabetico cronico diffuso 10: la riduzione di spessore retinico centrale può essere osservato a lungo dopo ripetute iniezioni intravitreali di bevacizumab. La FAG è molto utile, perché l’uso dell’angiogramma durante la fotocoagulazione laser può migliorare la precisione del trattamento 11. La nostra ipotesi iniziale era che, effettuando il trattamento sequenziale con bevacizumab intravitreale e fotocoagulazione laser a guida FAG, i 2 meccanismi agissero in sinergia, aumentando gli effetti benefici in termini di riduzione dell’EMD. Abbiamo effettuato questo studio per confrontare l’efficacia della terapia sequenziale con bevacizumab e FA-guidate fotocoagulazione laser con la sola iniezione di bevacizumab intravitreale nel trattamento dell’EMD. Lo studio ha compreso 44 pazienti con edema maculare diabetico diffuso (28 donne e 16 uomini), reclutati tra ottobre 2007 e novembre 2008. L’età media era di 64 anni (range 53-75). Sono stati selezionati pazienti con EMD che coinvolgeva la fovea, come definizione di “edema maculare clinicamente significativo” secondo le linee guida ETDRS. La diagnosi di EMD è stata fatta dopo osservazione diretta con biomicroscopia, FAG (HRA Heidelberg Engineering, Heidelberg, Germania), e Tomografia a Coerenza Ottica (OCT; StratusOCT, Carl Zeiss, Dublin, CA). Per ogni paziente l’AV è stata misurata utilizzando la ETDRS chart a 4 metri e calcolata in scala logaritmica (LogMAR). Il consenso informato è stato ottenuto da tutti i pazienti dopo spiegazione delle finalità e dei possibili rischi di studio. I pazienti sono stati randomizzati in 2 gruppi di trattamento: il gruppo A (24 pazienti) è stato trattato con protocollo terapeutico sequenziale, mediante iniezione intravitreale di 1,25 mg di bevacizumab via pars plana, seguita, dopo 7 ± 2 giorni, da fotocoagulazione laser FAG-guidata; il gruppo B (20 pazienti) è stato trattato con una sola iniezione intravitreale di bevacizumab. Dopo il trattamento, i pazienti sono stati osservati a 1 giorno e 1, 2, 4, 8, 12, 24 e 36 settimane. Tutti i pazienti hanno completato almeno 24 settimane di follow-up. Sono state valutate essenzialmente le variazioni di spessore foveale e, secondariamente le variazioni dell’AV. Ad ogni visita, i pazienti sottoposti a visita oculistica completa, determinazione della migliore acuità visiva corretta (VA), esame con lampada a fessura, misurazione della pressione intraoculare, biomicroscopia della macula, la misurazione dello spessore retinico mediante OCT, FAG, fotografia del fondo oculare. 34 Risultati I dati pre- e post-operatori sono riassunti nelle Figure 1-4. Nel pre-operatorio lo spessore foveale e l’acuità visiva non avevano differenze significative. Lo spessore foveale medio era di 291 ± 37 micron nel gruppo A e 282 ± 32 micron nel gruppo B; l’acuità visiva media era 0,84 ± 0,15 LogMAR nel gruppo A e 0,71 ± 0,13 LogMAR nel gruppo B. caso clinico Fig. 1. Valori (media e range) di spessore maculare nei pazienti del gruppo A, al t0, t1 e t2 – Macular thickness (mean and range) in Group A, at t0, t1 and t2. Fig. 2. Valori (media e range) di spessore maculare nei pazienti del gruppo B, al t0, t1 e t2 – Macular thickness (mean and range) in Group B, at t0, t1 and t2. 1 mese dopo il trattamento (t1), lo spessore foveale era significativamente diminuito a 224 ± 33 m nel gruppo A (p < 0,01), ed a 197 ± 38 m nel gruppo B (p < 0,01). In entrambi i gruppi, l’AV era migliorata significativamente: 0,72 ± 0,13 LogMAR nel gruppo A (p < 0,1), e 0,65 ± 0,08 LogMAR nel gruppo B (p = 0,1). Non si rilevavano differenze statisticamente significative tra i gruppi in quanto a miglioramento di spessore e di visus (p = 0,1 per AV; p = 0,08 per spessore foveale). Tuttavia, all’ultimo controllo (t2), in media 10 mesi post-trattamento, i risultati hanno mostrato differenze significative tra i 2 gruppi. Lo spessore foveale del gruppo A era 207 ± 27 m; in confronto con i valori pre-trattamento, vi era una differenza statisticamente significativa, in termini di riduzione di edema maculare (p < 0,01). L’AV del gruppo A era 0,70 ± 0,11 LogMAR, notevolmente migliorata rispetto al baseline (p = 0,01). Nel gruppo B, il miglioramento funzionale ed anatomico appariva soltanto temporaneo: lo spessore foveale era 270 ± 28 m, mentre l’AV era 0,68 ± 0,16 LogMAR. In confronto con i valori pre-trattamento, non vi era differenza statistica sia di spessore foveale che di acuità visiva. Non sono stati registrati, durante lo studio, eventi avversi oculari (compresi endoftalmite) o sistemici (cerebrovascolari, attacchi ischemici transitori, infarti del miocardio, o malattia vascolare periferica) degni di nota. Discussione Fig. 3. Andamento (media e range) di acuità visiva nei pazienti dl gruppo A (LogMAR), al t0, t1 e t2 – Visual acuity of patients of group A at t0, t1 and t2. Fig. 4. Andamento (media e range) di acuità visiva nei pazienti del gruppo B (LogMAR), al t0, t1 e t2 – Visual acuity of patients of group B at t0, t1 and t2. L’edema maculare diabetico è una delle principali cause di perdita visiva nei pazienti diabetici. Negli ultimi anni, le strategie di trattamento sono state riviste per includere, oltre la fotocoagulazione laser, le farmacoterapie e la chirurgia. L’obiettivo della fotocoagulazione laser è focalizzato principalmente sul trattamento delle zone di fuoriuscita diffuse e non perfusione capillare come individuati sulla fluorangiografia. Negli ultimi anni, vi è stato un grande interesse per i fattori vasoproliferativi, che inducono neovascolarizzazione. È dimostrato che l’ischemia retinica stimola una neovascolarizzazione patologica mediata da fattori angiogenici, come il fattore di crescita vascolare endoteliale (VEGF), prodotto da cellule dell’epitelio pigmentato retinico, da periciti e da cellule endoteliali della retina. Numerosi studi clinici sulla iniezione intravitreale 35 M. Leozappa, T. Micelli Ferrari. di anti-VEGF nell’EMD (pegaptanib sodico, ranibizumab e bevacizumab) hanno mostrato risultati favorevoli 10-15. La nostra ipotesi era che associare l’iniezione di bevacizumab alla fotocoagulazione laser potesse dare migliori e più duraturi effetti rispetto alla sola iniezione di bevacizumab. Nel nostro studio, la fotocoagulazione laser focale è stata eseguita circa 7 ± 2 giorni dopo l’iniezione intravitreale di bevacizumab, con l’obiettivo di trattare le zone di ischemia o perdita evidenziate dalla fluorangiografia. Mentre ad 1 mese i risultati non erano differenti tra i 2 gruppi di pazienti, le differenze più importanti sono state evidenziate nel corso dei mesi successivi, in quanto il gruppo che era stato sottoposto a terapia combinata mostrava un visus ed uno spessore foveale stabile, mentre i pazienti trattati con solo bevacizumab mostravano maggiore tendenza alla recidiva di edema maculare e a conseguente perdita visiva. È emerso, pertanto, che la terapia combinata (bevacizumab + fotocoagulazione laser) può essere superiore al solo bevacizumab intravitreale nel ridurre l’edema maculare e migliorare l’acuità visiva per un tempo più lungo. Uno studio multicentrico randomizzato con lungo follow-up è necessario per valutare sicurezza ed efficacia di questo trattamento sequenziale in tempi ancor superiori. Introduction term decrease of central retinal thickness is observed following repeated intravitreal injections of bevacizumab. FA is of major importance since the use of projected angiogram during laser photocoagulation may improve the precision of treatment 11. We hypothesized that by performing both intravitreal bevacizumab and FA-guided laser photocoagulation, the two mechanisms might act synergistically, increasing the beneficial effects of reduction of macular edema. This study compared the efficacy of sequential therapy with bevacizumab and FA-guided laser photocoagulation versus intravitreal bevacizumab alone for the treatment of DME. Diabetic Macular Edema (DME) is the most important cause of visual loss in patients with diabetes; the benefits of laser photocoagulation for the treatment of DME has been demonstrated in the Early Treatment Diabetic Retinopathy Study (ETDRS): focal photocoagulation is effective in reducing the risk of moderate visual loss, with a low incidence of adverse effects 1 2. The ETDRS used direct focal laser treatment to target individual microaneurysms and applied a grid pattern to areas of diffuse leakage and capillary non-perfusion as identified by fluorescein angiography (FA). However, patients had only minimal visual improvement after laser treatment; 12% of eyes developed moderate visual loss at 3 years despite treatment 3. Several studies have demonstrated the effectiveness of intravitreal injection of triamcinolone acetonide (TA) associated or not with previous grid laser photocoagulation 4-6. TA with or without additional grid laser led to significantly greater reduction in macular edema and better mean final visual acuity VA than eyes treated with laser alone 7. However, no significant differences in foveal thickness and VA were found between the intravitreal TA–alone group and those treated with combined intravitreal TA and laser at any time point 8. Most of diabetes-related complications, such as macular edema and neovascularization, occur secondary to the release of the growth factors in response to retinal ischemia. VEGF promotes inflammation by inducing intracellular adhesion molecule-1 (ICAM-1) expression and leukocyte adhesion 9. Inhibition of VEGF activity can prevent retinal neovascularization and associated blood flow abnormalities. The use of the intravitreal anti-VEGF drug bevacizumab has been shown to be effective for the treatment of chronic diffuse diabetic macular edema 10, and a long- 36 Nessun interesse economico da parte degli autori su quanto esposto nell’articolo. Materials and methods This was a clinical trial involving 44 patients with diffuse diabetic macular edema (28 women and 16 men), recruited between October 2007 and November 2008. Mean age was 64 years (range 53-75). Patients were enrolled if they had DME involving the fovea, as defined by clinically significant macular edema according to ETDRS guidelines. Diagnosis of macular edema was made after direct observation by biomicroscopy, Fluorescein angiography (HRA 2 Heidelberg Engineering, Heidelberg,Germany), and optical coherence tomography (OCT; StratusOCT, Carl Zeiss, Dublin, CA). For each patient the best corrected visual acuity (BCVA) was measured using the ETDRS chart at a distance of 4 m and calculated as the logarithm of the minimum angle of resolution (LogMAR). Informed consent was obtained from all patients after explanation of the purpose and possible risks of the study. Patients were randomized into 2 treatment groups: group A (24 patients) was treated with sequential therapeutic protocol using intravitreal injection of 1.25 mg of beva- caso clinico cizumab via pars plana followed, after 7 ± 2 days, by FAguided laser photocoagulation; group B (20 patients) was treated with intravitreal injection of bevacizumab alone. After treatment, patients were observed on day 1, and at 1, 2, 4, 8, 12, 24 and 36 weeks after intervention. All patients completed 24 weeks of follow-up. The primary outcome measure was change in foveal thickness on OCT, while the secondary outcome measure was BCVA. At each visit, patients underwent complete eye examination, determination of BCVA, slit-lamp examination, intraocular pressure measurement, stereoscopic biomicroscopy of the macula, retinal thickness measurement by OCT, FA and fundus photography. Results Patient characteristics are summarized in Figures. 1-4. The baseline characteristics (t0) of foveal thickness and VA were not significantly different between groups. Mean foveal thickness before treatment was 291 µm in group A and 279 µm in group B; mean VA was 0.84 LogMAR in group A and 0.72 LogMAR in group B. One month after treatment (t1), foveal thickness measured by OCT was significantly decreased in both group A (p < 0.01; mean 223 µm) and group B (p < 0.01; mean 195 µm). In both groups, the BCVA improved significantly, from 0.84 to 0.72 LogMAR in group A (p < 0.1), and from 0.72 to 0.65 LogMAR in group B (p = 0.1). No statistically significant difference was between the groups (p = 0.1 for BCVA; p = 0.08 for foveal thickness). At last control after treatment (t2), there were significant differences between the 2 groups. Mean foveal thickness of group A was 203 µm, which was statistically different compared to pre-treatment values reduction of macular edema (p < 0.01). Mean VA of group A was 0.69 LogMAR, which was significantly improved versus baseline (p = 0.01). In group B, functional and anatomical improvement appeared only transient: 6 months after treatment, mean foveal thickness of group B was 268 µm; mean VA was 0.72 LogMAR. Comparing with pre-treatment values, there was no statistically significant difference in foveal thickness and VA, both gradually deteriorated to baseline levels within 24 weeks. During the study, no ocular side effects or systemic adverse events such as thromboembolic events were encountered. Discussion Diabetic macular edema is a major cause of visual loss in patients with diabetes. In the last years, treatment strategies have been revised to include, in addition to laser photocoagulation, pharmacotherapies and early surgical intervention. The aim of laser photocoagulation has focused primarily on the treatment of areas of diffuse leakage and capillary non-perfusion as identified by FA. In recent years, there has been an interest in vasoproliferative factors, which induce neovascularization. It has been shown that retinal ischemia stimulates pathologic neovascularization mediated by angiogenic factors, such as vascular endothelial growth factor (VEGF), which is released by retinal pigment epithelium, pericytes and endothelial cells of the retina. Clinical studies on the effect of intravitreally administered anti-VEGF aptamer, pegaptanib sodium and antibodies, ranibizumab and bevacizumab on DME has shown favorable results 10-15. Our hypothesis was that the sequential association of bevacizumab plus laser photocoagulation would have benefits in reduction of macular edema compared to injection of bevacizumab alone. In the present study, focal laser photocoagulation was performed at 7 ± 2 days after intravitreal injection of bevacizumab, with the aim to treat areas of ischemia or leakage evidenced by FA. The results at one month after treatment showed no significant difference between the two patient groups. Both the bevacizumab-alone and the combined-therapy groups showed a significant decrease of foveal thickness, which was associated with improvement of VA. However, more important differences were evident at 6 months after treatment: the combined-treatment group showed a greater stability of VA and reduction of foveal thickness; during follow-up, patients treated with bevacizumab alone showed a higher tendency of recurrence of macular edema and of a decrease in visual function. We found that combined therapy (bevacizumab plus laser photocoagulation) appeared to be superior to intravitreal bevacizumab alone in reducing macular thickening and in improving visual acuity in patients with diabetes for a longer time interval. Evaluation in a multicenter, randomized, controlled clinical trial with longer follow-up is warranted to evaluate the safety and efficacy of this sequential treatment. 37 M. Leozappa, T. Micelli Ferrari. Bibliografia 1 Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmol 1985;103:1796-806. Triamcinolone or laser alone for Treating Diabetic Macular Edema. Ophthalmol 2007;114:2162-7. 9 Ishida S, Usui T, Yamashiro K. VEGF164 is pro inflammatory in the diabetic retina. Invest Ophthalmol Vis Sci 2003;44:2155-62. 2 Bandello F, Lanzetta P, Menchini U. When and how to do a grid laser for diabetic macular edema. Doc Ophthalmol 1999;97:415-9. 10 Kook D, Wolf A, Kreutzer T, et al. Long-term effect of intravitreal bevacizumab (avastin) in patients with chronic diffuse diabetic macular edema. Retina 2008;228:1053-60. 3 Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy (ETDRS report number 9). Ophthalmol 1991;98:766-85. 11 4 Martidis A, Duker JS, Greenberg PB, et al. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmol 2002;109:920-7. Kylstra JA, Brown JC, Jaffe GJ. The importance of fluorescein angiography in planning laser treatment of diabetic macular edema. Ophthalmol 1999;106:206873. 12 Cunningham ET Jr, Adamis AP, Altaweel M, et al. A phase II randomized double-masked trial of pegaptanib: An anti-vascular endothelial growth factor aptamer, for diabetic macular edema. Ophthalmol 2005;112:174757. 13 Nguyen QD, Tatlipinar S, Shah SM, et al. Vascular endothelial growth factor is a critical stimulus for diabetic macular edema. Am J Ophthamol 2006;142:961-9. 14 Chun DW, Heier JS, Topping TM, e al. A pilot study of multiple intravitreal injections of ranibizumab in patients with center involving clinically significant macular edema. Ophthalmol 2006;113:1706-12. 15 Haritoglou C, Kook D, Neubauer A, et al. Intravitreal bevacizumab (Avastin) therapy for persistent diffuse diabetic macular edema. Retina 2006;26:999-1005. 5 Karacorlu M, Ozdemir H, Karacorlu S, et al. Intravitreal triamcinolone as a primary therapy in diabetic macular oedema. Eye 2005;19:382-6. 6 Lam DS, Chan CK, Tang EW, et al. Intravitreal triamcinolone for diabetic macular oedema in Chinese patients: six-month prospective longitudinal pilot study. Clin Experiment Ophthalmol 2004;32:569-72. 7 8 Avitabile T, Longo A, Reibaldi A. Intravitreal triamcinolone compared with macular laser grid photocoagulation for the treatment of cystoid macular edema. Am J Ophthalmol 2005;140:695-702. Lam DS, Chan CK, Mohamed S et al. Intravitreal Triamcinolone plus Sequential Grid laser versus 38
Scaricare