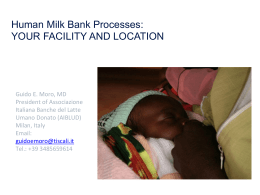
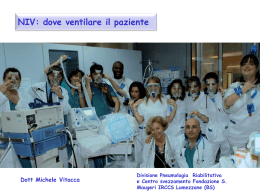
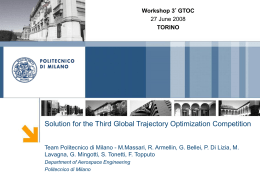
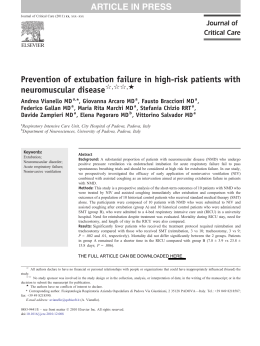
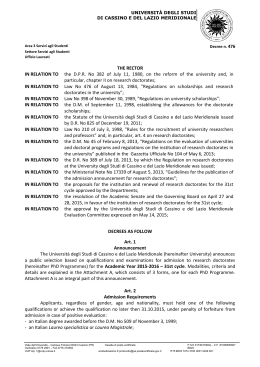
Improving Delivery Room Management for Very Preterm Infants abstract BACKGROUND AND OBJECTIVES: Events in the delivery room significantly impact the outcomes of preterm infants. We developed evidence-based guidelines to prevent heat loss, reduce exposure to supplemental oxygen, and increase use of noninvasive respiratory support to improve the care and outcomes of infants with birth weight #1250 g at our institution. METHODS: The guidelines were implemented through multidisciplinary conferences, routine use of a checklist, appointment of a dedicated resuscitation nurse, and frequent feedback to clinicians. This cohort study compares a historical group (n = 80) to a prospective group (n = 80, after guidelines were implemented). Primary outcome was axillary temperature at admission to the intensive care nursery. Secondary outcomes measured adherence to the guidelines and changes in clinically relevant patient outcomes. RESULTS: Baseline characteristics of the groups were similar. After introduction of the guidelines, average admission temperatures increased (36.4°C vs 36.7°C, P , .001) and the proportion of infants admitted with moderate/severe hypothermia fell (14% vs 1%, P = .003). Infants were exposed to less oxygen during the first 10 minutes (P , .001), with similar oxygen saturations. Although more patients were tried on continuous positive airway pressure (40% vs 61%, P = .007), the intubation rate was not significantly different (64% vs 54%, P = .20). Median durations of invasive ventilation and hospitalization decreased after the quality initiative (5 vs 1 days [P = .008] and 80 vs 60 days [P = .02], respectively). CONCLUSIONS: We have demonstrated significantly improved quality of delivery room care for very preterm infants after introduction of evidence-based delivery room guidelines. Multidisciplinary involvement and continuous education and reinforcement of the guidelines permitted sustained change. Pediatrics 2013;132:e1018–e1025 AUTHORS: Sara B. DeMauro, MD, MSCE,a,b Emily Douglas, MPH,a Kelley Karp, RN,b Barbara Schmidt, MD, MSc,b Jay Patel, MD,a,b Amy Kronberger, MSN, RNC-NIC,b Russell Scarboro, MA, RRT,b and Michael Posencheg, MDa,b aDepartment of Pediatrics, The Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania; and bThe Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania KEY WORDS preterm, temperature, thermal regulation, resuscitation, outcomes of high-risk infants ABBREVIATIONS CPAP—continuous positive airway pressure FiO2—fraction of inspired oxygen QI—quality improvement SpO2—oxygen saturation Dr DeMauro contributed to writing and editing all drafts of the manuscript, conception and design, and acquisition, analysis, and interpretation of data; Ms Douglas contributed to writing the first draft of the manuscript and to acquisition and analysis of data; Ms Karp contributed to acquisition of data and critical revision of the manuscript; Dr Schmidt contributed to study conception and design, interpretation of the data, and critical revision of the manuscript; Ms Kronberger contributed to study conception and design and critical revision of the manuscript; Mr Scarboro contributed to study conception and design and critical revision of the manuscript; Dr Patel contributed to study conception and design, acquisition of data, and critical revision of the manuscript; Dr Posencheg contributed to drafting and critical revision of the manuscript, conception and design, and analysis and interpretation of data; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2013-0686 doi:10.1542/peds.2013-0686 Accepted for publication Jun 17, 2013 Address correspondence to Sara DeMauro, MD, MSCE, The Children’s Hospital of Philadelphia, 2nd Floor Main Building, Division of Neonatology, 34th Street and Civic Center Boulevard, Philadelphia, PA 19104. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2013 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: No external funding. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. e1018 DeMAURO et al QUALITY REPORT Events that occur in the first moments of life can have considerable short-term and long-term consequences, especially for very preterm infants. Specifically, 3 aspects of newborn care that require prompt attention in the delivery room are thermoregulation, respiratory management, and oxygen delivery. Hypothermia in the newborn is associated with much significant morbidity, including hypoglycemia, respiratory distress, hypoxia, and metabolic acidosis.1,2 The preterm infant is particularly susceptible to hypothermia. In the EPICure cohort, admission temperature ,35°C was present in 40% of infants ,26 weeks’ gestation and was independently associated with mortality.2 Several interventions, including plastic hats and wraps, warmer mattresses, and warm delivery rooms, have been shown to improve admission temperatures for preterm infants, but the majority of infants still become cold.3–12 Normal postnatal transition is associated with a slow rise in oxygen saturation from ∼60% to 90% over the first 5 to 10 minutes.13–16 Yet it is common practice to provide supplemental oxygen, often without monitoring or specific saturation goals, during neonatal resuscitation. Recent studies have suggested possible harm associated with the use of supplemental oxygen during resuscitation of term infants.16–21 In preterm infants, active titration of oxygen during resuscitation allows more infants to achieve saturations within a goal range, and initiation of resuscitation with ,100% oxygen results in similar heart rates during resuscitation and lower rates of bronchopulmonary dysplasia.22–25 Several observational and randomized clinical studies have compared immediate intubation and ventilation to use of noninvasive respiratory support for preterm infants in the delivery room.26–31 All of these studies reported trends toward decreased rates of death or PEDIATRICS Volume 132, Number 4, October 2013 bronchopulmonary dysplasia in infants initially managed with continuous positive airway pressure (CPAP). Although many infants who initially received CPAP eventually required intubation, there was no evidence of harm associated with early use of CPAP. At the Hospital of the University of Pennsylvania, we were inconsistently using a warmermattressorplasticwrap to prevent hypothermia, initiating resuscitation with 80% oxygen, and intubating all infants with birth weight ,750 g or gestational age #26 weeks. Given the current literature, we designed an intervention to prevent heat loss, reduce exposure to supplemental oxygen, and increase the use of CPAP during delivery room resuscitation of infants with birth weights #1250 g. Our goal was to use quality improvement (QI) principals to standardize and improve the quality and safety of delivery room care for very preterm infants. METHODS Setting There are ∼4200 births per year at the Hospital of the University of Pennsylvania. The 38-bed level III intensive care nursery is staffed by neonatologists, fellows, residents, nurse practitioners, and physician assistants from the Division of Neonatology at the Children’s Hospital of Philadelphia, which is located adjacent to our hospital, and respiratory therapists and nurses based at the Hospital of the University of Pennsylvania. After birth, very preterm infants are immediately brought to an adjoining resuscitation room. Initial resuscitation is provided with the NeoPuff device (Fisher & Paykel Healthcare Inc, Irvine, CA), and then patients are rapidly transitioned to a Dräger Baby-Log ventilator (Dräger Medical Inc, Telford, PA) for ongoing invasive or noninvasive respiratory support. Infants are transported to the intensive care nursery after stable respiratory status has been established and umbilical lines have been placed. Planning and Implementation of the Intervention A multidisciplinary team of neonatologists, nurses, and respiratory therapists performed a thorough review of the literature and then crafted evidence-based guidelines for the delivery room care of infants with birth weight #1250 g. The group presented their detailed recommendations to the Division of Neonatology at a formal conference in June 2010. The guidelines were circulated and there was an opportunity for discussion and modifications. The final guidelines are displayed in Fig 1. The guidelines were implemented between June and September 2010. Inservicing of the staff consisted of small-group sessions with a slide show and hands-on practice with the heat loss prevention equipment. Several approaches have ensured continued enforcement of the guidelines. A checklist is used to guide the team through important steps before and after delivery (Supplemental Information). Multidisciplinary simulation training is used to reinforce the key elements of the initiative. A dedicated resuscitation nurse attends all daytime deliveries and is responsible for ongoing training of clinical staff. Several key process measures, including completion of the checklist, use of thermoregulation equipment, and details of respiratory management and oxygen administration, are reviewed after each resuscitation and then the clinicians receive direct feedback. To identify opportunities for process improvement, the QI and clinical teams debrief within 24 hours of an admission of a hypothermic infant. Process control charts are used to continually monitor admission temperatures and are discussed with the faculty each month. In addition, data about delivery room e1019 approved by the Institutional Review Board at the University of Pennsylvania. Analysis Based on the literature, we assumed an SD in admission temperature of 0.8°C.3 A sample size of 80 per group was planned to allow 90% power to detect a difference of one-half of an SD (0.4°C). FIGURE 1 Guidelines for delivery room resuscitation of infants with birth weights #1250 g, adopted in June 2010. respiratory management and oxygen use are reviewed during monthly QI team meetings and then feedback is given to the clinicians. Evaluation of the Quality Improvement Initiative We performed a before/after cohort study to examine the impact of our clinical practice change. This cohort study compared a historical control group (“Epoch 1”) and a prospective group (after implementation of the QI initiative, “Epoch 2”). Eligible infants were born at our institution with a birth weight #1250 g. Infants were excluded if the family and clinical team had plans for “no aggressive measures” or “do not resuscitate.” Retrospective data about the historical control group were collected from patient registration logs maintained in the nursery and from electronic medical records. Prospective data were collected from patient charts throughout hospitalization. The outcomes of this cohort study were selected to measure both the e1020 DeMAURO et al effectiveness of the implementation of the new guidelines and the impact of these changes on patient outcomes. The primary outcome was axillary temperature at the time of admission to the intensive care nursery. Secondary outcome measures included the proportion of infants who were hypothermic at admission, amount of supplemental oxygen administered and corresponding oxygen saturations (SpO2), incidence of intubation without a trial of CPAP, mode(s) of respiratory support during resuscitation, and several clinically relevant patient outcomes. All temperatures were classified based on World Health Organization definitions: hyperthermia .37.5°C, normal 36.5°C to 37.5°C, cold stress/mild hypothermia 36.0°C to 36.4°C, moderate hypothermia 32.0°C to 35.9°C, and severe hypothermia ,32.0°C.32 We defined bacterial sepsis as a positive blood culture and necrotizing enterocolitis based on both clinical and radiologic or surgical evidence. The study was Baseline characteristics and outcomes were compared between the groups using t tests or Wilcoxon rank-sum tests for continuous data, depending on the distribution, and x 2 or Fisher’s exact tests for dichotomous data, depending on the sample size. Because continuous staff education and feedback were expected to lead to improved quality over time, changes in admission temperature, incidence of intubation without an attempt to use noninvasive respiratory support, and supplemental oxygen (FiO2) exposure at 5 minutes of life were further evaluated with statistical process control (XMR or P) charts. To further analyze FiO2 exposure and SpO2, we calculated the rate of change of FiO2 or SpO2 for each patient over time. We then used linear mixed-effects models, which permit differential follow-up times and account for withinpatient correlation. This approach allowed us to include all observations and the age in minutes at which they occurred. The model included FiO2 or SpO2 as the outcome variable, epoch and time as fixed explanatory variables, and each individual patient’s intercept and slope as random effects, and was used to produce figures depicting average FiO2 and SpO2 over the first 20 minutes of life. Analyses were preformed with Stata IC/ 11 (StataCorp LP, College Station, TX) and statistical process control charts were created with QI Charts (Process Improvement Products, Austin, TX). We considered 2-sided P values #0.05 to be significant. QUALITY REPORT TABLE 2 Outcomes Related to the Quality Improvement Initiative RESULTS Eighty consecutively born infants were enrolled in the historical cohort (January 2009 to June 2010, “Epoch 1”). Eighty consecutively born infants were enrolled in the prospective cohort (October 2010 to January 2012, “Epoch 2”). Data collection occurred between September 2010 and June 2012. Baseline characteristics of the 2 groups were similar (Table 1). At least 1 temperature was recorded during resuscitation for 64 patients (80%) during Epoch 1 and 80 patients (100%) during Epoch 2. In Epoch 2, infants were significantly warmer during resuscitation (Table 2). Data for the primary outcome, axillary temperature at the time of admission to the intensive care nursery, was unavailable for 1 infant in Epoch 1 who did not survive the initial resuscitation. There was a significant increase in admission temperature (36.4°C vs 36.7°C, P , .001) in Epoch 2. The proportion of infants who were admitted with temperatures in the normothermic range increased from 53% to 76% (P = .002) and the proportion of infants who were admitted with moderate or severe hypothermia decreased from 14% to 1% (P = .003). In Epoch 1, 1 infant was hyperthermic at the time of admission. In Epoch 2, 2 infants were admitted with Epoch 1 (n = 80) Epoch 2 (n = 80) P value 36.3 (0.8) 36.4 (0.8) 36.6 (0.6) 36.6 (0.6) 36.7 (0.4) 36.8 (0.4) 0.01 ,0.001 0.02 32 (40) 49 (61) 0.007 0.82 16 (53) 13 (43) 1 (3) 27 (55) 19 (39) 3 (6) 11 (37) 15 (50) 3 (10) 1 (3) 51 (64) 46 (58) 18 (37) 22 (45) 7 (14) 2 (4) 43 (54) 28 (35) 0.20 0.004 77 (25) 80 (22) 67 (27) 39 (23) 48 (24) 50 (28) ,0.001 ,0.001 ,0.001 60 (32) 68 (29) 81 (24) 55 (26) 70 (24) 85 (18) 0.47 0.61 0.32 Temperature Temperature during resuscitationa NICU admission temperature Second temperature in NICU Respiratory support Any use of CPAP during resuscitation Starting level of CPAP, cm H2O 5 6 7 Highest level of CPAP, cm H2O 5 6 7 8 Intubated in resuscitation roomb Intubated without trial of CPAP Supplemental oxygen Fraction inspired oxygen, %c 0–1 min of life 2–5 min of life 6–10 min of life Oxygen saturation, %c 0–2 min of life 2–5 min of life 6–10 min of life 0.94 All data are displayed as mean (SD) or n (%); temperatures are reported in °C. Outcomes include patients for whom the data are available and were recorded in the infant resuscitation room unless otherwise indicated. a If more than 1 temperature was obtained during the resuscitation, the first recorded temperature was used. b This outcome excludes 1 patient in Epoch 2 who was intubated for surfactant only. c The first available data point from each time interval was included. temperatures of 37.6°C, just above the upper limit of normal. Figure 2A is a process control chart for admission temperature, demonstrating both a sustained increase in average admission temperature and decreased variability, reflected in the narrowing of TABLE 1 Selected Baseline Characteristics and Delivery Room Interventions Baseline characteristics Gestational age, wk Birth weight, g Female Cesarean section 1-min Apgar score #3 5-min Apgar score #3 Antenatal steroid therapy ($2 doses) Delivery room interventions Umbilical artery catheter Umbilical vein catheter Surfactant Epinephrine Chest compressions Normal saline bolus All data are displayed as mean (SD) or n (%). PEDIATRICS Volume 132, Number 4, October 2013 Epoch 1 (n = 80) Epoch 2 (n = 80) P value 27.2 (2.5) 890 (224) 40 (50) 49 (61) 42 (53) 12 (15) 47 (59) 27.1 (2.6) 903 (245) 39 (49) 48 (60) 37 (46) 8 (10) 46 (58) 0.88 0.74 0.87 0.87 0.43 0.34 0.87 64 (80) 74 (93) 48 (60) 6 (8) 8 (10) 17 (21) 65 (81) 74 (93) 39 (49) 0 (0) 3 (4) 15 (19) 0.84 0.99 0.18 0.03 0.21 0.69 the control limits. The early shift of the mean line, just before formal guideline implementation, may represent increasing recognition of the importance of temperature regulation even while the guidelines were still under development. The new guidelines did not lead to a statistically significant decrease in the number of delivery room intubations (Table 2). However, the percent of patients who were intubated without a trial of noninvasive support decreased over time (Fig 2B). The delayed shift of the mean line in Fig 2B reflects the ongoing work of the QI team after formal implementation of the guidelines, providing frequent feedback to the clinicians. Of those who were tried on CPAP, there was not a significant change in the failure rate in Epoch 2 (19% vs 31%, P = .23). We did not observe a change in the pressure at e1021 exposed to less supplemental oxygen during Epoch 2 (Fig 2C). Linear mixedeffects models were used to combine all FiO2 and SpO2 data collected on individual patients over the first 20 minutes of life and develop the curves depicted in Figs 3 A and B. These figures describe average FiO2 (Fig 3A) and SpO2 over time (Fig 3B) during the 2 Epochs. During Epoch 1, the FiO2 started at ∼80% and was weaned to ∼60% by 10 minutes. During Epoch 2, the FiO2 started at ∼40% and was titrated to ∼50% by 10 minutes. Despite these differences, oxygen saturations were nearly identical in the 2 groups. We observed improvements in several in-hospital outcomes after implementation of the new guidelines (Table 3). Infants required fewer days of mechanical and noninvasive ventilation and were less likely to receive postnatal steroids for treatment of chronic lung disease. The median length of hospital stay decreased from 80 days to 60 days (P = .02). As balancing metrics, we did not observe increased rates of admission hyperthermia or pneumothorax or any other evidence of harm during Epoch 2. Importantly, there were no competing QI programs aimed at these outcomes during our observation period. DISCUSSION FIGURE 2 Statistical process control charts of A, axillary temperature at the time of admission to the intensive care nursery (XMR chart); B, percent of infants who underwent endotracheal intubation without a trial of CPAP (P chart); and C, percent supplemental oxygen administered at 5 minutes of life (XMR chart), per 5 consecutive patients and separated by Epoch. UCL, upper control limit; LCL, lower control limit. which CPAP was started or the maximum pressure to which CPAP was titrated. In Epoch 2, the average maximum amount of CPAP support for infants who “failed” CPAP (n = 15) was only 5.7 6 0.9 cm. A single infant in Epoch 2 was treated with surfactant and then placed back on CPAP. In post hoc analyses, successful use of CPAP e1022 DeMAURO et al was not significantly related to gestational age, birth weight, or antenatal steroid exposure in this population. Monthly review of resuscitation data revealed close compliance with the FiO2 titration guidelines. The process control chart for FiO2 recorded closest to 5 minutes, as a measure of compliance, demonstrates that patients were We have demonstrated successful implementation of evidence-based guidelines for delivery room management of very preterm infants at our institution. We observed a significant increase in the proportion of infants who were normothermic when admitted to the nursery, more infants were given a trial of CPAP, and infants were exposed to less supplemental oxygen during resuscitation. The quality initiative was associated with significant improvements in several important patientcentered outcomes, including shorter duration of ventilation and length of QUALITY REPORT initiative. Despite the decreased use of supplemental oxygen during Epoch 2, oxygen saturations were nearly identical. These results are consistent with the published trials of supplemental oxygen titration in preterm infants on which our guidelines were based.24 FIGURE 3 A, Predicted fraction of inspired oxygen (FiO2). B, Oxygen saturations over the first 20 minutes of life, by Epoch, with 95% confidence limits. Curves are based on linear mixed-effects models that incorporate all available data. Epoch 1 is indicated by solid lines and Epoch 2 is indicated by dashed lines. stay. Equally importantly, we have demonstrated that an approach to QI in the neonatal ICU that uses a multifaceted or “bundled” package of changes is feasible and can result in substantial improvements in clinical care. Previous research has demonstrated that although individual interventions such as a warmer mattress or occlusive wrap will raise infant temperatures, they do not provide sufficient protection to ensure normothermia.3–12 Our unique approach to prevention of heat loss bundled the multiple strategies that raise infant temperatures by small increments. Ours is the first study to demonstrate both an increase in average PEDIATRICS Volume 132, Number 4, October 2013 admission temperatures to the normal range and a substantial majority of patients with admission temperatures in the normal range. Importantly, our infants are at high risk for preadmission heat loss because it is local practice to place umbilical lines before transfer to the nursery. Nevertheless, our bundle safely and effectively maintained infant temperatures in the normothermic range throughout resuscitation and until admission, without causing hyperthermia. The significant difference in oxygen exposure between groups throughout the first 10 minutes of life is furtherevidence of successful implementation of the QI Increasing evidence suggests that outcomes of infants who are managed with delivery room CPAP are at least equal to, and potentially better than, outcomes of those who are immediately intubated.27,31,33,34 Despite the lack of a statistically significant decrease in delivery room intubations, our results are similar to previous studies that demonstrated associations between increased use of delivery room CPAP and decreased duration of mechanical ventilation or oxygen dependence.27,31 One explanation for these results could be that the QI intervention was associated with a culture shift toward decreased dependence on endotracheal intubation and increased use of noninvasive support throughout the hospitalization. Alternately, reduced exposure to hyperoxia and hypothermia in the immediate postnatal period is associated with overall clinical improvements in very preterm infants. Finally, our less aggressive approach to respiratory management was associated with lower rates of cardiopulmonary resuscitation. This is consistent with the SUPPORT Trial, in which the rate of epinephrine use was 4.1% in the intubation/surfactant group and only 2.0% in the CPAP group, and could have led to improved patient outcomes.33 There are several potential reasons that we have not yet observed a statistically significant decrease in the number of infants intubated in the delivery room, despite the increased use of CPAP. It is possible that our sample size was too small to detect differences in this outcome. Alternately, as discussed earlier, we first provide CPAP with a face mask and NeoPuff device and then transition e1023 TABLE 3 Respiratory and Other Clinical Outcomes Epoch 1 (n = 80) Epoch 2 (n = 80) P value Respiratory outcomes Supplemental oxygen at 36 wk Steroid treatment of lung disease Pneumothorax Duration of invasive ventilation, daysa Duration of noninvasive ventilation, daysa 16 (24) 12 (17) 3 (4) 5 (1, 31) 26 (8, 39) 15 (22) 2 (3) 3 (4) 1 (0, 3) 18 (3, 30) 0.76 0.004 0.99 0.008 0.04 Other clinical outcomes Deathb Early bacterial sepsis Late bacterial sepsis Grade III/IV intraventricular hemorrhage Patent ductus arteriosus Retinopathy of prematurity requiring surgery Necrotizing enterocolitis Length of hospitalization, daysa 12 (15) 5 (6) 12 (18) 13 (17) 30 (42) 2 (3) 10 (14) 80 (59, 100) 11 (14) 2 (3) 17 (22) 7 (9) 28 (37) 3 (4) 8 (11) 60 (50, 80) 0.80 0.44 0.48 0.16 0.55 0.99 0.55 0.02 All data are displayed as n (%) or median (interquartile range). These results are for patients who survived long enough to have the outcome assessed and for whom the outcome is known. a These results are for patients who were discharged to home from the birth hospital and do not include those who died or were transferred. b Vital status is unknown for 1 infant who was lost to follow-up after transfer. toappropriately sized nasal CPAP prongs (3 sizes available, Medicomp Medical, Princeton, MN) and the ventilator. Our QI initiative did not include a change to newer devices for respiratory support, such as bubble CPAP, which has been reported to reduce extubation failure in this population.35,36 This choice of equipment may be associated with our incidence of CPAP failure. We do not have data about the timing of CPAP administration or the duration of CPAP use before infants were declared to have “failed,” both of which will be important factors in determining next steps in our QI process. The guidelines suggest that clinicians titrate CPAP “up to 8 cm as needed to reduce work of breathing and oxygen requirement”; however, the maximum level of CPAP in the group who “failed” was ,6 cm. In addition, only 1 infant underwent INtubate-SURfactantExtubate (“INSURE”) as recommended for spontaneously breathing infants with significant work of breathing. Previous studies have demonstrated that policies encouraging use of CPAP are increasingly successful over time, as staff experience increases.27,31 As clinicians become more accustomed to the use of CPAP in the resuscitation room, we anticipate that they will be more comfortable employing the INSURE method of surfactant administration and titrating to higher levels of support before resorting to intubation. In balance, changes in delivery room management of very preterm infants did not lead to increases in hyperthermia, pneumothorax, or need for cardiopulmonary resuscitation in the delivery room. We did not observe any adverse effects associated with our evidencebased resuscitation guidelines. QI initiative. The nurses and respiratory therapists who are primarily responsible for implementation of several aspects of the guidelines were involved from the beginning. Therefore, the entire staff was, and remains, invested in the success of the program. The presence of the checklist and delivery room nurse during resuscitations, group feedback after each delivery, and the ongoing work of the QI team, reviewing resuscitation data and process charts with the clinical team at least monthly, together allow for continuous reinforcement of the recommendations. In next steps, we will develop a modified version of the guidelines for low birth weight infants between 1250 and 2000 g and evaluate alternate strategies to improve our use of delivery room CPAP. Our study has several important limitations. With our sample size, we did not have adequate power to draw conclusions about relationships between the QI initiative and less common patient outcomes. In addition, as with all observational studies, we can report associations, but cannot conclude that our practice change directly caused the clinical outcomes that we report. CONCLUSIONS Several important factors are likely to have contributed to the success of this We have demonstrated significantly improved quality of delivery room care for very premature infants at our institution with the implementation of evidence-based guidelines that address 3 aspects of delivery room management. The success of this QI intervention was possible with multidisciplinary involvement and continuous reinforcement of the guidelines. 2. Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR. The EPICure study: outcomes to discharge from hospital for infants born at the threshold of viability. Pediatrics. 2000;106(4):659–671 3. Trevisanuto D, Doglioni N, Cavallin F, Parotto M, Micaglio M, Zanardo V. Heat loss prevention in very preterm infants in delivery rooms: a prospective, randomized, controlled trial of polyethylene REFERENCES 1. Silverman WA, Fertig JW, Berger AP. The influence of the thermal environment upon the survival of newly born premature infants. Pediatrics. 1958;22(5): 876–886 e1024 DeMAURO et al QUALITY REPORT 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. caps. J Pediatr. 2010;156(6):914–917, 917 e911 Singh A, Duckett J, Newton T, Watkinson M. Improving neonatal unit admission temperatures in preterm babies: exothermic mattresses, polythene bags or a traditional approach? J Perinatol. 2010;30(1):45–49 Kent AL, Williams J. Increasing ambient operating theatre temperature and wrapping in polyethylene improves admission temperature in premature infants. J Paediatr Child Health. 2008;44(6):325–331 Lewis DA, Sanders LP, Brockopp DY. The effect of three nursing interventions on thermoregulation in low birth weight infants. Neonatal Netw. 2011;30(3):160–164 Chawla S, Amaram A, Gopal SP, Natarajan G. Safety and efficacy of Trans-warmer mattress for preterm neonates: results of a randomized controlled trial. J Perinatol. 2011;31(12):780–784 Brennan A. Effect of sodium acetate transport mattresses on admission temperatures of infants ,= 1500 grams [dissertation]. 1996 Knobel RB, Wimmer JE Jr, Holbert D. Heat loss prevention for preterm infants in the delivery room. J Perinatol. 2005;25(5):304–308 Roberts J. Use of a stockinet cap on premature infants after delivery [dissertation]; 1981 Vohra S, Roberts RS, Zhang B, Janes M, Schmidt B. Heat Loss Prevention (HeLP) in the delivery room: A randomized controlled trial of polyethylene occlusive skin wrapping in very preterm infants. J Pediatr. 2004;145(6):750–753 Vohra S, Frent G, Campbell V, Abbott M, Whyte R. Effect of polyethylene occlusive skin wrapping on heat loss in very low birth weight infants at delivery: a randomized trial. J Pediatr. 1999;134(5):547–551 Toth B, Becker A, Seelbach-Göbel B. Oxygen saturation in healthy newborn infants immediately after birth measured by pulse oximetry. Arch Gynecol Obstet. 2002;266(2):105–107 Rabi Y, Yee W, Chen SY, Singhal N. Oxygen saturation trends immediately after birth. J Pediatr. 2006;148(5):590–594 Kamlin CO, O’Donnell CP, Davis PG, Morley CJ. Oxygen saturation in healthy infants immediately after birth. J Pediatr. 2006;148 (5):585–589 Dawson JA, Kamlin CO, Vento M, et al. Defining the reference range for oxygen saturation for infants after birth. Pediatrics. PEDIATRICS Volume 132, Number 4, October 2013 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 2010;125(6). Available at: www.pediatrics. org/cgi/content/full/125/6/e1340 Vento M, Asensi M, Sastre J, García-Sala F, Pallardó FV, Viña J. Resuscitation with room air instead of 100% oxygen prevents oxidative stress in moderately asphyxiated term neonates. Pediatrics. 2001;107(4):642–647 Vento M, Asensi M, Sastre J, Lloret A, García-Sala F, Viña J. Oxidative stress in asphyxiated term infants resuscitated with 100% oxygen. J Pediatr. 2003;142(3):240–246 Vento M, Sastre J, Asensi MA, Viña J. Room-air resuscitation causes less damage to heart and kidney than 100% oxygen. Am J Respir Crit Care Med. 2005;172(11):1393–1398 Saugstad OD, Rootwelt T, Aalen O. Resuscitation of asphyxiated newborn infants with room air or oxygen: an international controlled trial: the Resair 2 study. Pediatrics. 1998;102(1):e1 Saugstad OD, Ramji S, Irani SF, et al. Resuscitation of newborn infants with 21% or 100% oxygen: follow-up at 18 to 24 months. Pediatrics. 2003;112(2):296–300 Rabi Y, Singhal N, Nettel-Aguirre A. Room-air versus oxygen administration for resuscitation of preterm infants: the ROAR study. Pediatrics. 2011;128(2). Available at: www. pediatrics.org/cgi/content/full/128/2/e374 Wang CL, Anderson C, Leone TA, Rich W, Govindaswami B, Finer NN. Resuscitation of preterm neonates by using room air or 100% oxygen. Pediatrics. 2008;121(6):1083–1089 Escrig R, Arruza L, Izquierdo I, et al. Achievement of targeted saturation values in extremely low gestational age neonates resuscitated with low or high oxygen concentrations: a prospective, randomized trial. Pediatrics. 2008;121(5):875–881 Vento M, Moro M, Escrig R, et al. Preterm resuscitation with low oxygen causes less oxidative stress, inflammation, and chronic lung disease. Pediatrics. 2009;124(3). Available at: www.pediatrics.org/cgi/content/full/124/3/e439 DeMauro SB, Roberts RS, Davis P, Alvaro R, Bairam A, Schmidt B. Impact of delivery room resuscitation on outcomes up to 18 months in very low birth weight infants. J Pediatr. 2011;159(4):546–550 e541 Aly H, Massaro AN, Patel K, El-Mohandes AA. Is it safer to intubate premature infants in the delivery room? Pediatrics. 2005;115(6): 1660–1665 Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB; COIN Trial Investigators. Nasal CPAP or intubation at birth 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. for very preterm infants. N Engl J Med. 2008;358(7):700–708 Finer NN, Carlo WA, Walsh MC, et al; SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med. 2010;362(21): 1970–1979 Dunn MS, Kaempf J, de Klerk A, et al; Vermont Oxford Network DRM Study Group. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics. 2011;128(5). Available at: www.pediatrics.org/cgi/content/full/128/5/e1069 Levesque BM, Kalish LA, LaPierre J, Welch M, Porter V. Impact of implementing 5 potentially better respiratory practices on neonatal outcomes and costs. Pediatrics. 2011;128(1). Available at: www.pediatrics. org/cgi/content/full/128/1/e218 Thermal Protection in Neonates. www.newbornwhocc.org/pdf/teaching-aids/2010/Thermalprotection-in-neonates-ENC4.pdf. Published 1997. Accessed January 23, 2013 Vaucher YE, Peralta-Carcelen M, Finer NN, et al; SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Neurodevelopmental outcomes in the early CPAP and pulse oximetry trial. N Engl J Med. 2012;367(26):2495–2504 Thomas CW, Meinzen-Derr J, Hoath SB, Narendran V. Neurodevelopmental outcomes of extremely low birth weight infants ventilated with continuous positive airway pressure vs. mechanical ventilation. Indian J Pediatr. 2012;79(2):218–223 Gupta S, Sinha SK, Tin W, Donn SM. A randomized controlled trial of post-extubation bubble continuous positive airway pressure versus Infant Flow Driver continuous positive airway pressure in preterm infants with respiratory distress syndrome. J Pediatr. 2009;154(5):645–650 Tagare A, Kadam S, Vaidya U, Pandit A, Patole S. Bubble CPAP versus ventilator CPAP in preterm neonates with early onset respiratory distress—a randomized controlled trial. J Trop Pediatr. 2013;59(2):113– 119 Kattwinkel J, ed. Textbook of Neonatal Resuscitation, 6th Edition. Elk Grove Village, IL: American Academy of Pediatrics; 2011 Yost CC, Soll RF. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev. 2000(2):CD001456 e1025
Scaricare