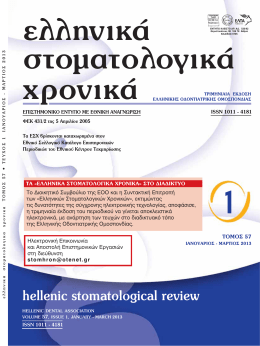
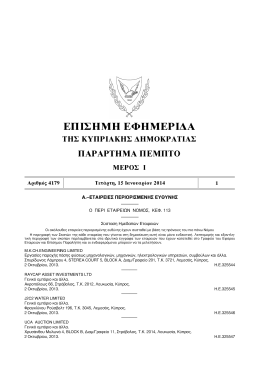
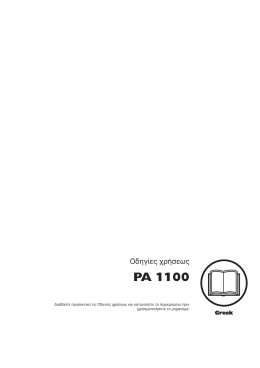
¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ ·ÓÙÈÌÂÙÒÈÛË ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fi fiÓÓÙˆÓ AÚÈÛÙ›‰Ë˜ B. M¤ÏÎÔ˜,1 Mfi fiÛ Û¯Ô˜ A. ¶··‰fi fiÔ˘ÏÔ˜2 ªÂÙ·Ù˘¯È·Îfi˜ ÊÔÈÙËÙ‹˜, ∂ÚÁ·ÛÙ‹ÚÈÔ √ÚıÔ‰ÔÓÙÈ΋˜, ∆Ì‹Ì· √‰ÔÓÙÈ·ÙÚÈ΋˜, ∞ÚÈÛÙÔÙ¤ÏÂÈÔ ¶·ÓÂÈÛÙ‹ÌÈÔ £ÂÛÛ·ÏÔӛ΢. ∂›ÎÔ˘ÚÔ˜ ∫·ıËÁËÙ‹˜ & ™˘ÓÙÔÓÈÛÙ‹˜ ÙÔ˘ ªÂÙ·Ù˘¯È·ÎÔ‡ ¶ÚÔÁÚ¿ÌÌ·ÙÔ˜, ∂ÚÁ·ÛÙ‹ÚÈÔ √ÚıÔ‰ÔÓÙÈ΋˜, ∆Ì‹Ì· √‰ÔÓÙÈ·ÙÚÈ΋˜, ∞ÚÈÛÙÔÙ¤ÏÂÈÔ ¶·ÓÂÈÛÙ‹ÌÈÔ £ÂÛÛ·ÏÔӛ΢. 1 2 Periodontal aspects associated with the surgical and orthodontic treatment of impacted canines Aristides B. Melkos,1 Moschos A. Papadopoulos 2 Postgraduate student, Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece. Assistant Professor & Postgraduate Program Coordinator, Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece. 1 2 ¶EPI§HæH ABSTRACT √È ¤ÁÎÏÂÈÛÙÔÈ Î˘Ófi‰ÔÓÙ˜ ·ÔÙÂÏÔ‡Ó Û˘ÓËıÈṲ̂ÓÔ Â‡ÚËÌ· Û ·ÛıÂÓ›˜ Ô˘ ÂÈ˙ËÙÔ‡Ó ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›·. ∏ ·ÓÙÈÌÂÙÒÈÛ‹ ÙÔ˘˜ ··ÈÙ› Û˘Ó‹ıˆ˜ Û˘ÓÂÚÁ·Û›· ÌÂٷ͇ ¯ÂÈÚÔ˘ÚÁÔ‡ ÛÙfiÌ·ÙÔ˜, ÔÚıÔ‰ÔÓÙÈÎÔ‡ Î·È ÂÚÈÔ‰ÔÓÙÔÏfiÁÔ˘. ∏ ÔÚıÔ‰ÔÓÙÈ΋ ÚÔÛ¤ÁÁÈÛË ¤¯ÂÈ ˆ˜ ÛÙfi¯Ô ÙË ÌÂٷΛÓËÛË ÙÔ˘ ˘·›ÙÈÔ˘ ‰ÔÓÙÈÔ‡ ÛÙË ÛˆÛÙ‹ ÙÔ˘ ı¤ÛË ÛÙÔ Ô‰ÔÓÙÈÎfi ÙfiÍÔ ¯ˆÚ›˜ ÚfiÎÏËÛË ÂÚÈÔ‰ÔÓÙÈÎÒÓ ÚÔ‚ÏËÌ¿ÙˆÓ. ∏ ›Ù¢ÍË ‚¤ÏÙÈÛÙ˘ ÂÚÈÔ‰ÔÓÙÈ΋˜ ÛÙ‹ÚÈ͢ ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ‰ÔÓÙÈÔ‡ ÂÍ·ÚÙ¿Ù·È ·fi ÙËÓ ·Ú¯È΋ ÙÔ˘ ı¤ÛË Î·È ·fi ÙÔ Â›‰Ô˜ Ù˘ ¯ÂÈÚÔ˘ÚÁÈ΋˜ Î·È ÔÚıÔ‰ÔÓÙÈ΋˜ Ù¯ÓÈ΋˜ Ô˘ ı· ¯ÚËÛÈÌÔÔÈËı›. ™ÎÔfi˜ ·˘Ù‹˜ Ù˘ ÂÚÁ·Û›·˜ ‹Ù·Ó Ó· Á›ÓÂÈ ÌÈ· ÎÚÈÙÈ΋ ·Ó·ÛÎfiËÛË ÙˆÓ ÂÚÈÔ‰ÔÓÙÈÎÒÓ ·Ú·Ì¤ÙÚˆÓ Î·Ù¿ ÙËÓ ·ÓÙÈÌÂÙÒÈÛË ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Î·È ÙˆÓ ·ÓÙ›ÛÙÔȯˆÓ ÔÚıÔ‰ÔÓÙÈÎÒÓ Î·È ¯ÂÈÚÔ˘ÚÁÈÎÒÓ Ù¯ÓÈÎÒÓ. ∆Ô Û˘Ì¤Ú·ÛÌ· Ô˘ ÚÔ·ÙÂÈ Â›Ó·È fiÙÈ ÙÔ ÂÚÈÔ‰fiÓÙÈÔ ÙˆÓ ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ ÂËÚ¿˙ÂÙ·È Û¯Â‰fiÓ ¿ÓÙ·, ·ÓÂÍ¿ÚÙËÙ· ·fi ÙȘ ¯ÂÈÚÔ˘ÚÁÈΤ˜ ‹ ÔÚıÔ‰ÔÓÙÈΤ˜ ‰È·‰Èηۛ˜. ∂Ó ÙÔ‡ÙÔȘ, Ê·›ÓÂÙ·È fiÙÈ ÔÈ ÎÏÂÈÛÙ¤˜ ¯ÂÈÚÔ˘ÚÁÈΤ˜ Ù¯ÓÈΤ˜ ·ÔÎ¿Ï˘„˘ ÙˆÓ ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ, ‰ËÏ·‰‹ ·Ó‡„ˆÛË ¯ÂÈÚÔ˘ÚÁÈÎÔ‡ ÎÚËÌÓÔ‡, Û˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘ Î·È Â·Ó·Û˘ÚÚ·Ê‹ ÙÔ˘ ÎÚËÌÓÔ‡ ÛÙË ı¤ÛË ÙÔ˘, ÂÁ΢ÌÔÓÔ‡Ó ÙÔ˘˜ ÏÈÁfiÙÂÚÔ˘˜ ÎÈÓ‰‡ÓÔ˘˜ ÁÈ· ÙÔ ÂÚÈÔ‰fiÓÙÈÔ. Impacted canines are a common finding in patients seeking orthodontic treatment. The management of impacted canines usually requires cooperation between oral surgery, orthodontics and periodontology. The orthodontic approach aims in moving the corresponding tooth into its correct position in the dental arch without causing periodontal problems. Optimum periodontal support is related to initial position of the impacted tooth as well as to the type of the surgical and orthodontic technique used. Aim of this paper was to critically review the periodontal interactions in reference to the management of impacted canines and the corresponding orthodontic and surgical techniques used. It can be concluded that the periodontal condition of treating impacted canines is almost always affected not-depending from the surgical or orthodontic procedures used. However, it seems that less damaging effects on the periodontium should anticipated when using the closed-surgical exposure techniques, which involve raising of a surgical flap, bonding of an attachment and finally resuturing of the flap to its original position. §∂•∂π™ ∫§∂π¢π∞: ŒÁÎÏÂÈÛÙÔÈ Î˘Ófi‰ÔÓÙ˜, ¯ÂÈÚÔ˘ÚÁÈ΋ ¤̂·ÛË, ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›·, ÂÚÈÔ‰fiÓÙÈÔ ∂ÏÏ √ÚıÔ‰ ∂Èı 2004;7:9-24. ¶·ÚÂÏ‹ÊıË: 15.01.2003 - ŒÁÈÓ ‰ÂÎÙ‹: 26.03.2003 KEY WORDS: impacted canines, surgery, orthodontic treatment, periodontium Hell Orthod Rev 2004;7:9-24. Received: 15.01.2003 - Accepted: 26.03.2003 EI™A°ø°H INTRODUCTION √È ¤ÁÎÏÂÈÛÙÔÈ Î˘Ófi‰ÔÓÙ˜ ·ÔÙÂÏÔ‡Ó Û˘ÓËıÈṲ̂ÓÔ Â‡ÚËÌ· Û ·ÛıÂÓ›˜ Ô˘ ÂÈ˙ËÙÔ‡Ó ÔÚıÔ‰ÔÓÙÈ΋ ıÂÚ·- Impacted canines are a common finding in patients seeking orthodontic treatment. Great differences are E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 9 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ observed among researchers concerning the frequency of impaction and location of the impacted teeth, but it is generally agreed that the most frequently impacted teeth are the third molars followed by the maxillary canines (Papadopoulos et al. 2001). Impacted maxillary canines constitute about 18% of all impacted teeth (Wolf and Matilla, 1979) and represent 0,9% of all maxillary canines while the incident of mandibular canine impaction is 0,35% (Dachi and Howell, 1961). Each patient with an impacted canine must undergo a comprehensive evaluation of the malocclusion. Depending on the exact position of the impacted tooth, the prognosis for its orthodontic movement and placement in a normal position in the dental arch can vary widely (Elefteriadis and Athanasiou, 1996). According to Bishara (1992) and to Kokich and Mathews (1993), by managing impacted canines the clinician should consider the various treatment options available for the patient, including the following: (a) no treatment if the patient does not desire it and if there is absence of any pathologic changes, (b) auto transplantation of the canine (Shaw et al., 1981; Sayne et al., 1986), (c) extraction of the impacted canine and movement of the first premolar in its position (replacement of the impacted canine by the first premolar), (d) extraction of the canine and posterior segmental osteotomy to move the buccal segment mesially to close the residual space (Maloney, 1985), (e) prosthetic replacement of the canine, and (f) surgical exposure of the canine and orthodontic treatment to bring the tooth into the line of occlusion. The last option which is obviously the most desirable approach, aims in bringing the tooth into its correct position in the dental arch without causing any periodontal damage. Although numerous surgical techniques have been used in the management of unerupted teeth, there has been little documentation of the influences of such surgeries and of orthodontic treatment on the periodontal tissues of these teeth (Heasman et al., 1996). On the other hand, although several studies have shown that the periodontal status after orthodontic movement of impacted teeth is related to the position of the impacted tooth as well as to the type of the surgical and orthodontic technique used, there is still controversy about these issues. Aim of this paper was to critically review the periodontal interactions in reference to the management of impacted canines and the corresponding orthodontic and surgical techniques used. ›·. √È ‰È¿ÊÔÚÔÈ ÂÚ¢ÓËÙ¤˜ ‰È·ÊˆÓÔ‡Ó ÌÂٷ͇ ÙÔ˘˜ Û¯ÂÙÈο Ì ÙË Û˘¯ÓfiÙËÙ· ¤ÁÎÏÂÈÛ˘ Î·È ÙËÓ ÂÓÙfiÈÛË ÙˆÓ ¤ÁÎÏÂÈÛÙˆÓ ‰ÔÓÙÈÒÓ, ÁÂÓÈο fï˜ Û˘ÌʈÓÔ‡Ó fiÙÈ Ù· ‰fiÓÙÈ· Ô˘ Â›Ó·È Û˘¯ÓfiÙÂÚ· ¤ÁÎÏÂÈÛÙ· Â›Ó·È ÔÈ ÙÚ›ÙÔÈ ÁÔÌÊ›ÔÈ ·ÎÔÏÔ˘ıÔ‡ÌÂÓÔÈ ·fi ÙÔ˘˜ ¿Óˆ ΢Ófi‰ÔÓÙ˜ (Papadopoulos Î·È Û˘Ó., 2001). √È ¤ÁÎÏÂÈÛÙÔÈ ¿Óˆ ΢Ófi‰ÔÓÙ˜ ·ÔÙÂÏÔ‡Ó ÂÚ›Ô˘ 18% ÙÔ˘ Û˘ÓfiÏÔ˘ ÙˆÓ ÂÁÎÏ›ÛÙˆÓ ‰ÔÓÙÈÒÓ (Wolf Î·È Matilla, 1979) Î·È 0.9% fiÏˆÓ ÙˆÓ ¿Óˆ ΢ÓÔ‰fiÓÙˆÓ, ÂÓÒ Ë Û˘¯ÓfiÙËÙ· ¤ÁÎÏÂÈÛ˘ ÙˆÓ Î¿Ùˆ ΢ÓÔ‰fiÓÙˆÓ Â›Ó·È 0.35% (Dachi Î·È Howell, 1961). ™Â οı ·ÛıÂÓ‹ Ì ¤ÁÎÏÂÈÛÙÔ Î˘Ófi‰ÔÓÙ· Ú¤ÂÈ Ó· Á›ÓÂÈ Û˘ÓÔÏÈ΋ ·ÍÈÔÏfiÁËÛË Ù˘ Û‡ÁÎÏÂÈÛ˘. ∞Ó¿ÏÔÁ· Ì ÙËÓ ·ÎÚÈ‚‹ ı¤ÛË ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ‰ÔÓÙÈÔ‡ ÔÈΛÏÏÂÈ Ë ÚfiÁÓˆÛË ÁÈ· ÙËÓ ÔÚıÔ‰ÔÓÙÈ΋ ÌÂٷΛÓËÛË Î·È ‰È¢ı¤ÙËÛ‹ ÙÔ˘ ÛÂ Ê˘ÛÈÔÏÔÁÈ΋ ı¤ÛË ÛÙÔ ÙfiÍÔ (Elefteriadis Î·È Athanasiou, 1996). ™‡Ìʈӷ Ì ÙÔÓ Bishara (1992) Î·È ÙÔ˘˜ Kokich Î·È Mathews (1993), ηٿ ÙËÓ ·ÓÙÈÌÂÙÒÈÛË ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ, Ô ÎÏÈÓÈÎfi˜ ı· Ú¤ÂÈ Ó· ·ÍÈÔÏÔÁ‹ÛÂÈ ÙȘ ‰È¿ÊÔÚ˜ ıÂڷ¢ÙÈΤ˜ ÂÈÏÔÁ¤˜ Ô˘ ¤¯ÂÈ Ô ·ÛıÂÓ‹˜ Û˘ÌÂÚÈÏ·Ì‚·ÓÔÌ¤ÓˆÓ ÙˆÓ ·Ú·Î¿Ùˆ: (·) ·ÔÊ˘Á‹ ıÂڷ›·˜, ÂÊfiÛÔÓ ‰ÂÓ ÙÔ ÂÈı˘Ì› Ô ·ÛıÂÓ‹˜ Î·È ÂÊfiÛÔÓ ·Ô˘ÛÈ¿˙Ô˘Ó ·ıÔÏÔÁÈΤ˜ ·ÏÏÔÈÒÛÂȘ, (‚) ·˘ÙÔÌÂÙ·ÌfiÛ¯Â˘ÛË ÙÔ˘ ΢Ófi‰ÔÓÙ· (Shaw Î·È Û˘Ó., 1981; Sayne Î·È Û˘Ó., 1986), (Á) ÂÍ·ÁˆÁ‹ ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ΢Ófi‰ÔÓÙ· Î·È ÌÂٷΛÓËÛË ÙÔ˘ ÚÒÙÔ˘ ÚÔÁÔÌÊ›Ô˘ ÛÙË ı¤ÛË ÙÔ˘ (·ÓÙÈηٿÛÙ·ÛË ÙÔ˘ ΢Ófi‰ÔÓÙ· ·fi ÙÔÓ ÚÒÙÔ ÚÔÁfiÌÊÈÔ), (‰) ÂÍ·ÁˆÁ‹ ÙÔ˘ ΢Ófi‰ÔÓÙ· Î·È Ô›ÛıÈ· ÙÌËÌ·ÙÈ΋ ÔÛÙÂÔÙÔÌ›· ÁÈ· ÂÁÁ‡˜ ÌÂٷΛÓËÛË ÙÔ˘ ·ÚÂÈ·ÎÔ‡ ÙÌ‹Ì·ÙÔ˜ ÒÛÙ ӷ ÎÏ›ÛÂÈ ÙÔ ÎÂÓfi Ù˘ ÂÍ·ÁˆÁ‹˜ (Maloney, 1985), (Â) ÚÔÛıÂÙÈ΋ ·ÓÙÈηٿÛÙ·ÛË ÙÔ˘ ΢Ófi‰ÔÓÙ· Î·È (ÛÙ) ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ÙÔ˘ ΢Ófi‰ÔÓÙ· Î·È ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›· ÁÈ· Ó· ÙÔÔıÂÙËı› ÙÔ ‰fiÓÙÈ Û ı¤ÛË Û‡ÁÎÏÂÈÛ˘. ∏ ÙÂÏÂ˘Ù·›· ÂÈÏÔÁ‹, Ë ÔÔ›· ·ÔÙÂÏ›, ÚÔÊ·ÓÒ˜, Î·È ÙËÓ Ï¤ÔÓ ÂÈı˘ÌËÙ‹ ÚÔÛ¤ÁÁÈÛË, ¤¯ÂÈ ˆ˜ ÛÙfi¯Ô Ó· ʤÚÂÈ ÙÔ ‰fiÓÙÈ ÛÙË ÛˆÛÙ‹ ÙÔ˘ ı¤ÛË ÛÙÔ ÙfiÍÔ ¯ˆÚ›˜ ÚfiÎÏËÛË ÂÚÈÔ‰ÔÓÙÈ΋˜ ‚Ï¿‚˘. ¶·ÚfiÏÔ Ô˘ ¤¯Ô˘Ó ¯ÚËÛÈÌÔÔÈËı› ‰È¿ÊÔÚ˜ ¯ÂÈÚÔ˘ÚÁÈΤ˜ Ù¯ÓÈΤ˜ ÁÈ· ÙËÓ ·ÓÙÈÌÂÙÒÈÛË ‰ÔÓÙÈÒÓ Ô˘ ‰ÂÓ ¤¯Ô˘Ó ·Ó·Ù›ÏÂÈ, Ë Â›‰Ú·ÛË ÙˆÓ ÂÂÌ‚¿ÛÂˆÓ Î·È Ù˘ ÔÚıÔ‰ÔÓÙÈ΋˜ ıÂڷ›·˜ ÛÙÔ˘˜ ÂÚÈÔ‰ÔÓÙÈÎÔ‡˜ ÈÛÙÔ‡˜ ·˘ÙÒÓ ÙˆÓ ‰ÔÓÙÈÒÓ Â›Ó·È ·Ó·ÚÎÒ˜ ÙÂÎÌËÚȈ̤ÓË ‚È‚ÏÈÔÁÚ·ÊÈο (Heasman Î·È Û˘Ó., 1996). ∞fi ÙËÓ ¿ÏÏË ÏÂ˘Ú¿, ·ÚfiÏÔ Ô˘ ·ÚÎÂÙ¤˜ ÌÂϤÙ˜ ¤¯Ô˘Ó ‰Â›ÍÂÈ fiÙÈ Ë ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË ÌÂÙ¿ ÙËÓ ÔÚıÔ‰ÔÓÙÈ΋ ÌÂٷΛÓËÛË ÙˆÓ ÂÁÎÏ›ÛÙˆÓ ÂÍ·ÚÙ¿Ù·È ·fi ÙË ı¤ÛË ÙˆÓ ‰ÔÓÙÈÒÓ ·˘ÙÒÓ Î·È ÙÔ Â›‰Ô˜ Ù˘ ¯ÂÈÚÔ˘ÚÁÈ΋˜ Î·È ÔÚıÔ‰ÔÓÙÈ΋˜ Ù¯ÓÈ΋˜ Ô˘ ·ÎÔÏÔ˘ı‹ıËÎÂ, ÂÍ·ÎÔÏÔ˘ı› Ó· ˘¿Ú¯ÂÈ ‰È¯ÔÁӈ̛· Û¯ÂÙÈο Ì ·˘Ù¿ Ù· ı¤Ì·Ù·. E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment PALATALLY IMPACTED CANINES Palatally impacted canines rarely erupt of their own, without surgical intervention (Jacoby, 1983). There are 10 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ ™Ùfi¯Ô˜ Ù˘ ÂÚÁ·Û›·˜ Â›Ó·È Ó· Á›ÓÂÈ ÎÚÈÙÈ΋ ·Ó·ÛÎfiËÛË ÙˆÓ ÂÚÈÔ‰ÔÓÙÈÎÒÓ ÚÔ‚ÏËÌ¿ÙˆÓ Ô˘ ·ÊÔÚÔ‡Ó ÛÙËÓ ·ÓÙÈÌÂÙÒÈÛË ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Î·È ÛÙȘ ·ÓÙ›ÛÙÔȯ˜ ÔÚıÔ‰ÔÓÙÈΤ˜ Î·È ¯ÂÈÚÔ˘ÚÁÈΤ˜ Ù¯ÓÈΤ˜ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È. numerous surgical methods for exposing the impacted canine and moving it to the line of occlusion. Many different variations have been suggested concerning these surgical procedures, from the more radical exposure (Lappin, 1951; Azaz et al., 1980) to the minimal one (Hunt, 1977). According to Bishara (1992) and to Pearson et al. (1997), two of the most commonly used methods are: (a) the simple surgical exposure and (b) the surgical exposure with placement of an auxiliary orthodontic attachment. Y¶EPøIA E°K§EI™TOI KYNO¢ONTE™ √È ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙÔÈ Î˘Ófi‰ÔÓÙ˜ Û·Ó›ˆ˜ ·Ó·Ù¤ÏÏÔ˘Ó ÌfiÓÔÈ ÙÔ˘˜, ¯ˆÚ›˜ ‰ËÏ·‰‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·Ú¤Ì‚·ÛË (Jacoby, 1983). À¿Ú¯Ô˘Ó ‰È¿ÊÔÚ˜ ¯ÂÈÚÔ˘ÚÁÈΤ˜ ̤ıÔ‰ÔÈ ÁÈ· ·ÔÎ¿Ï˘„Ë ÙˆÓ ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Î·È ÌÂٷΛÓËÛ‹ ÙÔ˘˜ Û ı¤ÛË Û‡ÁÎÏÂÈÛ˘. Œ¯Ô˘Ó ÚÔÙ·ı› ‰È¿ÊÔÚ˜ ÙÚÔÔÔÈ‹ÛÂȘ ÙˆÓ ¯ÂÈÚÔ˘ÚÁÈÎÒÓ ‰È·‰ÈηÛÈÒÓ, ·fi ÙËÓ Ï¤ÔÓ ÚÈ˙È΋ ·ÔÎ¿Ï˘„Ë (Lappin, 1951; Azaz Î·È Û˘Ó., 1980) ˆ˜ ÙËÓ ÂÏ¿¯ÈÛÙ· ÂÂÌ‚·ÙÈ΋ Ù¯ÓÈ΋ (Hunt, 1977). ™‡Ìʈӷ Ì ÙÔÓ Bishara (1992) Î·È ÙÔ˘˜ Pearson Î·È Û˘Ó. (1997), ‰‡Ô ·fi ÙȘ ϤÔÓ ¯ÚËÛÈÌÔÔÈÔ‡ÌÂÓ˜ ÌÂıfi‰Ô˘˜ ›ӷÈ: (·) Ë ·Ï‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë Î·È (‚) Ë ·ÔÎ¿Ï˘„Ë Î·È ÙÔÔı¤ÙËÛË ‚ÔËıËÙÈÎÔ‡ ÔÚıÔ‰ÔÓÙÈÎÔ‡ Û˘Ó‰¤ÛÌÔ˘. Simple surgical exposure The philosophic belief on which the first method is based, in that the majority of teeth will erupt if all bony or soft tissue impringement or any other obstructions are removed from the path of eruption (Clark, 1971). This method is most useful when the canine has a correct axial inclination and does not need to be uprighted during its eruption. A favorable axial inclination of the tooth is more frequent in labially impacted teeth; the palatally impacted teeth are in more horizontal/oblique direction (Theofanatos et al., 1994). Surgical exposure with placement of an auxiliary attachment Regarding the surgical exposure with placement of an auxiliary orthodontic attachment, there are generally two approaches recommended in regard to the timing of placing the attachment: (a) the one-step approach and (b) the two-step approach. The one-step approach According to the one-step approach the orthodontic attachment is placed on the tooth at the time of surgical exposure (Becker et al., 1982) using either an openor a closed-surgical exposure (McSherry, 1996). Regarding the open surgical exposure, a gingival flap is reflected and the bone over the crown is removed. The soft tissue in the flap is excised and a window to expose the crown of the impacted tooth is created. Then the flap is re-approximated and after bonding of an orthodontic attachment a periodontal dressing is placed in order to prevent the window from closing (Fig.1). According to Becker et al. (1996), the onestep approach is superior to the two-step-approach; the ability to gain attachment permits a more conservative approach to the exposure. However, the palatal mucosa is very thick and will leave a broad cut surface, which will tend to close over unless its edges are more radically trimmed back and the dental follicle is removed. Thus, when the tooth is placed deeply, the exposure will additionally need to be maintained using a surgical pack. This type of approach will therefore leave the tooth with a soft tissue deficiency and a long clinical crown at the completion of the orthodontic alignment (Becker, 1998). ∞Ï‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ∆Ô ıˆÚËÙÈÎfi ˘fi‚·ıÚÔ Ù˘ ÚÒÙ˘ ÌÂıfi‰Ô˘ ‚·Û›˙ÂÙ·È ÛÙËÓ ¿Ô„Ë fiÙÈ Ë ÏÂÈÔ„ËÊ›· ÙˆÓ ‰ÔÓÙÈÒÓ ı· ·Ó·Ù›ÏÂÈ, ÂÊfiÛÔÓ ·ÔÌ·ÎÚ˘Óı› ÔÔÈ·‰‹ÔÙ ·ÚÂÌ‚ÔÏ‹ ·fi ÔÛÙfi ‹ Ì·Ï·ÎÔ‡˜ ÈÛÙÔ‡˜ ‹ ¿ÏÏÔ ÂÌfi‰ÈÔ ·fi ÙËÓ Ô‰fi ·Ó·ÙÔÏ‹˜ (Clark, 1971). ∏ ̤ıÔ‰Ô˜ ·˘Ù‹ ¤¯ÂÈ Ì¤ÁÈÛÙË ¯ÚËÛÈÌfiÙËÙ· fiÙ·Ó Ô Î˘Ófi‰ÔÓÙ·˜ ¤¯ÂÈ ÛˆÛÙ‹ ·ÍÔÓÈ΋ ÎÏ›ÛË Î·È ‰ÂÓ ··ÈÙÂ›Ù·È ·ÓfiÚıˆÛË Î·Ù¿ ÙËÓ ·Ó·ÙÔÏ‹ ÙÔ˘. ∂˘ÓÔ˚΋ fï˜ ·ÍÔÓÈ΋ ÎÏ›ÛË ÙÔ˘ ΢Ófi‰ÔÓÙ· ··ÓÙ¿Ù·È Û˘¯ÓfiÙÂÚ· Û ·ÚÂȷο ¤ÁÎÏÂÈÛÙ· ‰fiÓÙÈ·. ∆· ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙ· ‰fiÓÙÈ· ¤¯Ô˘Ó Ì¿ÏÏÔÓ ÔÚÈ˙fiÓÙÈ·/ÏÔÍ‹ ‰È‡ı˘ÓÛË (Theofanatos Î·È Û˘Ó., 1994). ∞ÔÎ¿Ï˘„Ë Î·È ÙÔÔı¤ÙËÛË ‚ÔËıËÙÈÎÔ‡ Û˘Ó‰¤ÛÌÔ˘ ™¯ÂÙÈο Ì ÙËÓ ·ÔÎ¿Ï˘„Ë Î·È ÙÔÔı¤ÙËÛË ‚ÔËıËÙÈÎÔ‡ ÔÚıÔ‰ÔÓÙÈÎÔ‡ Û˘Ó‰¤ÛÌÔ˘, ˘¿Ú¯Ô˘Ó ÁÂÓÈο ‰‡Ô ÚÔÛÂÁÁ›ÛÂȘ, fiÛÔÓ ·ÊÔÚ¿ ÛÙÔ ¯ÚfiÓÔ ÙÔÔı¤ÙËÛ˘ ÙÔ˘ Û˘Ó‰¤ÛÌÔ˘: (·) Ë Ù¯ÓÈ΋ ÂÓfi˜ ÛÙ·‰›Ô˘ Î·È (‚) Ë Ù¯ÓÈ΋ ‰‡Ô ÛÙ·‰›ˆÓ. ∆¯ÓÈ΋ ÂÓfi fi˜˜ ÛÙ·‰›Ô˘ ™‡Ìʈӷ Ì ·˘Ù‹ ÙËÓ Ù¯ÓÈ΋, Ô ÔÚıÔ‰ÔÓÙÈÎfi˜ Û‡Ó‰ÂÛÌÔ˜ ÙÔÔıÂÙÂ›Ù·È ÛÙÔ ‰fiÓÙÈ Î·Ù¿ ÙÔÓ ¯ÚfiÓÔ Ù˘ ¯ÂÈÚÔ˘ÚÁÈ΋˜ ·ÔÎ¿Ï˘„˘ (Becker Î·È Û˘Ó., 1982), ›Ù Ì ·ÓÔȯً ›Ù Ì ÎÏÂÈÛÙ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋ (McSherry, 1996). ∫·Ù¿ ÙËÓ ·ÓÔȯً ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë, ·Ó·ÛËÎÒÓÂÙ·È ¤Ó·˜ Ô˘ÏÈÎfi˜ ÎÚËÌÓfi˜ Î·È ·Ê·ÈÚÂ›Ù·È ÔÛÙfi ¿Óˆ E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment 11 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ ·fi ÙË Ì‡ÏË ÙÔ˘ ‰ÔÓÙÈÔ‡. ∞Ê·ÈÚÂ›Ù·È Ô Ì·Ï·Îfi˜ ÈÛÙfi˜ ÙÔ˘ ÎÚËÌÓÔ‡ Î·È ‰ËÌÈÔ˘ÚÁÂ›Ù·È ·Ú¿ı˘ÚÔ ·ÔÎ¿Ï˘„˘ Ù˘ ̇Ï˘ ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ‰ÔÓÙÈÔ‡. ∞ÎÔÏÔ˘ı› Â·Ó·Û˘ÌÏËÛ›·ÛË ÙÔ˘ ÎÚËÌÓÔ‡ Î·È ÌÂÙ¿ ÙË Û˘ÁÎfiÏÏËÛË ÔÚıÔ‰ÔÓÙÈÎÔ‡ Û˘Ó‰¤ÛÌÔ˘ ÛÙÔ ‰fiÓÙÈ ÙÔÔıÂÙÂ›Ù·È ÂÚÈÔ‰ÔÓÙÈ΋ ÎÔÓ›· ÒÛÙ ӷ ÌËÓ ÎÏ›ÛÂÈ ÙÔ ·Ú¿ı˘ÚÔ (EÈÎ. 1). ™‡Ìʈӷ Ì ÙÔ˘˜ Becker Î·È Û˘Ó. (1996), Ë Ù¯ÓÈ΋ ÂÓfi˜ ÛÙ·‰›Ô˘ Â›Ó·È Î·Ï‡ÙÂÚË ·fi ·˘Ù‹ ÙˆÓ ‰‡Ô ÛÙ·‰›ˆÓ. ∏ ‰˘Ó·ÙfiÙËÙ· ΤډԢ˜ ÚfiÛÊ˘Û˘ ÂÈÙÚ¤ÂÈ ÌÈ· ÈÔ Û˘ÓÙËÚËÙÈ΋ ÚÔÛ¤ÁÁÈÛË Ù˘ ·ÔÎ¿Ï˘„˘. ∂Ó ÙÔ‡ÙÔȘ, Ô ˘ÂÚÒÈÔ˜ ‚ÏÂÓÓÔÁfiÓÔ˜ Â›Ó·È Ôχ ·¯‡˜ Î·È ·Ê‹ÓÂÈ Â˘Ú›· ÂÈÊ¿ÓÂÈ· ·ÔÎÔ‹˜ Ì ٿÛË Û‡ÁÎÏÂÈÛ˘ ÙˆÓ ¿ÎÚˆÓ Ù˘, ÂÎÙfi˜ Î·È ·Ó ·˘Ù¿ ·ÔÍÂÛıÔ‡Ó ÈÔ ÚÈ˙Èο Î·È ·Ê·ÈÚÂı› ÙÔ Ô‰ÔÓÙÔı˘Ï¿ÎÈÔ. ŒÙÛÈ, fiÙ·Ó ÙÔ ‰fiÓÙÈ ‚Ú›ÛÎÂÙ·È Û ÌÂÁ¿ÏÔ ‚¿ıÔ˜, Ë ·ÔÎ¿Ï˘„Ë ı· Ú¤ÂÈ ÂÈϤÔÓ Ó· ‰È·ÙËÚËı› Î·È Ì ¯ÂÈÚÔ˘ÚÁÈ΋ ÎÔÓ›·. ∞˘ÙÔ‡ ÙÔ˘ ›‰Ô˘˜ Ë Ù¯ÓÈ΋, ÏÔÈfiÓ, ı· ‰ËÌÈÔ˘ÚÁ‹ÛÂÈ ÛÙÔ ‰fiÓÙÈ ¤ÏÏÂÈÌÌ· Ì·Ï·ÎÒÓ ÈÛÙÒÓ Î·È Ì·ÎÚÈ¿ ÎÏÈÓÈ΋ ̇ÏË ÛÙÔ Ù¤ÏÔ˜ Ù˘ ÔÚıÔ‰ÔÓÙÈ΋˜ ‰È¢ı¤ÙËÛ˘ (Becker, 1998). ∏ ·ÓÔȯً ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋ ·ÚÔ˘ÛÈ¿˙ÂÈ ÔÚÈṲ̂ӷ ÏÂÔÓÂÎÙ‹Ì·Ù·, fiˆ˜ ÙË ‰˘Ó·ÙfiÙËÙ· Ô˘ ¤¯ÂÈ Ô ÔÚıÔ‰ÔÓÙÈÎfi˜ ÁÈ· ·Ú·Ù‹ÚËÛË Î·È Û˘Ó¯‹ ÚfiÛ‚·ÛË ÛÙÔ ¤ÁÎÏÂÈÛÙÔ ‰fiÓÙÈ Î·ı’ fiÏË ÙË ‰È¿ÚÎÂÈ· Ù˘ ÔÚ›·˜ ÙÔ˘ ÚÔ˜ ÙË Ê˘ÛÈÔÏÔÁÈ΋ ÙÔ˘ ı¤ÛË ÛÙÔ Ô‰ÔÓÙÈÎfi ÙfiÍÔ (Wisth Î·È Û˘Ó., 1976b; Vanarsdall Î·È Corn, 1977), ηıÒ˜ Î·È Ù·¯‡ÙÂÚË ·Ó·ÙÔÏ‹ (Vanarsdall Î·È Corn, 1977). ∂Ó ÙÔ‡ÙÔȘ, Ë Ì¤ıÔ‰Ô˜ ·˘Ù‹ Û˘¯Ó¿ Û˘Û¯ÂÙ›˙ÂÙ·È Ì ‰È¿ÊÔÚ· ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù·, fiˆ˜ ˘Ê›˙ËÛË ÙˆÓ Ô‡ÏˆÓ (Vanarsdall Î·È Corn, 1977; Boyd, 1984; Tegsjö Î·È Û˘Ó., 1984; Odenrick Î·È Modeer, 1978), ÔÛÙÈ΋ ·ÒÏÂÈ· (Vanarsdall Î·È Corn, 1977), ÌÂȈ̤ÓÔ Â‡ÚÔ˜ ÎÂÚ·ÙÈÓÔÔÈËÌ¤ÓˆÓ Ô‡ÏˆÓ (Tegsjö Î·È Û˘Ó., 1984, Kohavi Î·È Û˘Ó., 1984b), ηı˘ÛÙ¤ÚËÛË Ù˘ ÂÚÈÔ‰ÔÓÙÈ΋˜ ÂԇψÛ˘ (Becker, 1996) Î·È ÊÏÂÁÌÔÓ‹ ÙˆÓ Ô‡ÏˆÓ (Tegsjö Î·È Û˘Ó., 1984). ∫·Ù¿ ÙËÓ ÎÏÂÈÛÙ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋, ·ÔηχÙÂÙ·È Ë Ì‡ÏË ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ‰ÔÓÙÈÔ‡ Ì ·Ó‡„ˆÛË ÎÚËÌÓÔ‡ ‚ÏÂÓÓÔÁÔÓÔÂÚÈÔÛÙ¤Ô˘, ·Ê·ÈÚÂ›Ù·È ÙÔ ÔÛÙfi Ô˘ ÙËÓ Î·Ï‡ÙÂÈ, Á›ÓÂÙ·È Û˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘ ÛÙÔ ‰fiÓÙÈ Î·È Â·Ó·ÙÔÔı¤ÙËÛË ÙÔ˘ ÎÚËÌÓÔ‡. ™‡ÚÌ· Ì eyelet ‹ ¯Ú˘Û‹ ·Ï˘Û›‰·, Ô˘ Û˘Ó‰¤ÂÙ·È ÛÙÔ ¤Ó· ¿ÎÚÔ Ì ÙÔÓ Û‡Ó‰ÂÛÌÔ, ‰È¤Ú¯ÂÙ·È ‰È· ÙÔ˘ ÎÚËÌÓÔ‡ ̤۷ ÛÙË ÛÙÔÌ·ÙÈ΋ ÎÔÈÏfiÙËÙ· Î·È ÚÔÛ‰¤ÓÂÙ·È ÛÙÔ ¿ÏÏÔ ¿ÎÚÔ ÙÔ˘ ÛÙȘ ·Î›ÓËÙ˜ Û˘Û΢¤˜, ÒÛÙ ӷ ·ÛÎËı› ¿ÌÂÛË ¤ÏÍË (McSherry, 1998). ∂ÎÙfi˜ ·fi Ù· Û‡ÚÌ·Ù· Î·È ÙȘ ·Ï˘Û›‰Â˜, ÁÈ· ÙËÓ ·Ó·ÙÔÏ‹ ¤ÁÎÏÂÈÛÙˆÓ ‰ÔÓÙÈÒÓ ¤¯Ô˘Ó ¯ÚËÛÈÌÔÔÈËı› ηٿ ηÈÚÔ‡˜ ‰È¿ÊÔÚ· ›‰Ë ÔÚıÔ‰ÔÓÙÈÎÒÓ Û˘Ó‰¤Û̈Ó, fiˆ˜ ÎÔ¯ÏÈÔ‡ÌÂÓ˜ ηÚÊ›‰Â˜, ¯˘Ù¿ ¯Ú˘Û¿ ¤ÓıÂÙ·, ¯Ú˘Û¤˜ ηχÙÚ˜ Ì cleats, Û˘ÚÌ¿ÙÈÓ˜ ÚÔÛ‰¤ÛÂȘ, Û˘ÁÎÔÏE§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment The open surgical exposure presents some advantages such as ability of the orthodontist to observe and have a continuing access to the impacted tooth as it is moved to its normal position in the dental arch (Wisth et al., 1976b; Vanarsdall and Corn, 1977), as well as faster eruption (Vanarsdall and Corn, 1977). However, this method is often associated with multiple periodontal problems, such as gingival recession (Vanarsdall and Corn, 1977; Boyd, 1884; Tegsjö et al., 1984; Odenrick and Modeer, 1978), bone loss (Vanarsdall and Corn, 1977), decreased width of keratinized gingiva (Tegsjö et al., 1984; Kohavi et al., 1984b), delayed periodontal healing (Becker, 1996), and gingival inflammation (Tegsjö et al., 1984). Regarding the closed-surgical exposure, a mucoperiosteal flap is raised exposing the crown of the impacted tooth, the bone covering the crown is removed, an attachment is bonded and the flap is repositioned. An eyelet wire or (gold) chain connected to the attachment exits through the flap into the oral cavity to gain attachment to the fixed appliance for immediate traction (McSherry, 1998). In addition to eyelet wires or chains, several other kinds of orthodontic attachments have been used in order to erupt impacted teeth, such as threaded pins, cast gold inlays, gold cups with cleats, ligature wires, bonded attachments, bands, and extracoronal caps. Some of them can produce more damaging effects than others to the periodontium, the impacted tooth, or the adjacent teeth. For example, a threaded pin can damage the pulp of an impacted tooth (Theofanatos et al., 1994), a circumferential ligature wire can cause ankylosis, external resorption, and alveolar bone loss (Shapira and Kuftinek, 1981; Boyd, 1982), while gold cups, inlays, bands, and extracoronal caps require significant bone removal. Wisth et al. (1976a) compared the periodontal status between treated impacted canines which had been moved by means of orthodontic forces and the contralateral control ones, which had erupted unaided, and found that the pocket on the distal surface was significantly deeper in the treated impacted canines. Both the buccal and the palatal surfaces of the previously impacted canines displayed significantly greater loss of attachment than the control teeth did. The significant difference between the loss of attachment on the buccal surface of both the previously impacted canines and the control teeth, confirms the findings of Zachrisson and Alnaes (1974), according to which the pressure side is particularly prone to exhibit periodontal destruction, even when it is not related to an extraction site. Hansson and Rindler (1998) observed an increased depth of the mesio-lingual and mesio-labial pockets of the previously impacted canines which were orthodontically moved after surgical exposure (a flap 12 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment A B C D ∂ÈÎfiÓ· 1. ∞ÓÙÈÌÂÙÒÈÛË ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ì ·ÓÔȯً ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋ ÂÓfi˜ ÛÙ·‰›Ô˘. ∞. ÃÂÈÚÔ˘ÚÁÈ΋ ·Ê·›ÚÂÛË ÙÔ˘ ˘ÂÚÒÈÔ˘ ‚ÏÂÓÓÔÁfiÓÔ˘ ÙÔ˘ ‰ÂÍÈÔ‡ ¿Óˆ ¤ÁÎÏÂÈÛÙÔ˘ ΢Ófi‰ÔÓÙ·. µ. ÃÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë Î·È Û˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘ ÛÙÔ ›‰ÈÔ ‰fiÓÙÈ. C. ÃÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë Î·È Û˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘ ÛÙÔ˘˜ ¿Óˆ ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ ‰ÂÍÈ¿ Î·È ·ÚÈÛÙÂÚ¿. D. ∏ ÔÚıÔ‰ÔÓÙÈ΋ Û˘Û΢‹ ηٿ ÙË ‰È¿ÚÎÂÈ· Ù˘ ÌÂٷΛÓËÛ˘ ÙˆÓ ¿Óˆ ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ. Figure 1. Management of palatally impacted canines with the open surgical exposure in one-step approach. A. Surgical removal of the palatal mucosa of the right upper palatally impacted canine. B. Surgical exposure and attachment bonding of same canine. C. Surgical exposure and attachment bonding of the right and left upper palatally impacted canines. D. Orthodontic appliance insitu during movement of the upper palatally impacted canines. ÏÔ‡ÌÂÓÔÈ Û‡Ó‰ÂÛÌÔÈ, ‰·ÎÙ‡ÏÈÔÈ Î·È ÂÍˆÌ˘ÏÈΤ˜ ηχÙÚ˜. √ÚÈṲ̂ӷ ·fi ·˘Ù¿ ÚÔηÏÔ‡Ó ÌÂÁ·Ï‡ÙÂÚ˜ ‚Ï¿‚˜ ·fi ¿ÏÏ· ÛÙÔ ÂÚÈÔ‰fiÓÙÈÔ, ÛÙÔ ¤ÁÎÏÂÈÛÙÔ ‰fiÓÙÈ ‹ ÛÙ· ·Ú·Î›ÌÂÓ· ‰fiÓÙÈ·. °È· ·Ú¿‰ÂÈÁÌ·, Ë ÎÔ¯ÏÈÔ‡ÌÂÓË Î·ÚÊ›‰· ÌÔÚ› Ó· ‚Ï¿„ÂÈ ÙÔÓ ÔÏÊfi ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ‰ÔÓÙÈÔ‡ (Theofanatos Î·È Û˘Ó., 1994), Ë Û˘ÚÌ¿ÙÈÓË ÚfiÛ‰ÂÛË ‰›ÎËÓ ‚Úfi¯Ô˘ ÌÔÚ› Ó· ÚÔηϤÛÂÈ ·Á·ψÛË, Â͈ÙÂÚÈ΋ ·ÔÚÚfiÊËÛË Î·È ·ÒÏÂÈ· Ê·ÙÓÈ·ÎÔ‡ ÔÛÙÔ‡ (Shapira Î·È Kuftinek, 1981; Boyd, E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 had been raised and resutured after bone removal in 11 of the 42 cases examined), compared to the canines of the untreated contralateral control site. They also noticed that the marginal bone level was significantly lower on the distal surface of the treated canines, but they concluded that in general their results showed a good gingival and periodontal status with slight differences between treated and untreated sides. In a comparison of the probing attachment level between the treated impacted canines and the 13 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ A B untreated contralateral ones, Woloshyn et al. (1994) observed an increased probing attachment level at the mesial and distal aspects of the treated canines, while the crestal bone height was significantly lower at the mesial aspect of the previously impacted canines than at the control ones. These results agree with the findings of Becker et al. (1983), who also observed that the mean pocket depth was significantly greater in the previously impacted teeth and the bone support was also significantly lower on the distal and on the mesial side of these teeth as well. The two-step approach According to the two-step approach (Lewis, 1971), initially the canine is surgically uncovered and then the area is packed with a surgical pack to avoid the filling in of tissues around the tooth. After wound healing, within 2 to 3 weeks, the pack is removed, and an attachment is placed on the uncovered tooth (Fig. 2) (Becker 1998). Boyd (1982) observed that the comparison between the impacted canines treated with the two-step approach and direct bonding and the contralateral non-impacted ones, revealed no clinically significant differences in the mean values of loss of attachment. The same finding was observed in all six tooth sites, where the measurements were taken. However, it must be mentioned that all probing measurements were ended off to the nearest millimeter; thus, only differences greater than 1 mm were clinically significant. Listing of the findings of the various studies concerning the periodontal status of orthodontically treated palatally impacted canines, are presented in Table 1. C ∂ÈÎfiÓ· 2. ∞ÓÙÈÌÂÙÒÈÛË ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ì ·ÓÔȯً ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋ ‰‡Ô ÛÙ·‰›ˆÓ. ∞. ∆ÔÔı¤ÙËÛË Û˘Ó‰¤ÛÌÔ˘ Î·È ÂÊ·ÚÌÔÁ‹ ÔÚıÔ‰ÔÓÙÈÎÒÓ ‰˘Ó¿ÌÂˆÓ Ì ÙÌËÌ·ÙÈÎfi ÙfiÍÔ ÌÂÙ¿ ÙË ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë, ¤ÙÛÈ ÒÛÙ ӷ ˘ÂÚÂÎÊ˘ı› Ô Î˘Ófi‰ÔÓÙ·˜. µ. ∏ ·Ú¯È΋ ‰È‡ı˘ÓÛË Ù˘ ‰‡Ó·Ì˘ Â›Ó·È Ù¤ÙÔÈ· Ô˘ Ó· ·ÔÌ·ÎÚ‡ÓÂÈ ÙÔ ‰fiÓÙÈ ·fi Ù· ·Ú·Î›ÌÂÓ· ÒÛÙ ·˘Ù¿ Ó· ÌËÓ ÙÚ·˘Ì·ÙÈÛÙÔ‡Ó Î·È ÁÈ· ÙÔ ÏfiÁÔ ·˘Ùfi ÌÂÙ·‚¿ÏÏÂÙ·È Ë ‰È‡ı˘ÓÛË ÂÊ·ÚÌÔÁ‹˜ Ù˘ ‰‡Ó·Ì˘ ÚÔ˜ Ù· ¿ˆ ‰È·Ì¤ÛÔ˘ ÂÏ·ÛÙÈ΋˜ ·Ï˘Û›‰·˜ ·fi ÙÔÓ ÁψÛÛÈÎfi ÛˆÏËÓ›ÛÎÔ ÙÔ˘ ‰·ÎÙ˘Ï›Ô˘ ÙÔ˘ ÚÒÙÔ˘ ÁÔÌÊ›Ô˘. C. ¶ÂÚ·ÈÙ¤Úˆ ·ÏÏ·Á‹ Ù˘ ‰‡Ó·Ì˘ ÚÔ˜ ·ÚÂȷ΋ ηÙ‡ı˘ÓÛË ‰È·Ì¤ÛÔ˘ ‰‡Ô ÂÏ·ÛÙÈÎÒÓ ·Ï˘Û›‰ˆÓ ·fi ÙÔÓ ÁψÛÛÈÎfi ÛˆÏËÓ›ÛÎÔ ÙÔ˘ ‰·ÎÙ˘Ï›Ô˘ ÙÔ˘ ÚÒÙÔ˘ ÁÔÌÊ›Ô˘ Î·È ·fi ÙÔ Û˘ÚÌ¿ÙÈÓÔ ÙfiÍÔ. Figure 2. Management of palatally impacted canines with the open surgical exposure in two-step approach. A. Placement of attachment and application of orthodontic forces by means of a sectional arch following surgical exposure in order to extrude the canine. B. The initial direction of the force should be to move the tooth away from the neighboring teeth to avoid their injury and therefore a change in force application in distal direction is performed by means of an elastic chain attached to the lingual sheath of the first molar band. C. Further change in force application in buccal direction by means of two elastic chains attached to the lingual sheath of the first molar band and to the archwire. E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment LABIALLY IMPACTED CANINES The most common methods of uncovering labial impacted canines are: (a) the simple surgical exposure, (b) the closed-flap eruption technique, and 14 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ (c) the apically positioned flap technique (Clark, 1971; Shiloah and Kopezyk, 1978; Vanarsdall and Corn, 1977; Hunt, 1977; Boyd, 1984; McSherry, 1998). According to Becker (1998), there is also one more method to add, namely the relief of crowding, if that was the cause of the canine displacement. 1982), ÂÓÒ ÔÈ ¯Ú˘Û¤˜ ηχÙÚ˜, Ù· ¤ÓıÂÙ·, ÔÈ ‰·ÎÙ‡ÏÈÔÈ Î·È ÔÈ ÂÍˆÌ˘ÏÈΤ˜ ηχÙÚ˜ ··ÈÙÔ‡Ó ÛËÌ·ÓÙÈ΋ ·Ê·›ÚÂÛË ÔÛÙÔ‡. √È Wisth Î·È Û˘Ó. (1976a) Û˘Ó¤ÎÚÈÓ·Ó ÙËÓ ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË ıÂÚ·Â˘Ì¤ÓˆÓ ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ÌÂÙ·ÎÈÓ‹ıËÎ·Ó Ì ÔÚıÔ‰ÔÓÙÈΤ˜ ‰˘Ó¿ÌÂȘ Î·È ÙˆÓ ·ÓÙ›ÛÙÔȯˆÓ ‰ÔÓÙÈÒÓ Ù˘ ¿ÏÏ˘ ÏÂ˘Ú¿˜ Ô˘ ›¯·Ó ·Ó·Ù›ÏÂÈ ¯ˆÚ›˜ ·Ú¤Ì‚·ÛË Î·È ‚Ú‹Î·Ó fiÙÈ Ô ı‡Ï·ÎÔ˜ Ù˘ ¿ˆ ÂÈÊ¿ÓÂÈ·˜ ‹Ù·Ó ÛËÌ·ÓÙÈο ‚·ı‡ÙÂÚÔ˜ ÛÙÔ˘˜ ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ ÛÙÔ˘˜ ÔÔ›Ô˘˜ ›¯Â Á›ÓÂÈ ıÂڷ›·. ∆fiÛÔ Ë ·ÚÂȷ΋ fiÛÔ Î·È Ë ˘ÂÚÒÈ· ÂÈÊ¿ÓÂÈ· ÙˆÓ ÚÒËÓ ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ ·ÚÔ˘Û›·˙·Ó ÛËÌ·ÓÙÈο ÌÂÁ·Ï‡ÙÂÚË ·ÒÏÂÈ· ÚfiÛÊ˘Û˘ Û ۯ¤ÛË Ì ٷ ‰fiÓÙÈ· ÂϤÁ¯Ô˘. ∏ ÌÂÁ¿ÏË ‰È·ÊÔÚ¿ ÌÂٷ͇ Ù˘ ·ÒÏÂÈ·˜ ÚfiÛÊ˘Û˘ ÛÙËÓ ·ÚÂȷ΋ ÂÈÊ¿ÓÂÈ· ÙfiÛÔ ÙˆÓ ÚÒËÓ ¤ÁÎÏÂÈÛÙˆÓ ‰ÔÓÙÈÒÓ fiÛÔ Î·È ÙˆÓ ‰ÔÓÙÈÒÓ ÂϤÁ¯Ô˘ ÂȂ‚·ÈÒÓÂÈ Ù· Â˘Ú‹Ì·Ù· ÙˆÓ Zachrisson Î·È Alnaes (1974), Û‡Ìʈӷ Ì ٷ ÔÔ›· Ë ÏÂ˘Ú¿ Ô˘ ‰¤¯ÂÙ·È ›ÂÛË Â›Ó·È È‰È·›ÙÂÚ· ÂÈÚÚ‹˜ Û ÂÚÈÔ‰ÔÓÙÈ΋ ηٷÛÙÚÔÊ‹, ·ÎfiÌË Î·È fiÙ·Ó ‰ÂÓ Û¯ÂÙ›˙ÂÙ·È Ì ı¤ÛË ÂÍ·ÁˆÁ‹˜. √È Hansson Î·È Rindler (1998) ·Ú·Ù‹ÚËÛ·Ó ·‡ÍËÛË ÙÔ˘ ‚¿ıÔ˘˜ ÙÔ˘ ÂÁÁ‡˜-ÁψÛÛÈÎÔ‡ Î·È ÂÁÁ‡˜·ÚÂÈ·ÎÔ‡ ı˘Ï¿ÎÔ˘ ÛÙÔ˘˜ ÚÒËÓ ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ô˘ ÌÂÙ·ÎÈÓ‹ıËÎ·Ó ÔÚıÔ‰ÔÓÙÈο ÌÂÙ¿ ·fi ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë (¤ÁÈÓ ·Ó‡„ˆÛË ÎÚËÌÓÔ‡ Î·È Â·Ó·Û˘ÚÚ·Ê‹ ÌÂÙ¿ ·fi ·Ê·›ÚÂÛË ÔÛÙÔ‡ ÛÙȘ 11 ·fi ÙȘ 42 ÂÚÈÙÒÛÂȘ Ô˘ ÂÍÂÙ¿ÛıËηÓ) Û ۯ¤ÛË Ì ÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ù˘ ¿ÏÏ˘ ÏÂ˘Ú¿˜ fiÔ˘ ‰ÂÓ ¤ÁÈÓ ıÂڷ›·. ¶·Ú·Ù‹ÚËÛ·Ó ·ÎfiÌË fiÙÈ ÙÔ Â›Â‰Ô ÙÔ˘ ÔÛÙÔ‡ Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜ ‹Ù·Ó ÛËÌ·ÓÙÈο ¯·ÌËÏfiÙÂÚÔ ÛÙËÓ ¿ˆ ÂÈÊ¿ÓÂÈ· ÙˆÓ ıÂÚ·Â˘Ì¤ÓˆÓ Î˘ÓÔ‰fiÓÙˆÓ. ™˘Ì¤Ú·Ó·Ó, fï˜, fiÙÈ Î·Ù¿ ηÓfiÓ· Ù· ·ÔÙÂϤÛÌ·Ù¿ ÙÔ˘˜ ‰Â›¯ÓÔ˘Ó Î·Ï‹ Ô˘ÏÈ΋ Î·È ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË Ì Ôχ ÌÈÎÚ¤˜ ‰È·ÊÔÚ¤˜ ÌÂٷ͇ Ù˘ ıÂÚ·Â˘Ì¤Ó˘ ÏÂ˘Ú¿˜ Î·È Ù˘ ÏÂ˘Ú¿˜ ÂϤÁ¯Ô˘. ™‡ÁÎÚÈÛË ÙÔ˘ ÌÂÙÚÔ‡ÌÂÓÔ˘ ÂȤ‰Ô˘ ÚfiÛÊ˘Û˘ Ì ÂÚÈÔ‰ÔÓÙÈ΋ Ì‹ÏË ÌÂٷ͇ ıÂÚ·Â˘Ì¤ÓˆÓ ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Î·È ·ÓÙ›ÛÙÔȯˆÓ ‰ÔÓÙÈÒÓ ÂϤÁ¯Ô˘ ·fi ÙÔ˘˜ Woloshyn Î·È Û˘Ó. (1994) ¤‰ÂÈÍ ·˘ÍË̤ÓË ÙÈÌ‹ ̤ÙÚËÛ˘ ÂÁÁ‡˜ Î·È ¿ˆ ÙˆÓ ıÂÚ·Â˘Ì¤ÓˆÓ Î˘ÓÔ‰fiÓÙˆÓ, ÂÓÒ ÙÔ ‡„Ô˜ ÙÔ˘ ÔÛÙÔ‡ Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜ ‹Ù·Ó ÛËÌ·ÓÙÈο ÌÂȈ̤ÓÔ ÛÙËÓ ÂÁÁ‡˜ ÂÈÊ¿ÓÂÈ· ÙˆÓ ÚÒËÓ ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Û ۯ¤ÛË Ì ٷ ‰fiÓÙÈ· ÂϤÁ¯Ô˘. ∆· ·ÔÙÂϤÛÌ·Ù· ·˘Ù¿ Û˘ÌʈÓÔ‡Ó Ì ٷ Â˘Ú‹Ì·Ù· ÙˆÓ Becker Î·È Û˘Ó. (1983), ÔÈ ÔÔ›ÔÈ Â›Û˘ ·Ú·Ù‹ÚËÛ·Ó fiÙÈ ÙÔ Ì¤ÛÔ ‚¿ıÔ˜ ı˘Ï¿ÎÔ˘ ‹Ù·Ó ÛËÌ·ÓÙÈο ÌÂÁ·Ï‡ÙÂÚÔ ÛÙ· ÚÒËÓ ¤ÁÎÏÂÈÛÙ· ‰fiÓÙÈ· Î·È Ë ÔÛÙÈ΋ ÛÙ‹ÚÈÍË ·ÍÈÔÛËÌ›ˆÙ· ÌÂȈ̤ÓË ÛÙȘ ÂÁÁ‡˜ Î·È ¿ˆ ÂÈÊ¿ÓÂȘ ·˘ÙÒÓ ÙˆÓ ‰ÔÓÙÈÒÓ. E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment Simple surgical exposure The simple surgical exposure includes the excision of the covering tissues of the crown of the impacted tooth. Fournier et al. (1982) suggested that labially impacted canines with a favorable vertical position may be treated initially by surgical exposure without the application of a traction force. They believe that in younger patients the tooth will erupt on its own after surgical exposure, whereas in older patients traction is almost always indicated. Tegsjö et al. (1984) observed that the width of keratinized gingiva of the treated canines with a simple but "radical" surgical exposure alone was significantly reduced compared to the contralateral normally erupted canines. In addition, the sulcus depth of the treated canines was significantly lower and the gingival recession was significant increased in comparison to the contralateral control ones. Boyd (1984) compared the "window approach" (exposure of the entire labial aspect of the anatomic crown with total excision of the keratinized tissue), with a more conservative surgical approach which exposed only 4-5 mm of the most superficial portion of the labial aspect of the cusp, maintaining 2-3 mm of keratinized tissue. Evaluation of twelve patients in each category six months to two years after orthodontic alignment revealed that those treated by the window approach presented statistically more gingival recession, gingival inflammation and loss of attachment on the labial and labio-proximal surfaces of the impacted teeth when compared to controls. These findings were confirmed also by Kohavi et al. (1984b) and by Artun et al. (1986), who found significantly less attached gingiva and loss of attachment on labially erupting maxillary canines after their orthodontic alignment. The closed-flap eruption technique In the closed-eruption technique a flap is elevated, an attachment is placed on the impacted tooth, and then the flap is returned to its original location (Fig. 3) (Gaulis and Joho, 1978; Kokich and Mathews, 1993). Vermette et al. (1995) observed that the width of the attached gingiva of the labially impacted canines treated with the closed-eruption technique, was reduced on the distal surface and the crestal bone was located more apically on their facial surface of them than of the untreated control canines. Crescini et al. (1994) reported on the periodontal effects of the closed surgical technique with tunnel traction for deep 15 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ ∆¯ÓÈ΋ ‰‡Ô ÛÙ·‰›ˆÓ ™‡Ìʈӷ Ì ÙËÓ Ù¯ÓÈ΋ ·˘Ù‹ (Lewis, 1971), ηْ ·Ú¯‹Ó ·ÔηχÙÂÙ·È ¯ÂÈÚÔ˘ÚÁÈο Ô Î˘Ófi‰ÔÓÙ·˜ Î·È ÙÔÔıÂÙÂ›Ù·È ÛÙËÓ ÂÚÈÔ¯‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ÎÔÓ›· ÒÛÙ ӷ ÌËÓ Î·Ï˘Êı› ÙÔ ‰fiÓÙÈ ·fi ÙÔ˘˜ Á‡Úˆ ÈÛÙÔ‡˜. ªÂÙ¿ ÙËÓ ÂԇψÛË ÙÔ˘ ÙÚ·‡Ì·ÙÔ˜ ÂÓÙfi˜ 2-3 ‚‰ÔÌ¿‰ˆÓ, ·Ê·ÈÚÂ›Ù·È Ë ÎÔÓ›· Î·È Û˘ÁÎÔÏÏ¿Ù·È ÛÙÔ ‰fiÓÙÈ ÔÚıÔ‰ÔÓÙÈÎfi˜ Û‡Ó‰ÂÛÌÔ˜ (∂ÈÎ. 2) (Becker, 1998). √ Boyd (1982) ·Ú·Ù‹ÚËÛ fiÙÈ Î·Ù¿ ÙË Û‡ÁÎÚÈÛË ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì Ù¯ÓÈ΋ ‰‡Ô ÛÙ·‰›ˆÓ Î·È ¿ÌÂÛË Û˘ÁÎfiÏÏËÛË Î·È ÌË ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ù˘ ¿ÏÏ˘ ÏÂ˘Ú¿˜ ‰ÂÓ ‚Ú¤ıËÎ·Ó ÎÏÈÓÈο ÛËÌ·ÓÙÈΤ˜ ‰È·ÊÔÚ¤˜ ÛÙȘ ̤Û˜ ÙÈ̤˜ ·ÒÏÂÈ·˜ ÚfiÛÊ˘Û˘. ∆Ô ›‰ÈÔ ·Ú·ÙËÚ‹ıËÎÂ Î·È ÛÙȘ ¤ÍÈ ı¤ÛÂȘ Û fiÏ· Ù· ‰fiÓÙÈ· ÛÙ· ÔÔ›· ¤ÁÈÓ·Ó ÌÂÙÚ‹ÛÂȘ. ∂Ó ÙÔ‡ÙÔȘ, Ú¤ÂÈ Ó· ÛËÌÂȈı› fiÙÈ fiϘ ÔÈ ÌÂÙÚ‹ÛÂȘ Ì ÙËÓ ÂÚÈÔ‰ÔÓÙÈ΋ Ì‹ÏË ÛÙÚÔÁÁ˘ÏÔÔÈ‹ıËÎ·Ó ÚÔ˜ ÙÔ ÏËÛȤÛÙÂÚÔ ¯ÈÏÈÔÛÙfi. ŒÙÛÈ, ÌfiÓÔ ‰È·ÊÔÚ¤˜ ÌÂÁ·Ï‡ÙÂÚ˜ ÙÔ˘ ÂÓfi˜ ¯ÈÏÈÔÛÙÔ‡ ‹Ù·Ó ÎÏÈÓÈο ÛËÌ·ÓÙÈΤ˜. ™ÙÔÓ ¶›Ó·Î· 1 ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È Ù· Â˘Ú‹Ì·Ù· ‰È·ÊfiÚˆÓ ÌÂÏÂÙÒÓ Û¯ÂÙÈο Ì ÙËÓ ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË ÙˆÓ ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›·. A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment infra-osseous labially impacted canines. They found no attachment loss and no recession at the end of active treatment and after three years follow-up. In addition, no significant differences were observed in the width of keratinized tissue between the surgically uncovered and the contralateral spontaneous erupted canines. The apically positioned flap technique In the apically repositioned flap technique, a partial thickness flap is raised and the wound is carefully curetted to remove the dental sac and to expose the tooth. There is no need for bone removal unless it is necessary to reach the canine crown. The latter must be executed as conservatively as possible and not beyond the cemento-enamel-junction. Interrupted periosteal sutures are placed to position the flap apically and the surgical area is packed for 7-10 days (Theofanatos et al.,1994). According to Becker (1998), when an apically repositioned flap is performed, tooth eruption is speeded up. This method is not recommended if the impacted tooth is very high positioned, since the apically repositioned flap would then leave a wide area of the labial bony plate unnecessarily exposed to the oral environment. Nevertheless, an important advantage of this method is that the buccally impacted canine remains accessible for attachment bonding at any appropriate later date, if the orthodontist decides for an active extrusion. Regarding the periodontal conditions following use of this technique, Vermette et al. (1995) found that the gingival margin of labially impacted canines uncovered with the apically positioned flap technique was located more apically on the mesial and facial surfaces, and more bone was lost on the mesial, facial and distal surfaces than in the control canines. On the contrary, Tegsjö et al. (1984) observed no significant differences in the periodontal status between treated canines and the non-treated contralaterals (Table 2). ¶APEIAKA E°K§EI™TOI KYNO¢ONTE™ √È Û˘ÓËı¤ÛÙÂÚ˜ ̤ıÔ‰ÔÈ ·ÔÎ¿Ï˘„˘ ·ÚÂȷο ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Â›Ó·È: (·) Ë ·Ï‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë, (‚) Ë Ù¯ÓÈ΋ ·Ó·ÙÔÏ‹˜ Ì ÎÏÂÈÛÙfi ÎÚËÌÓfi Î·È (Á) Ë Ù¯ÓÈ΋ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fiÌÂÓÔ˘ ÎÚËÌÓÔ‡ (Clark, 1971; Shiloah Î·È Kopezyk, 1978; Vanarsdall Î·È Corn, 1977; Hunt, 1977; Boyd, 1984; McSherry, 1998). ™‡Ìʈӷ Ì ÙÔÓ Becker (1998), ˘¿Ú¯ÂÈ ·ÎfiÌË Ì›· ̤ıÔ‰Ô˜, ÂΛÓË Ù˘ Â›Ï˘Û˘ ÙÔ˘ Û˘ÓˆÛÙÈÛÌÔ‡, ÂÊfiÛÔÓ ·˘Ùfi˜ ‹Ù·Ó Ë ·ÈÙ›· Ù˘ ·ÚÂÎÙfiÈÛ˘ ÙÔ˘ ΢Ófi‰ÔÓÙ·. DISCUSSION ∞Ï‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ∏ ·Ï‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ÂÚÈÏ·Ì‚¿ÓÂÈ ÙËÓ ÂÎÙÔÌ‹ ÙˆÓ ÈÛÙÒÓ Ô˘ ηχÙÔ˘Ó ÙË Ì‡ÏË ÙÔ˘ ¤ÁÎÏÂÈÛÙÔ˘ ‰ÔÓÙÈÔ‡. √È Fournier Î·È Û˘Ó. (1982) ÚÔÙ›ÓÔ˘Ó Ë ·ÓÙÈÌÂÙÒÈÛË ·ÚÂȷο ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ì ¢ÓÔ˚΋ ηٷÎfiÚ˘ÊË ı¤ÛË Ó· Á›ÓÂÙ·È ·Ú¯Èο Ì ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ¯ˆÚ›˜ ÂÊ·ÚÌÔÁ‹ ‰‡Ó·Ì˘ ¤Ï͢. ¶ÈÛÙÂ‡Ô˘Ó fiÙÈ Û ÈÔ Ó¤Ô˘˜ ·ÛıÂÓ›˜ ÙÔ ‰fiÓÙÈ ı· ·Ó·Ù›ÏÂÈ ÌfiÓÔ ÙÔ˘ ÌÂÙ¿ ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë, ÂÓÒ Û ÌÂÁ·Ï‡ÙÂÚ˘ ËÏÈΛ·˜ ·ÛıÂÓ›˜ ۯ‰fiÓ ¿ÓÙ· ÂӉ›ÎÓ˘Ù·È Ë ¤ÏÍË. √È Tegsjö Î·È Û˘Ó. (1984) ·Ú·Ù‹ÚËÛ·Ó fiÙÈ ÙÔ Â‡ÚÔ˜ ÙˆÓ ÎÂÚ·ÙÈ- Periodontal evaluation is an important requisite for the patient prior to combined surgical/orthodontic treatment. Periodontal problems many times can be prevented by careful case planning and appropriate oral hygiene control. Regarding the palatally impacted canines, their surgical exposure and alignment (open-surgical exposure) results to a significantly greater loss of attachment both on the buccal and palatal surfaces when compared to the control teeth, which erupted unaided (Wisth et al., 1976a; Zachrisson and Alnaes, 1974). According to Becker (1998), this method will leave the tooth with a soft tissue deficiency and a long E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 16 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment ¶›Ó·Î·˜ 1. ™‡ÁÎÚÈÛË Ù˘ ÂÚÈÔ‰ÔÓÙÈ΋˜ ηٿÛÙ·Û˘ ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ ÌÂÙ¿ ·fi ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›· (CEJ: ÔÛÙÂ˚ÓÔ-·‰·Ì·ÓÙÈÓÈ΋ ¤ÓˆÛË [√∞∂], NA: ÌË ‰È·ı¤ÛÈÌÔ, NS: ÌË ÛËÌ·ÓÙÈÎfi). Table 1. Comparisons of the periodontal status of palatally impacted canines following surgical and orthodontic treatment (CEJ: Cementoenamel junction, NA: not available, NS: non-significant). ¢fifiÓÓÙÈ· ˘fi ÂͤٷÛË Experimental teeth –x s.d. ¢fifiÓÓÙÈ· ÂϤÁ¯Ô˘ Control teeth –x s.d. ÂÁÁ‡˜/mesial ·ÚÂȷ΋/buccal ¿ˆ/distal ˘ÂÚÒÈ·/palatal ÂÁÁ‡˜/mesial ·ÚÂȷ΋/buccal ¿ˆ/distal ˘ÂÚÒÈ·/palatal 2,59 1,85 2,66 2,06 0,91 0,82 1,12 1,85 0,82 0,66 0,77 0,34 0,67 0,80 0,84 0,58 2,29 1,62 2,24 2,03 0,62 0,47 0,76 0,79 0,52 0,55 0,61 0,46 0,60 0,56 0,70 0,73 0,30 0,23 0,44 0,03 0,29 0,35 0,36 1,06 MÂÙÚÔ‡ÌÂÓÔ Â›Â‰Ô ÚfiÛÊ˘Û˘ robing attachment level ÂÁÁ‡˜/mesial ·ÚÂȷ΋/buccal ¿ˆ/distal ˘ÂÚÒÈ·/palatal 1,96 1,67 1,66 1,63 0,53 0,74 0,47 0,71 1,64 1,37 1,46 1,47 0,30 0,39 0,14 0,49 0,32 0,30 0,30 0,16 p<0,05 NS p<0,05 NS ⁄„Ô˜ ÙÔ˘ ÔÛÙÔ‡ Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜ Crestal bone height ÂÁÁ‡˜/mesial ¿ˆ/distal 0,98 1,25 0,82 0,66 0,46 1,02 0,58 0,60 0,52 0,23 p<0,01 NS E›Â‰Ô ÙÔ˘ ÔÛÙÔ‡ Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜ (·fiÛÙ·ÛË Û mm Ù˘ OAE ·fi ÙËÓ ÎÔÚ˘Ê‹ ÙÔ˘ Ê·ÙÓÈ·ÎÔ‡ ÔÛÙÔ‡) Marginal bone level distance in mm from CEJ to peak of marginal bone) ÂÁÁ‡˜/mesial ¿ˆ/distal 3,03 3,42 1,58 1,62 2,74 2,85 1,22 1,04 0,29 0,57 NS p<0,01 B¿ıÔ˜ ı˘Ï¿ÎÔ˘ Pocket depth ÂÁÁ˘˜-ÁψÛÛÈ΋/mesio-lingual ÁψÛÛÈ΋/lingual ¿ˆ ÁψÛÛÈ΋/disto-lingual ¿ˆ ¯ÂÈÏÈ΋/disto-labial ¯ÂÈÏÈ΋/labial ÂÁÁ‡˜-¯ÂÈÏÈ΋/mesio-labial 1,98 1,38 1,79 2,19 1,14 1,98 0,87 0,54 0,84 1,13 0,35 0,87 1,57 1,31 1,79 1,95 1,05 1,74 0,67 0,47 0,72 0,76 0,22 0,63 0,41 0,07 0,00 0,24 0,09 0,24 p<0,01 NS NS NS NS p<0,05 Boyd (1982) AÒÏÂÈ· ÚfiÛÊ˘Û˘ Loss of attachment ÂÁÁ˘˜-ÁψÛÛÈ΋/mesio-lingual ÁψÛÛÈ΋/lingual ¿ˆ ÁψÛÛÈ΋/disto-lingual ¿ˆ ¯ÂÈÏÈ΋/disto-labial ¯ÂÈÏÈ΋/labial ÂÁÁ‡˜-¯ÂÈÏÈ΋/mesio-labial 0,5 0,66 0,33 0,33 0,41 0,41 NA 0,33 0,5 0,5 0,41 0,33 0,33 NA 0,17 0,16 -0,17 -0,08 0,08 0,08 NA Becker et al. (1983) B¿ıÔ˜ ı˘Ï¿ÎÔ˘ Pocket depth OÛÙÈ΋ ÛÙ‹ÚÈÍË Bone support ŸÏ˜ (6) ÔÈ ÂÈÊ¿ÓÂȘ All six tooth surfaces ÂÁÁ‡˜/mesial ¿ˆ/distal 2,52 0,71 2,17 0,49 0,35 p<0,05 90,26% 88,91% 4,80 5,97 93,7% 92,87% 3,91 3,99 -3,44% -3,96% p<0,05 p<0,05 ™˘ÁÁÚ·Ê›˜ Authors MÂÙÚ‹ÛÂȘ Measurements EÈÊ¿ÓÂÈ· Surface B¿ıÔ˜ ı˘Ï¿ÎÔ˘ Pocket Depth Wisth et al. (1976a) AÒÏÂÈ· ÚfiÛÊ˘Û˘ Loss of attachment Woloshyn et al. (1994) Hansson and Rindler (1998) P-value NA NA clinical crown, especially when it is placed deeply in the palatal mucosa. Periodontal health may be also compromised when the closed-surgical exposure is performed. Woloshyn et al. (1994) observed that the probing attachment level was ÓÔÔÈËÌ¤ÓˆÓ Ô‡ÏˆÓ ÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó ÌfiÓÔ Ì ·Ï‹, ·ÏÏ¿ "ÚÈ˙È΋" ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ‹Ù·Ó ÛËÌ·ÓÙÈο ÌÂȈ̤ÓÔ Û ۯ¤ÛË Ì ÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ù˘ ¿ÏÏ˘ ÏÂ˘Ú¿˜ Ô˘ ·Ó¿ÙÂÈÏ·Ó Ê˘ÛÈÔÏÔÁÈο. ∂ÈϤÔÓ, ÙÔ ‚¿ıÔ˜ Ù˘ Ô˘ÏÔ‰ÔÓÙÈ΋˜ Û¯ÈÛÌ‹˜ E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 ¢È·ÊÔÚ¿ Difference 17 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment A B C D E F ∂ÈÎfiÓ· 3 (Û˘Ó¤¯ÂÈ· ÛÙËÓ ÂfiÌÂÓË ÛÂÏ›‰·). ∞ÓÙÈÌÂÙÒÈÛË ·ÚÂȷο ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ì ÎÏÂÈÛÙ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋. ∞. ÃÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë ÙÔ˘ ¿Óˆ ‰ÂÍÈÔ‡ ¤ÁÎÏÂÈÛÙÔ˘ ΢Ófi‰ÔÓÙ·. µ. ™˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘. C. ∂·Ó·ÙÔÔı¤ÙËÛË ÙÔ˘ ÎÚËÌÓÔ‡ Î·È Û˘ÚÚ·Ê‹, ÂÓÒ ·fi ÙÔÓ ÎÚËÌÓfi ÂͤگÂÙ·È Û˘ÚÌ¿ÙÈÓË ÚfiÛ‰ÂÛË. D. ∏ ·Ú¯È΋ ‰È‡ı˘ÓÛË Ù˘ ‰‡Ó·Ì˘ Â›Ó·È Ù¤ÙÔÈ· Ô˘ Ó· ·ÔÌ·ÎÚ‡ÓÂÈ ÙÔ ‰fiÓÙÈ ·fi Ù· ·Ú·Î›ÌÂÓ·, ÒÛÙ ·˘Ù¿ Ó· ÌËÓ ÙÚ·˘Ì·ÙÈÛÙÔ‡Ó, Î·È ÁÈ· ÙÔ ÏfiÁÔ ·˘Ùfi Ë ÔÚıÔ‰ÔÓÙÈ΋ ‰‡Ó·ÌË ÂÊ·ÚÌfi˙ÂÙ·È ÌÂ Û˘Ó‰˘·ÛÌfi ÙÌËÌ·ÙÈÎÔ‡ Û˘ÚÌ¿ÙÈÓÔ˘ ÙfiÍÔ˘ Î·È ÂÏ·ÛÙÈ΋˜ ·Ï˘Û›‰·˜. ∂. ∂Ê·ÚÌÔÁ‹ ÔÚıÔ‰ÔÓÙÈ΋˜ ‰‡Ó·Ì˘ Ì ÂÏ·ÛÙÈ΋ ·Ï˘Û›‰· Ô˘ Û˘Ó‰¤ÂÙ·È Ì ÙÔ ·Á·ÏÈÔ ÙÔ˘ ÚÔÁÔÌÊ›Ô˘. F. ¶ÂÚ·ÈÙ¤Úˆ ÂÊ·ÚÌÔÁ‹ ÔÚıÔ‰ÔÓÙÈ΋˜ ‰‡Ó·Ì˘ Ì ÂÏ·ÛÙÈ΋ ·Ï˘Û›‰· Ô˘ Û˘Ó‰¤ÂÙ·È Ì ÙÔ Û˘ÚÌ¿ÙÈÓÔ ÙfiÍÔ. Figure 3 (continued on next page). Management of labially impacted canines with the closed-flap eruption technique. A. Surgical exposure of the right upper labially impacted canine. B. Bonding of the attachment. C. Repositioning of the flap and surgical closure. A twisted ligature exits through the flap. D. The initial direction of the force should be to move the tooth away from the neighboring teeth to avoid their injury and therefore orthodontic force application is performed by means of a combination of a sectional arch wire and an elastic chain. E. Orthodontic force application by means of an elastic chain attached to the premolar bracket. F. Further orthodontic force application by means of an elastic chain attached to the archwire. E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 18 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI AP.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ increased and the crestal bone height was significantly lower in the impacted canines treated with this method. These findings agree also with the results of Becker et al. (1983), in their study group of 23 patients with unilateral palatal impaction of a maxillary canine. On the other hand, Crescini et al. (1994), found no attachment loss, no recession and no significant differences in keratinized tissue width in a follow-up examination of eight cases with impacted canines treated with this method, when compared to the contralateral unaided erupted canines. A good gingival and periodontal status with slight differences between treated and untreated sides was also reported by Hansson and Rindler (1998), in their follow-up study 1 to 18 years after completion of orthodontic treatment of unilateral palatally impacted maxillary canines; though, increased pocket depth and lower marginal bone level were registered. Caminiti et al. (1998) reported also no gingival inflammation and no recession after forced eruption of 60 palatally impacted canines treated with this technique. By comparing the open- and closed surgical exposure, it has been found that the open exposure causes more periodontal damage (loss of attachment and interdental bone height) than the closed one although the mean differences between the two techniques were small (Wisth et al., 1976b). Furthermore, Kohavi et al. (1984a) found a consistent significant loss of alveolar bone height on the mesial proximal surface of the exposed tooth with the amount of bone loss being greater if exposure is carried out to below of the cemento-enamel-junction. According to Becker (1998), the full flap closure (close-surgical exposure technique) after attachment placement on the exposed tooth must be recommended over any other, because the tooth is then exposed with the minimum tissue removal and consequent surgical trauma, which in combination with appropriate orthodontic biomechanics will provide healthy mucogingival tissues and the best bone support. Becker based scientifically his recommendation on various clinical comparisons of surgical methods of exposure (Heaney and Atherton, 1976; Wisth et al., 1976a; Odenrick and Modeer, 1978; Boyd, 1982; Becker et al., 1983; Kohavi et al., 1984a; Crescini et al., 1994; Vermette et al., 1995). By using the two-step method and direct bonding in a study group of 20 patients with one palatally impacted maxillary canine and one non-impacted, Boyd (1982) found no significant differences in the mean values of attachment loss on any of the six tooth sites between the treated canines and their contralaterals. On the contrary, the impacted canines, which were ligated with wire, showed significant loss of attachment on the proximal and lingual surfaces when compared to the non-impacted ones. These data were probably influenced by the surgical procedure used to gain access for the wire ligation placement, which was G ∂ÈÎfiÓ· 3. G. ¶ÚfiÛ‰ÂÛË ÙÔ˘ ·ÁÎ˘Ï›Ô˘ ÙÔ˘ ΢Ófi‰ÔÓÙ· ÛÙÔ ‚·ÛÈÎfi Û˘ÚÌ¿ÙÈÓÔ ÙfiÍÔ. Figure 3. G. Ligation of the canine bracket to the main archwire. ÙˆÓ ıÂÚ·Â˘Ì¤ÓˆÓ Î˘ÓÔ‰fiÓÙˆÓ ‹Ù·Ó ÛËÌ·ÓÙÈο ÌÂȈ̤ÓÔ Î·È Ë Ô˘ÏÈ΋ ˘Ê›˙ËÛË ÛËÌ·ÓÙÈο ÌÂÁ·Ï‡ÙÂÚË Û ۯ¤ÛË Ì ٷ ‰fiÓÙÈ· ÂϤÁ¯Ô˘. √ Boyd (1984) Û‡ÁÎÚÈÓ ÙËÓ "Ù¯ÓÈ΋ ÙÔ˘ ·Ú¿ı˘ÚÔ˘" (·ÔÎ¿Ï˘„Ë fiÏ˘ Ù˘ ·ÚÂȷ΋˜ ÂÈÊ¿ÓÂÈ·˜ Ù˘ ·Ó·ÙÔÌÈ΋˜ ̇Ï˘ Ì ÔÏÈ΋ ÂÎÙÔÌ‹ ÙÔ˘ ÎÂÚ·ÙÈÓÔÔÈË̤ÓÔ˘ ÈÛÙÔ‡) Ì ̛· ÈÔ Û˘ÓÙËÚËÙÈ΋ ¯ÂÈÚÔ˘ÚÁÈ΋ ÚÔÛ¤ÁÁÈÛË Ô˘ ·ÔηχÙÂÈ ÌfiÓÔ 4-5 mm ÙÔ˘ ÈÔ ÂÈÊ·ÓÂÈ·ÎÔ‡ ÙÌ‹Ì·ÙÔ˜ Ù˘ ·ÚÂȷ΋˜ fi„˘ ÙÔ˘ ʇ̷ÙÔ˜ ‰È·ÙËÚÒÓÙ·˜ 2-3 mm ÎÂÚ·ÙÈÓÔÔÈË̤ÓÔ˘ ÈÛÙÔ‡. ∞ÍÈÔÏfiÁËÛË 12 ·ÛıÂÓÒÓ ·fi οı ηÙËÁÔÚ›·, ¤ÍÈ Ì‹Ó˜ Ì ‰‡Ô ¯ÚfiÓÈ· ÌÂÙ¿ ÙËÓ ÔÚıÔ‰ÔÓÙÈ΋ ‰È¢ı¤ÙËÛË, ·ÔÎ¿Ï˘„ fiÙÈ ÔÈ ·ÛıÂÓ›˜ ÛÙÔ˘˜ ÔÔ›Ô˘˜ ¤ÁÈÓÂ Ë "Ù¯ÓÈ΋ ÙÔ˘ ·Ú¿ı˘ÚÔ˘" ·ÚÔ˘Û›·Û·Ó ÛÙ·ÙÈÛÙÈο ÌÂÁ·Ï‡ÙÂÚË Ô˘ÏÈ΋ ˘Ê›˙ËÛË, ÊÏÂÁÌÔÓ‹ ÙˆÓ Ô‡ÏˆÓ Î·È ·ÒÏÂÈ· ÚfiÛÊ˘Û˘ ÛÙËÓ ·ÚÂȷ΋ Î·È ÛÙȘ ÔÌÔÚÔ-·ÚÂȷΤ˜ ÂÈÊ¿ÓÂȘ ÙˆÓ ¤ÁÎÏÂÈÛÙˆÓ ‰ÔÓÙÈÒÓ Û ۇÁÎÚÈÛË Ì ÙÔ˘˜ ·ÛıÂÓ›˜ Ì¿ÚÙ˘Ú˜. ∆· Â˘Ú‹Ì·Ù· ·˘Ù¿ ÂȂ‚·ÈÒıËÎ·Ó Î·È ·fi ÙÔ˘˜ Kohavi Î·È Û˘Ó. (1984b), Î·È ÙÔ˘˜ Artun Î·È Û˘Ó. (1986), ÔÈ ÔÔ›ÔÈ ‚Ú‹Î·Ó ÛËÌ·ÓÙÈο ÌÈÎÚfiÙÂÚË ˙ÒÓË ÚÔÛÂÊ˘ÎfiÙˆÓ Ô‡ÏˆÓ Î·È ·ÒÏÂÈ· ÚfiÛÊ˘Û˘ ÌÂÙ¿ ÙËÓ ÔÚıÔ‰ÔÓÙÈ΋ ‰È¢ı¤ÙËÛË ¿Óˆ ΢ÓÔ‰fiÓÙˆÓ Ô˘ ·Ó¤ÙÂÈÏ·Ó ·ÚÂȷο. ∆¯ÓÈ΋ ·Ó·ÙÔÏ‹˜ Ì ÎÏÂÈÛÙfi ÎÚËÌÓfi ™ÙËÓ Ù¯ÓÈ΋ ·˘Ù‹ Á›ÓÂÙ·È ·Ó‡„ˆÛË ÎÚËÌÓÔ‡, Û˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘ ÛÙÔ ¤ÁÎÏÂÈÛÙÔ ‰fiÓÙÈ Î·È Â·Ó·Û˘ÚÚ·Ê‹ ÙÔ˘ ÎÚËÌÓÔ‡ ÛÙËÓ ·Ú¯È΋ ÙÔ˘ ı¤ÛË (∂ÈÎ. 3) (Gaulis Î·È Joho, 1978; Kokich Î·È Mathews, 1993). √È Vermette Î·È Û˘Ó. (1995) ·Ú·Ù‹ÚËÛ·Ó fiÙÈ ÙÔ Â‡ÚÔ˜ ÙˆÓ ÚÔÛÂÊ˘ÎfiÙˆÓ Ô‡ÏˆÓ ÛÙÔ˘˜ ·ÚÂȷο ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ÙËÓ Ù¯ÓÈ΋ ·Ó·ÙÔÏ‹˜ Ì ÎÏÂÈÛÙfi ÎÚËÌÓfi ‹Ù·Ó ÌÂȈ̤ÓÔ ÛÙËÓ E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 AR.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment 19 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ considerably more extensive and often involved exposure of the entire crown and a small part of the root in the area of the cemento-enamel junction. As far as the treatment of labially impacted canines concerned, it was found that, when compared to nonimpacted contralateral ones, their simple surgical exposure resulted to damaging effects on the periodontium (Tegsjö et al., 1984; Boyd, 1984). Regarding the closed-eruption technique, it was observed that a reduced width of attached gingiva and an increased probing bone level of the uncovered teeth (Vermette et al., 1995), while there have been also contradictory results (Crescini et al., 1994). Furthermore, regarding the apically positioned flap procedure, Vermette et al. (1995) reported significant damaging effects on the periodontium, although Tegsjö et al. (1994) found no significant differences on the periodontal status between impacted canines treated with this method and the non-treated controls. Finally, the comparison of the closed-eruption technique with the apically repositioned flap technique, Vermette et al. (1995) revealed that teeth uncovered with the apically repositioned flap technique presented more un-esthetic sequelae than those uncovered with the closed-eruption technique (Vermette et al. 1995). ¿ˆ ÂÈÊ¿ÓÂÈ· Î·È ÙÔ ÔÛÙfi Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜ ‚ÚÈÛÎfiÙ·Ó ÂÚÈÛÛfiÙÂÚÔ ·ÎÚÔÚÚÈ˙Èο ÛÙËÓ ·ÚÂȷ΋ ÙÔ˘˜ ÂÈÊ¿ÓÂÈ· Û ۯ¤ÛË Ì ٷ ‰fiÓÙÈ· ÂϤÁ¯Ô˘. √È Crescini Î·È Û˘Ó. (1994) ·Ó·Ê¤ÚÔÓÙ·È ÛÙȘ ÂÚÈÔ‰ÔÓÙÈΤ˜ ÂȉڿÛÂȘ Ù˘ ÎÏÂÈÛÙ‹˜ ¯ÂÈÚÔ˘ÚÁÈ΋˜ Ù¯ÓÈ΋˜ Ì ¤ÏÍË ‰È·Ì¤ÛÔ˘ ÙÔ‡ÓÂÏ ÁÈ· ·ÚÂȷο ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ô˘ ‚Ú›ÛÎÔÓÙ·È Û ÌÂÁ¿ÏÔ ‚¿ıÔ˜. ¢ÂÓ ‚Ú‹Î·Ó ·ÒÏÂÈ· ÚfiÛÊ˘Û˘ Î·È ˘Ê›˙ËÛË ÛÙÔ Ù¤ÏÔ˜ Ù˘ ÂÓÂÚÁÔ‡ ıÂڷ›·˜ Î·È ÌÂÙ¿ ·fi ÂÚ›Ô‰Ô ·Ú·ÎÔÏÔ‡ıËÛ˘ ÙÚÈÒÓ ¯ÚfiÓˆÓ. ∂ÈϤÔÓ, ‰ÂÓ ·Ú·ÙËÚ‹ıËÎ·Ó ÛËÌ·ÓÙÈΤ˜ ‰È·ÊÔÚ¤˜ ÛÙÔ Â‡ÚÔ˜ ÙˆÓ ÎÂÚ·ÙÈÓÔÔÈËÌ¤ÓˆÓ Ô‡ÏˆÓ ÌÂٷ͇ ÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÔηχÊıËÎ·Ó ¯ÂÈÚÔ˘ÚÁÈο Î·È ÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ù˘ ¿ÏÏ˘ ÏÂ˘Ú¿˜ Ô˘ ·Ó¿ÙÂÈÏ·Ó ·˘ÙfiÌ·Ù·. ∆¯ÓÈ΋ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fi fiÌÌÂÓÔ˘ ÎÚËÌÓÔ‡ ™‡Ìʈӷ Ì ÙËÓ Ù¯ÓÈ΋ ·˘Ù‹, Á›ÓÂÙ·È ·Ó‡„ˆÛË ÎÚËÌÓÔ‡ ÌÂÚÈÎÔ‡ ¿¯Ô˘˜ Î·È ÚÔÛÂÎÙÈ΋ ·fiÍÂÛË ÙÔ˘ ÙÚ·‡Ì·ÙÔ˜ ¤ÙÛÈ ÒÛÙ ӷ ·Ê·ÈÚÂı› Ô Ô‰ÔÓÙÈÎfi˜ Û¿ÎÔ˜ Î·È Ó· ·ÔÎ·Ï˘Êı› ÙÔ ‰fiÓÙÈ. ¢ÂÓ ··ÈÙÂ›Ù·È ·Ê·›ÚÂÛË ÔÛÙÔ‡, ÂÎÙfi˜ Î·È ·Ó ·˘Ùfi Â›Ó·È ··Ú·›ÙËÙÔ ÁÈ· Ó· ÚÔÛÂÁÁÈÛÙ› Ë Ì‡ÏË ÙÔ˘ ΢Ófi‰ÔÓÙ·. ∏ ÚÔۤϷÛË Ù˘ ̇Ï˘ Ú¤ÂÈ Ó· ÂÎÙÂÏÂÛÙ› fiÛÔ ÈÔ Û˘ÓÙËÚËÙÈο Á›ÓÂÙ·È Î·È fi¯È ¤Ú·Ó Ù˘ ÔÛÙÂ˚ÓÔ-·‰·Ì·ÓÙÈÓÈ΋˜ ¤ÓˆÛ˘. √ ÎÚËÌÓfi˜ Â·Ó·Û˘ÚÚ¿ÙÂÙ·È ·ÎÚÔÚÚÈ˙Èο Ì ‰È·ÎÂÎÔÌ̤ӷ ÂÚÈÔÛÙÈο Ú¿ÌÌ·Ù· Î·È ÙÔÔıÂÙÂ›Ù·È ÛÙËÓ ÂÚÈÔ¯‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ÎÔÓ›· ÁÈ· 7-10 ̤Ú˜ (Theofanatos Î·È Û˘Ó., 1994). ™‡Ìʈӷ Ì ÙÔÓ Becker (1998), Ë ·Ó·ÙÔÏ‹ ÙÔ˘ ‰ÔÓÙÈÔ‡ ÂÈÙ·¯‡ÓÂÙ·È Ì ÙËÓ Ù¯ÓÈ΋ ·˘Ù‹. ∏ ̤ıÔ‰Ô˜ ·˘Ù‹ ‰ÂÓ Û˘ÓÈÛÙ¿Ù·È Û ÂÚ›ÙˆÛË Ô˘ ÙÔ ¤ÁÎÏÂÈÛÙÔ ‰fiÓÙÈ ‚Ú›ÛÎÂÙ·È Ôχ „ËÏ¿, ÂÊfiÛÔÓ Ô ·ÎÚÔÚÚÈ˙Èο ·ӷÙÔÔıÂÙÔ‡ÌÂÓÔ˜ ÎÚËÌÓfi˜ ı· ·Ê‹ÛÂÈ Â˘Ú›· ÂÚÈÔ¯‹ ÙÔ˘ ·ÚÂÈ·ÎÔ‡ ÔÛÙÈÎÔ‡ ÂÙ¿ÏÔ˘ ÂÎÙÂıÂÈ̤ÓË ÛÙÔ ÛÙÔÌ·ÙÈÎfi ÂÚÈ‚¿ÏÏÔÓ ¯ˆÚ›˜ ÏfiÁÔ. ∂Ó ÙÔ‡ÙÔȘ, ÛËÌ·ÓÙÈÎfi ÏÂÔÓ¤ÎÙËÌ· Ù˘ ÌÂıfi‰Ô˘ ·ÔÙÂÏ› ÙÔ ÁÂÁÔÓfi˜ fiÙÈ Ô ·ÚÂȷο ¤ÁÎÏÂÈÛÙÔ˜ ΢Ófi‰ÔÓÙ·˜ ·Ú·Ì¤ÓÂÈ ÚÔÛÂÏ¿ÛÈÌÔ˜ ÁÈ· Û˘ÁÎfiÏÏËÛË ÔÚıÔ‰ÔÓÙÈÎÔ‡ Û˘Ó‰¤ÛÌÔ˘ Û ‰Â‡ÙÂÚÔ ¯ÚfiÓÔ, ÂÊfiÛÔÓ Ô ÔÚıÔ‰ÔÓÙÈÎfi˜ ·ÔÊ·Û›ÛÂÈ Ó· οÓÂÈ ÂÓÂÚÁfi ˘ÂÚ¤ÎÊ˘ÛË ÙÔ˘ ‰ÔÓÙÈÔ‡. ™¯ÂÙÈο Ì ÙËÓ ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË ÌÂÙ¿ ·fi ÂÊ·ÚÌÔÁ‹ Ù˘ Ù¯ÓÈ΋˜ ·˘Ù‹˜, ÔÈ Vermette Î·È Û˘Ó. (1995) ‚Ú‹Î·Ó fiÙÈ ÙÔ Ô˘ÏÈÎfi fiÚÈÔ ·ÚÂȷο ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ·˘Ù‹ ÙË Ì¤ıÔ‰Ô ‚ÚÈÛÎfiÙ·Ó ·ÎÚÔÚÚÈ˙ÈÎfiÙÂÚ· ÛÙËÓ ÂÁÁ‡˜ Î·È ·ÚÂȷ΋ ÂÈÊ¿ÓÂÈ·, Î·È ˘‹Ú¯Â ÌÂÁ·Ï‡ÙÂÚË ÔÛÙÈ΋ ·ÒÏÂÈ· ÛÙȘ fiÌÔÚ˜ Î·È ÛÙËÓ ·ÚÂȷ΋ ÂÈÊ¿ÓÂÈ· Û ۯ¤ÛË Ì ٷ ‰fiÓÙÈ· ÂϤÁ¯Ô˘. ∞ÓÙ›ıÂÙ· ÔÈ Tegsjö Î·È Û˘Ó. (1984) ‰ÂÓ ·Ú·Ù‹ÚËÛ·Ó ÛËÌ·ÓÙÈΤ˜ ‰È·ÊÔÚ¤˜ ÛÙËÓ ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË ÌÂٷ͇ ıÂÚ·Â˘Ì¤ÓˆÓ Î·È ÌË ‰ÔÓÙÈÒÓ (¶›Ó·Î·˜ 2). E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment CONCLUSIONS Purpose of orthodontic treatment should not only be to correct a malocclusion but to correct it with minimal side effects to the teeth and their supporting tissues. When alternative treatment procedures are discussed, it is important to be able to select that kind of treatment which causes the least damage. Although the opinions of the researchers are at some degree controversial, it can be concluded that, both palatally and labially impacted canines are almost always affected, not-depending from the surgical or orthodontic procedures used. However, it seems that less periodontal affection should anticipated when orthodontic forces are applied after performing closedsurgical exposure techniques, which involve raising of a surgical flap, bonding of an attachment and finally resuturing of the flap to its original position. REFERENCES Artun J, Osterberg SK, Joondeph DR. Long-term periodontal status of labially erupted canines following orthodontic treatment. J Clin Periodontol 1986;13:856-61. Azaz B, Steiman Z, Koyoumdjisky-Kaye E, LewinEpstein J. The sequelae of surgical exposure of 20 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment ¶›Ó·Î·˜ 2. ™‡ÁÎÚÈÛË Ù˘ ÂÚÈÔ‰ÔÓÙÈ΋˜ ηٿÛÙ·Û˘ ·ÚÂȷο ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ ÌÂÙ¿ ·fi ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›· (CEJ: ÔÛÙÂ˚ÓÔ-·‰·Ì·ÓÙÈÓÈ΋ ¤ÓˆÛË [√∞∂], NS: ÌË ÛËÌ·ÓÙÈÎfi). Table 2. Comparisons of the periodontal status of labially impacted canines following surgical and orthodontic treatment (CEJ: Cementoenamel junction, NS: non-significant). T¯ÓÈ΋ ·Ó·ÙÔÏ‹˜ Ì ÎÏÂÈÛÙfi ÎÚËÌÓfi Closed eruption technique ™˘ÁÁÚ·Ê›˜ Authors Vermette et al. (1995) MÂÙÚ‹ÛÂȘ Measurements EÈÊ¿ÓÂÈ· Surface ¢fifiÓÓÙÈ· ˘fi ÂͤٷÛË Experimental teeth –x s.d. ¢fifiÓÓÙÈ· ÂϤÁ¯Ô˘ P-value Control teeth –x s.d. ¢fifiÓÓÙÈ· ˘fi ÂͤٷÛË Experimental teeth –x s.d. ¢fifiÓÓÙÈ· ÂϤÁ¯Ô˘ Control teeth –x s.d. P-value E‡ÚÔ˜ ÚÔÛÂÊ˘ÎfiÙˆÓ ÂÁÁ‡˜/mesial Ô‡ÏˆÓ ÚfiÛıÈ·/facial Width of attached ¿ˆ/distal gingiva 4,3 2,2 3,5 2,14 0,89 1,49 4,6 2,0 4,2 1,48 NS 1,18 NS 1,33 p<0,05 5,6 3,5 3,9 2,78 2,08 2,08 4,7 1,9 3,8 1,48 0,68 1,60 NS p<0,01 NS O˘ÏÈÎfi fiÚÈÔ Gingival margin ÂÁÁ‡˜/mesial ÚfiÛıÈ·/facial ¿ˆ/distal 2,3 0,9 2,3 0,78 1,12 0,63 2,3 1,3 2,4 0,62 0,75 0,63 2,1 0,6 2,3 0,67 1,04 0,69 2,4 1,3 2,4 0,61 0,69 0,62 p<0,00 1 p<0,00 NS MÂÙÚÔ‡ÌÂÓÔ Â›Â‰Ô ÙÔ˘ Ê·ÙÓ·ÈÎÔ‡ ÔÛÙÔ‡ Probing bone level ÂÁÁ‡˜/mesial ÚfiÛıÈ·/facial ¿ˆ/distal 1,7 2,1 1,8 0,49 0,79 0,45 1,8 1,6 1,6 0,45 NS 0,51 p<0,05 0,51 NS 2,3 2,4 2,2 0,57 0,98 0,62 1,8 1,6 1,7 0,71 0,61 0,57 p<0,01 p<0,01 p<0,01 NS NS NS AÏ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë Simple surgical exposure technique E‡ÚÔ˜ ÚÔÛÂÊ˘ÎfiÙˆÓ Ô‡ÏˆÓ Width of attached gingiva Tegsjö et al. (1984) T¯ÓÈ΋ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fifiÌÌÂÓÔ˘ ÎÚËÌÓÔ‡ Apically positioned flap technique ¯ÂÈÏÈ΋/labial B¿ıÔ˜ Ô˘ÏÔ‰ÔÓÙÈ΋˜ ¯ÂÈÏÈ΋/labial ÂÁÁ‡˜/mesial Û¯ÈÛÌ‹˜ ˘ÂÚÒÈ·/palatal Sulcus depth ¿ˆ/distal AfiÛÙ·ÛË Û mm Ù˘ OAE ·fi ÙÔ Ô˘ÏÈÎfi fiÚÈÔ Distance in mm from CEJ to gingival margin ¯ÂÈÏÈ΋/labial 2,6 1,4 4,1 1,5 p<0,01 4,3 1,8 3,9 1,5 NS 1,2 2,4 2,1 2,6 0,4 0,6 0,5 0,6 1,6 1,9 1,9 2,0 0,6 0,6 0,5 p<0,01 0,6 1,4 2,1 2,0 2,2 0,4 0,5 0,5 0,6 1,6 2,2 2,0 2,1 0,4 0,7 0,5 0,6 NS -0,5 1,0 -1,5 0,8 p<0,01 -0,9 1,2 -1,1 0,9 NS unerupted teeth. J Oral Surg 1980;38:121-7. Becker A, Bimstein E, Shteyer A. Interdisciplinary treatment of multiple unerupted supernumerary teeth. Am J Orthod 1982;81:417-22. Becker A, Kohavi D, Zilberman Y. Periodontal status following the alignement of palatally impacted canine teeth. Am J Orthod 1983;84:332-6. Becker A, Shpack N, Shteyer A. Attachment bonding to impacted teeth at the time of surgical exposure. Eur J Orthod 1996;18:457-63. ™YZHTH™H ∏ ÂÚÈÔ‰ÔÓÙÈ΋ ·ÍÈÔÏfiÁËÛË Â›Ó·È ÛËÌ·ÓÙÈ΋ ÁÈ· ÙÔÓ ·ÛıÂÓ‹ ÚÈÓ ·fi Û˘Ó‰˘·Ṳ̂ÓË ¯ÂÈÚÔ˘ÚÁÈ΋/ÔÚıÔ‰ÔÓÙÈ΋ ıÂڷ›·. ∆· ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· ÌÔÚ› ÔÏϤ˜ ÊÔÚ¤˜ Ó· ÚÔ‚ÏÂÊıÔ‡Ó Ì ÚÔÛÂÎÙÈÎfi ۯ‰ȷÛÌfi ÙÔ˘ ÂÚÈÛÙ·ÙÈÎÔ‡ Î·È Î·Ù¿ÏÏËÏÔ ¤ÏÂÁ¯Ô Ù˘ ÛÙÔÌ·ÙÈ΋˜ ˘ÁÈÂÈÓ‹˜. ™¯ÂÙÈο Ì ÙÔ˘˜ ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜, Ë ¯ÂÈE§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 T¯ÓÈ΋ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fifiÌÌÂÓÔ˘ ÎÚËÌÓÔ‡ Apically positioned flap technique 21 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ Becker A. The orthodontic treatment of impacted teeth. London: M Dunitz Ltd, 1998. Bishara S. Impacted maxillary canines: A review. Am J Orthod Dentofac Orthop 1992;101:159-71. Boyd RL. Clinical assessment of injuries in orthodontic movement of impacted teeth. I. Methods of attachment. Am J Orthod 1982;82:478-86. Boyd RL. Clinical assessment of injuries in orthodontic movement of impacted teeth. II. Surgical recommendations. Am J Orthod 1984;86:407-18. Caminiti MF, Sander GKB, Giambattistini C, Tompson B. Outcomes of the surgical exposure, bonding and eruption of 82 impacted maxillary canines. J Can Dent Assoc 1998;64:572-4, 576-9. Clark D. The management of impacted canines: free physiologic eruption. J Am Dent Assoc 1971;82:836-40. Crescini A, Clauser C, Giorgetti R, Cortellini P, Pini Prato GP. Tunnel traction of infraosseous impacted maxillary canines: a three-year periodontal followup. Am J Orthod Dentofacial Orthop 1994;105:61-72. Dachi SF, Howell FV. A survey of 3874 routine full-mouth radiographs. II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol 1961;14:1165-9. Elefteriadis JN, Athanasiou AE. Evaluation of impacted canines by means of computerised tomography. Int J Adult Orthod Orthognath Surg 1996;11:257-64. Fournier A, Turcotte JY, Bernard C. Orthodontic considerations in the treatment of maxillary impacted canines. Am J Orthod 1982; 81: 236-9 Gaulis R, Joho JP. Parodonte marginal de canines superieures incluses: Evaluation suite a differentes methodes d’ acces chirurgical et de systeme orthodontique. [The marginal periodontium of impacted upper canines. Evaluation following various methods of surgical approach and orthodontic procedures.] SSO Schweiz Monatsschr Zahnheilkd. 1978;88:1249-61. Hansson C, Rindler A. Periodontal conditions following surgical and orthodontic treatment of palatally impacted maxillary canines-a follow-up study. Angle Orthod 1998;68:167-72. Heaney TG, Atherton JD. Periodontal problems associated with the surgical exposure of unerupted teeth. Br J Orthod 1976;3:79-84. Heasman PA, Millett DT, Chapple IL. The periodontium and orthodontics in health and disease. Oxford: Oxford University Press, 1996. Hunt NP. Direct traction applied to unerupted teeth using the acid-etch technique. Br J Orthod 1977;4:211-2. Jacoby H. The etiology of maxillary canine impactions. Am J Orthod 1983;84:125-32. Kohavi D, Becker A, Zilberman Y. Surgical exposure, orthodontic movement , and final tooth position as ÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„Ë Î·È ‰È¢ı¤ÙËÛ‹ ÙÔ˘˜ (·ÓÔȯً ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋) ¤¯ÂÈ ˆ˜ ·ÔÙ¤ÏÂÛÌ· ÛËÌ·ÓÙÈο ÌÂÁ·Ï‡ÙÂÚË ·ÒÏÂÈ· ÚfiÛÊ˘Û˘ ÛÙËÓ ·ÚÂȷ΋ Î·È ˘ÂÚÒÈ· ÂÈÊ¿ÓÂÈ· Û˘ÁÎÚÈÙÈο Ì ٷ ‰fiÓÙÈ· ÂϤÁ¯Ô˘ Ô˘ ·Ó·Ù¤ÏÏÔ˘Ó ¯ˆÚ›˜ ˘Ô‚Ô‹ıËÛË (Wisth Î·È Û˘Ó., 1976a; Zachrisson Î·È Alnaes, 1974). ™‡Ìʈӷ Ì ÙÔÓ Becker (1998), Ë Ì¤ıÔ‰Ô˜ ·˘Ù‹ ‰ËÌÈÔ˘ÚÁ› ÛÙÔ ‰fiÓÙÈ ¤ÏÏÂÈÌÌ· Ì·Ï·ÎÒÓ ÈÛÙÒÓ Î·È ÌÂÁ¿ÏË ÎÏÈÓÈ΋ ̇ÏË, ȉȷ›ÙÂÚ· fiÙ·Ó ÙÔ ‰fiÓÙÈ ‚Ú›ÛÎÂÙ·È Û ÌÂÁ¿ÏÔ ‚¿ıÔ˜ ÛÙÔÓ ˘ÂÚÒÈÔ ‚ÏÂÓÓÔÁfiÓÔ. ¶ÂÚÈÔ‰ÔÓÙÈΤ˜ Û˘Ó¤ÂȘ ÌÔÚ› Ó· ˘¿ÚÍÔ˘Ó Î·È Ì ÙËÓ ÎÏÂÈÛÙ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋. √È Woloshyn Î·È Û˘Ó. (1994) ·Ú·Ù‹ÚËÛ·Ó ·‡ÍËÛË ÙÔ˘ ÌÂÙÚÔ‡ÌÂÓÔ˘ ÂȤ‰Ô˘ ÚfiÛÊ˘Û˘, ÂÓÒ ÙÔ ‡„Ô˜ ÙÔ˘ ÔÛÙÔ‡ Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜ ‹Ù·Ó ÛËÌ·ÓÙÈο ÌÂȈ̤ÓÔ ÛÙÔ˘˜ ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ·˘Ù‹ ÙË Ì¤ıÔ‰Ô. ∆· Â˘Ú‹Ì·Ù· ·˘Ù¿ Û˘ÌʈÓÔ‡Ó Ì ٷ ·ÔÙÂϤÛÌ·Ù· ÙˆÓ Becker Î·È Û˘Ó. (1983), ÔÈ ÔÔ›ÔÈ ÌÂϤÙËÛ·Ó 23 ·ÛıÂÓ›˜ Ì ÂÙÂÚfiÏ¢ÚË ·ÚÂȷ΋ ¤ÁÎÏÂÈÛË ¿Óˆ ΢Ófi‰ÔÓÙ·. ∞fi ÙËÓ ¿ÏÏË ÏÂ˘Ú¿, ÔÈ Crescini Î·È Û˘Ó. (1994) ‰ÂÓ ‚Ú‹Î·Ó ·ÒÏÂÈ· ÚfiÛÊ˘Û˘, ˘Ê›˙ËÛË ‹ ÛËÌ·ÓÙÈΤ˜ ‰È·ÊÔÚ¤˜ ÛÙÔ Â‡ÚÔ˜ ÙÔ˘ ÎÂÚ·ÙÈÓÔÔÈË̤ÓÔ˘ ÈÛÙÔ‡ ηٿ ÙËÓ ·Ú·ÎÔÏÔ‡ıËÛË ÔÎÙÒ ÂÚÈÙÒÛÂˆÓ ÂÁÎÏ›ÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ÙËÓ Ù¯ÓÈ΋ ·˘Ù‹ Û ۇÁÎÚÈÛË Ì ÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ ÂϤÁ¯Ô˘ Ù˘ ¿ÏÏ˘ ÏÂ˘Ú¿˜ Ô˘ ·Ó¤ÙÂÈÏ·Ó ¯ˆÚ›˜ ˘Ô‚Ô‹ıËÛË. ∫·Ï‹ Ô˘ÏÈ΋ Î·È ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË Ì ÌÈÎÚ¤˜ ‰È·ÊÔÚ¤˜ ÌÂٷ͇ ¯ÂÈÚÔ˘ÚÁËÌ¤ÓˆÓ Î·È ÌË Ï¢ÚÒÓ ·Ó·Ê¤ÚÔ˘Ó Î·È ÔÈ Hansson Î·È Rindler (1998) Û ÌÂϤÙË ·Ú·ÎÔÏÔ‡ıËÛ˘ 1 ¤ˆ˜ 18 ¯ÚfiÓÈ· ÌÂÙ¿ ÙÔ Ù¤ÏÔ˜ Ù˘ ÔÚıÔ‰ÔÓÙÈ΋˜ ıÂڷ›·˜ ÂÙÂÚfiÏÂ˘ÚˆÓ ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙˆÓ ¿Óˆ ΢ÓÔ‰fiÓÙˆÓ, ·ÚfiÏÔ Ô˘ ηٷÁÚ¿ÊËΠ·˘ÍË̤ÓÔ ‚¿ıÔ˜ ı˘Ï¿ÎÔ˘ Î·È ¯·ÌËÏfiÙÂÚÔ Â›Â‰Ô ÔÛÙÔ‡ Ù˘ Ê·ÙÓȷ΋˜ ·ÎÚÔÏÔÊ›·˜. √È Caminiti Î·È Û˘Ó. (1998) ·Ó·Ê¤ÚÔ˘Ó ·Ô˘Û›· ÊÏÂÁÌÔÓ‹˜ ÙˆÓ Ô‡ÏˆÓ Î·È ˘Ê›˙ËÛ˘ ÌÂÙ¿ ·fi ˘Ô‚ÔËıÔ‡ÌÂÓË ·Ó·ÙÔÏ‹ 60 ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ÙËÓ ÎÏÂÈÛÙ‹ Ù¯ÓÈ΋. ™˘ÁÎÚ›ÓÔÓÙ·˜ ÙËÓ ·ÓÔȯً Î·È ÎÏÂÈÛÙ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋ ·ÔÎ¿Ï˘„˘ ÙˆÓ ¤ÁÎÏÂÈÛÙˆÓ ‰ÔÓÙÈÒÓ, ‚Ú¤ıËΠfiÙÈ Ë ·ÓÔȯً Ù¯ÓÈ΋ ÚÔηÏ› ÌÂÁ·Ï‡ÙÂÚË ÂÚÈÔ‰ÔÓÙÈ΋ ηٷÛÙÚÔÊ‹ (·ÒÏÂÈ· ÚfiÛÊ˘Û˘ Î·È ‡„Ô˘˜ ÌÂÛÔ‰fiÓÙÈÔ˘ ÔÛÙÔ‡) ·fi ÙËÓ ÎÏÂÈÛÙ‹ ̤ıÔ‰Ô, ·ÚfiÏÔ Ô˘ ÔÈ Ì¤Û˜ ‰È·ÊÔÚ¤˜ ÌÂٷ͇ ÙÔ˘˜ ‹Ù·Ó ÌÈÎÚ¤˜ (Wisth Î·È Û˘Ó., 1976b). ∂ÈϤÔÓ, ÔÈ Kohavi Î·È Û˘Ó. (1984a) ·ÓÂÈÏËÌ̤ӈ˜ ‚Ú‹Î·Ó ÛËÌ·ÓÙÈ΋ ·ÒÏÂÈ· ‡„Ô˘˜ Ê·ÙÓÈ·ÎÔ‡ ÔÛÙÔ‡ ÛÙËÓ ÂÁÁ‡˜ fiÌÔÚË ÂÈÊ¿ÓÂÈ· ÙÔ˘ ·ÔÎ·Ï˘Ì̤ÓÔ˘ ‰ÔÓÙÈÔ‡. ∏ ÔÛÙÈ΋, ‰Â, ·ÒÏÂÈ· ‹Ù·Ó ÌÂÁ·Ï‡ÙÂÚË fiÙ·Ó Ë ·Ê·›ÚÂÛË ÈÛÙÒÓ ÁÈ· ·ÔÎ¿Ï˘„Ë ÙÔ˘ ‰ÔÓÙÈÔ‡ ÂÎÙÂÈÓfiÙ·Ó ¤Ú·Ó Ù˘ ÔÛÙÂ˚ÓÔ-·‰·Ì·ÓÙÈÓÈ΋˜ ¤ÓˆÛ˘. ™‡Ìʈӷ Ì ÙÔÓ Becker (1998), Ë ÎÏÂÈÛÙ‹ ¯ÂÈÚÔ˘ÚÁÈ΋ Ù¯ÓÈ΋ ıˆE§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment 22 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ factors in periodontal breakdown of treated palatally impacted canines. Am J Orthod 1984a;85:72-7. Kohavi D, Zilberman Y, Becker A. Periodontal status following the alignment of bucally ectopic maxillary canine teeth. Am J Orthod 1984b;85:78-82. Kokich VG, Mathews DP. Surgical and orthodontic management of impacted teeth. Dent Clin North Am 1993;37:181-204. Lappin MM. Practical management of the impacted maxillary canine. Am J Orthod 1951;37:769-78. Lewis PD. Preorthodontic surgery in the treatment of impacted canines. Am J Orthod 1971;60:383-97. Maloney FM. The palatally impacted cuspid tooth: a new surgical approach to treatment. Aust Dent J 1985;30:37-46. McSherry PF. The assessment of and treatment options for the buried maxillary canine. Dental Update 1996;23:7-10 McSherry PF. The ectopic canine: A Review. Br J Orthod 1998;25:209-16. Odenrick L, Modeer T. Periodontal status following surgical-orthodontic alignment of impacted teeth. Acta Odontol Scand 1978;36:233-6. Papadopoulos MA, Ioannidou-Marathiotou I, Gianniou E, Kolokithas G. Impacted teeth in a Greek malocclusion population. Hell Orthod Rev 2001;4:103-17. Pearson MH, Robinson SN, Reed R, Birnie DJ, Zaki GA. Management of palatally impacted canines: the findings of a collaborative study. Eur J Orthod 1997;19:511-5. Sayne S, Lennartson B, Thilander B. Transalveolar transplantation of maxillary canines. Am J Orthod Dentofac Orthop 1986;90:149-57. Shapira Y, Kuftinec M. Treatment of impacted cuspids the hazard lasso. Angle Orthod 1981;51:203-7. Shaw B, Schneider SS, Zeyer J. Surgical management of ankylosed impacted maxillary canines. J Am Dent Assoc 1981;102:497-500. Shiloah J, Kopezyk RA. Mucogingival considerations in surgical exposure of maxillary impacted canines: report of a case. J Dent Child 1978;45:79-81. Tegsjö U, Valerius-Olsson H, Anderson L. Periodontal conditions following surgical exposure of unerupted maxillary canines-a long term follow-up study of two surgical techniques. Swed Dent J 1984;8:257-63. Theofanatos GD, Zavras AI, Turner IM. Periodontal considerations in the treatment of maxillary impacted cuspids. J Clin Ped Dent 1994;18:24552. Vanarsdall RL, Corn H. Soft tissue management of labially positioned unerupted teeth. Am J Orthod 1977;72:53-64. Vermette ME, Kokich VG, Kennedy DB. Uncovering labially impacted teeth: apically positioned flap and ÚÂ›Ù·È Ë Î·Ï‡ÙÂÚË ‰ÈfiÙÈ ÙÔ ‰fiÓÙÈ ·ÔηχÙÂÙ·È Ì ÙËÓ ÂÏ¿¯ÈÛÙË ‰˘Ó·Ù‹ ·Ê·›ÚÂÛË ÈÛÙÒÓ Î·È, ηٿ Û˘Ó¤ÂÈ·, Ì ÂÏ¿¯ÈÛÙÔ ¯ÂÈÚÔ˘ÚÁÈÎfi ÙÚ·‡Ì·, ÁÂÁÔÓfi˜ ÙÔ ÔÔ›Ô ÛÂ Û˘Ó‰˘·ÛÌfi Ì ٷ ηٿÏÏËÏ· ÔÚıÔ‰ÔÓÙÈο ÂÌ‚ÈÔÌ˯·ÓÈο Û˘ÛÙ‹Ì·Ù· ·Ú¤¯ÂÈ ˘ÁÈ›˜ Ô˘ÏÔ‚ÏÂÓÓÔÁfiÓÈÔ˘˜ ÈÛÙÔ‡˜ Î·È ÙËÓ Î·Ï‡ÙÂÚË ‰˘Ó·Ù‹ ÔÛÙÈ΋ ÛÙ‹ÚÈÍË. ∏ ÂÈÛÙËÌÔÓÈ΋ ‚¿ÛË Ù˘ ¿Ô„˘ ÙÔ˘ Becker ¤ÁÎÂÈÙ·È ÛÙËÓ ÎÏÈÓÈ΋ Û‡ÁÎÚÈÛË ‰È·ÊfiÚˆÓ ÌÂıfi‰ˆÓ ¯ÂÈÚÔ˘ÚÁÈ΋˜ ·ÔÎ¿Ï˘„˘ (Heaney Î·È Atherton, 1976; Wisth Î·È Û˘Ó., 1976a; Odenrick Î·È Modeer, 1978; Boyd, 1982; Becker Î·È Û˘Ó., 1983; Kohavi Î·È Û˘Ó., 1984a; Crescini Î·È Û˘Ó., 1994; Vermette Î·È Û˘Ó., 1995). √ Boyd (1982), ¯ÚËÛÈÌÔÔÈÒÓÙ·˜ Ù¯ÓÈ΋ ‰‡Ô ÛÙ·‰›ˆÓ Î·È ¿ÌÂÛË Û˘ÁÎfiÏÏËÛË Û ÔÌ¿‰· ÌÂϤÙ˘ 20 ·ÛıÂÓÒÓ Ì ¤Ó·Ó ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙÔ ¿Óˆ ΢Ófi‰ÔÓÙ· Î·È ¤Ó·Ó ÌË ¤ÁÎÏÂÈÛÙÔ, ‰ÂÓ ‚ڋΠÛËÌ·ÓÙÈΤ˜ ‰È·ÊÔÚ¤˜ ÛÙȘ ̤Û˜ ÙÈ̤˜ Ù˘ ·ÒÏÂÈ·˜ ÚfiÛÊ˘Û˘ Û ηӤӷ ·fi Ù· ¤ÍÈ ÛËÌ›· οı ‰ÔÓÙÈÔ‡ fiÔ˘ ¤ÁÈÓ·Ó ÌÂÙÚ‹ÛÂȘ ÌÂٷ͇ ıÂÚ·Â˘Ì¤ÓˆÓ Î·È ÌË Î˘ÓÔ‰fiÓÙˆÓ. ∞ÓÙ›ıÂÙ·, ÛÙÔ˘˜ ¤ÁÎÏÂÈÛÙÔ˘˜ ΢Ófi‰ÔÓÙ˜ fiÔ˘ ¤ÁÈÓ ÚfiÛ‰ÂÛË Ì ۇÚÌ·, ‚Ú¤ıËΠÛËÌ·ÓÙÈ΋ ·ÒÏÂÈ· ÚfiÛÊ˘Û˘ ÛÙȘ fiÌÔÚ˜ Î·È ÙËÓ ÁψÛÛÈ΋ ÂÈÊ¿ÓÂÈ· Û ۯ¤ÛË Ì ٷ ÌË ¤ÁÎÏÂÈÛÙ· ‰fiÓÙÈ·. ∆· ‰Â‰Ô̤ӷ ·˘Ù¿ Èı·ÓÒ˜ ÂËÚ¿ÛÙËÎ·Ó ·fi ÙË ¯ÂÈÚÔ˘ÚÁÈ΋ ‰È·‰Èηۛ· Ô˘ ¯ÚËÛÈÌÔÔÈ‹ıËΠÒÛÙ ӷ ‰ËÌÈÔ˘ÚÁËı› ÚfiÛ‚·ÛË ÁÈ· ÙËÓ ÙÔÔı¤ÙËÛË ÙÔ˘ Û‡ÚÌ·ÙÔ˜ ÚfiÛ‰ÂÛ˘. ∏ ‰È·‰Èηۛ· ·˘Ù‹ ‹Ù·Ó Ôχ ÈÔ ÂÎÙÂٷ̤ÓË Î·È ·ÊÔÚÔ‡ÛÂ Û˘¯Ó¿ ·ÔÎ¿Ï˘„Ë fiÏ˘ Ù˘ ̇Ï˘ Î·È ÌÈÎÚÔ‡ ÙÌ‹Ì·ÙÔ˜ Ù˘ Ú›˙·˜ ÛÙËÓ ÂÚÈÔ¯‹ Ù˘ ÔÛÙÂ˚ÓÔ·‰·Ì·ÓÙÈÓÈ΋˜ ¤ÓˆÛ˘. ™¯ÂÙÈο Ì ÙË ıÂڷ›· ÙˆÓ ·ÚÂȷο ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Û ۇÁÎÚÈÛË Ì ÙÔ˘˜ ·ÓÙ›ÛÙÔÈ¯Ô˘˜ ÌË ¤ÁÎÏÂÈÛÙÔ˘˜, ‚Ú¤ıËΠfiÙÈ Ë ·Ï‹ ¯ÂÈÚÔ˘ÚÁÈ΋ ·ÔÎ¿Ï˘„‹ ÙÔ˘˜ ›¯Â ‚Ï·ÙÈΤ˜ ÂȉڿÛÂȘ ÛÙÔ ÂÚÈÔ‰fiÓÙÈÔ (Tegsjö Î·È Û˘Ó., 1984; Boyd, 1984). ŸÛÔÓ ·ÊÔÚ¿ ÛÙËÓ Ù¯ÓÈ΋ ÎÏÂÈÛÙ‹˜ ·Ó·ÙÔÏ‹˜, ·Ú·ÙËÚ‹ıËΠÌÂȈ̤ÓÔ Â‡ÚÔ˜ ÚÔÛÂÊ˘ÎfiÙˆÓ Ô‡ÏˆÓ Î·È ·˘ÍË̤ÓÔ ÌÂÙÚÔ‡ÌÂÓÔ Â›Â‰Ô ÙÔ˘ Ê·ÙÓÈ·ÎÔ‡ ÔÛÙÔ‡ ÛÙ· ‰fiÓÙÈ· Ô˘ ·ÔηχÊıËÎ·Ó (Vermette Î·È Û˘Ó., 1995), ÂÓÒ ˘¿Ú¯Ô˘Ó Î·È ·ÓÙÈÎÚÔ˘fiÌÂÓ· ·ÔÙÂϤÛÌ·Ù· (Crescini Î·È Û˘Ó., 1994). ∂ÈϤÔÓ, Û¯ÂÙÈο Ì ÙÔÓ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fiÌÂÓÔ ÎÚËÌÓfi, ÔÈ Vermette Î·È Û˘Ó. (1995) ·Ó·Ê¤ÚÔ˘Ó ÛËÌ·ÓÙÈΤ˜ ‚Ï·ÙÈΤ˜ ÂȉڿÛÂȘ ÛÙÔ ÂÚÈÔ‰fiÓÙÈÔ, ·ÚfiÏÔ Ô˘ ÔÈ Tegsjö Î·È Û˘Ó. (1994) ‰ÂÓ ‚Ú‹Î·Ó ÛËÌ·ÓÙÈΤ˜ ‰È·ÊÔÚ¤˜ ÛÙËÓ ÂÚÈÔ‰ÔÓÙÈ΋ ηٿÛÙ·ÛË ÌÂٷ͇ ¤ÁÎÏÂÈÛÙˆÓ Î˘ÓÔ‰fiÓÙˆÓ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ·˘Ù‹ ÙË Ì¤ıÔ‰Ô Î·È ‰ÔÓÙÈÒÓ ÂϤÁ¯Ô˘. ∆¤ÏÔ˜, Û‡ÁÎÚÈÛË Ù˘ Ù¯ÓÈ΋˜ ÎÏÂÈÛÙ‹˜ ·Ó·ÙÔÏ‹˜ Ì ÙË Ì¤ıÔ‰Ô ÙÔ˘ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fiÌÂÓÔ˘ ÎÚËÌÓÔ‡ ·fi ÙÔ˘˜ Vermette Î·È Û˘Ó. (1995), ·ÔÎ¿Ï˘„ fiÙÈ ‰fiÓÙÈ· Ô˘ E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment 23 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7 ¢ONTIKH £O ET OP E§ ™ 1963 ¢O §A A PEI AI A.B. ME§KO™ Î·È Û˘Ó. ¶ÂÚÈÔ‰ÔÓÙÈο ÚÔ‚Ï‹Ì·Ù· Ô˘ Û¯ÂÙ›˙ÔÓÙ·È Ì ÙËÓ ¯ÂÈÚÔ˘ÚÁÈ΋ Î·È ÔÚıÔ‰ÔÓÙÈ΋ A.B. MELKOS et al. Periodontal aspects associated with the surgical and orthodontic treatment closed-eruption techniques. Angle Orthod 1995;65:23-34. Wisth PJ, Norderval K, Boe OE. Comparison of two surgical methods in combined surgical-orthodontic correction of impacted maxillary canines. Acta Odontol Scand 1976b;34:52-7. Wisth PJ, Norderval K, Boe OE. Periodontal status of orthodontically treated impacted maxillary canines. Angle Orthod 1976a;46:69-76. Wolf JE, Matilla K. Localisation of impacted maxillary canines by panoramic tomography. Dentomaxillofac Radiol 1979;8:85-91. Woloshyn H, Artun J, Kennedy DB, Joondeph DR. Pulpal and periodontal reactions to orthodontic alignement of palatally impacted canines. Angle Orthod 1994;64:257-64. Zachrisson BU, Alnaes L. Periodontal condition in orthodontically treated and untreated individuals. II. Alveolar bone loss: Radiographic findings. Angle Orthod 1974;44:48-55. ·ÔηχÊıËÎ·Ó Ì ÙËÓ Ù¯ÓÈ΋ ÙÔ˘ ·ÎÚÔÚÚÈ˙Èο ÌÂÙ·ÙÔÈ˙fiÌÂÓÔ˘ ÎÚËÌÓÔ‡ ·ÚÔ˘Û›·Û·Ó ÌÂÁ·Ï‡ÙÂÚ˜ ·ÈÛıËÙÈΤ˜ ÂÈÙÒÛÂȘ Û ۯ¤ÛË Ì ·˘Ù¿ Ô˘ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì ÙËÓ Ù¯ÓÈ΋ ÎÏÂÈÛÙ‹˜ ·Ó·ÙÔÏ‹˜ (Vermette Î·È Û˘Ó., 1995). ™YM¶EPA™MATA ™ÎÔfi˜ Ù˘ ÔÚıÔ‰ÔÓÙÈ΋˜ ıÂڷ›·˜ ‰ÂÓ Ú¤ÂÈ Ó· Â›Ó·È ÌfiÓÔ Ë ‰ÈfiÚıˆÛË Ù˘ Û˘ÁÎÏÂÈÛȷ΋˜ ‰È·Ù·Ú·¯‹˜, ·ÏÏ¿ Ë ‰ÈfiÚıˆÛË ·˘Ù‹ Ó· Á›ÓÂÙ·È Ì ÙȘ ÂÏ¿¯ÈÛÙ˜ ‰˘Ó·Ù¤˜ ·ÓÂÈı‡ÌËÙ˜ ·ÓÙȉڿÛÂȘ ·fi Ù· ‰fiÓÙÈ· Î·È ÙÔ˘˜ ˘ÔÛÙËÚÈÎÙÈÎÔ‡˜ ÈÛÙÔ‡˜. ∫·Ù¿ ÙË Û˘˙‹ÙËÛË ÂÓ·ÏÏ·ÎÙÈÎÒÓ ıÂڷ¢ÙÈÎÒÓ ‰È·‰ÈηÛÈÒÓ, Â›Ó·È ÛËÌ·ÓÙÈÎfi Ó· ÌÔÚ› ηÓ›˜ Ó· ÂÈϤÍÂÈ ÙÔ Â›‰Ô˜ ÂΛÓÔ Ù˘ ıÂڷ›·˜ Ô˘ ÚÔηÏ› ÙËÓ ÂÏ¿¯ÈÛÙË ‚Ï¿‚Ë. ¶·Ú¿ ÙȘ ˆ˜ ¤Ó· ‚·ıÌfi ·ÓÙÈÊ·ÙÈΤ˜ ÁÓÒ̘ ÙˆÓ ÂÚ¢ÓËÙÒÓ, ÌÔÚ› ηÓ›˜ Ó· Û˘ÌÂÚ¿ÓÂÈ fiÙÈ ÂËÚ¿˙ÔÓÙ·È Û¯Â‰fiÓ ¿ÓÙ· ÙfiÛÔ ÔÈ ·ÚÂȷο fiÛÔ Î·È ÔÈ ˘ÂÚÒÈ· ¤ÁÎÏÂÈÛÙÔÈ Î˘Ófi‰ÔÓÙ˜, ·ÓÂÍ¿ÚÙËÙ· ·fi ÙȘ ¯ÂÈÚÔ˘ÚÁÈΤ˜ ‹ ÙȘ ÔÚıÔ‰ÔÓÙÈΤ˜ ‰È·‰Èηۛ˜ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È. ∂Ó ÙÔ‡ÙÔȘ, Ê·›ÓÂÙ·È fiÙÈ ·Ó·Ì¤ÓÂÙ·È ÌÈÎÚfiÙÂÚË ÂÚÈÔ‰ÔÓÙÈ΋ ›‰Ú·ÛË fiÙ·Ó ÔÈ ÔÚıÔ‰ÔÓÙÈΤ˜ ‰˘Ó¿ÌÂȘ ÂÊ·ÚÌfi˙ÔÓÙ·È ÌÂÙ¿ ·fi ÎÏÂÈÛÙ¤˜ Ù¯ÓÈΤ˜ ¯ÂÈÚÔ˘ÚÁÈ΋˜ ·ÔÎ¿Ï˘„˘ ηٿ ÙȘ Ôԛ˜ Á›ÓÂÙ·È ·Ó‡„ˆÛË ÎÚËÌÓÔ‡, Û˘ÁÎfiÏÏËÛË Û˘Ó‰¤ÛÌÔ˘ Î·È Â·Ó·Û˘ÚÚ·Ê‹ ÙÔ˘ ÎÚËÌÓÔ‡ ÛÙËÓ ·Ú¯È΋ ÙÔ˘ ı¤ÛË. Reprint requests to: Moschos A. Papadopoulos Assistant Professor Department of Orthodontics School of Dentistry Aristotle University of Thessaloniki GR-54124 Thessaloniki Greece E-mail: [email protected] ¢È‡ı˘ÓÛË ÁÈ· ·Ó¿Ù˘·: ªfiÛ¯Ô˜ ∞. ¶··‰fiÔ˘ÏÔ˜ ∂›ÎÔ˘ÚÔ˜ ∫·ıËÁËÙ‹˜ ∂ÚÁ·ÛÙ‹ÚÈÔ √ÚıÔ‰ÔÓÙÈ΋˜ ∆Ì‹Ì· √‰ÔÓÙÈ·ÙÚÈ΋˜ ∞ÚÈÛÙÔÙ¤ÏÂÈÔ ¶·ÓÂÈÛÙ‹ÌÈÔ £ÂÛÛ·ÏÔӛ΢ 54124 £ÂÛÛ·ÏÔÓ›ÎË E-mail: [email protected] E§§HNIKH OP£O¢ONTIKH E¶I£EøPH™H 2004 ñ TOMO™ 7 24 HELLENIC ORTHODONTIC REVIEW 2004 ñ VOLUME 7
Scaricare