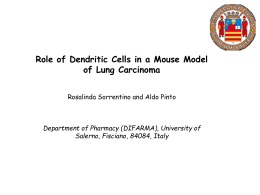
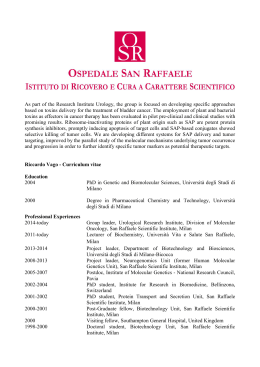
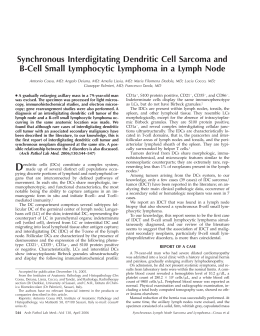
“Intestinal Kaposi’s sarcoma. A case report.” Rosanna Nenna, Daniela Di Clemente, Teresa Addati, Virginia Losito, Giusi Elicio, Pina Miscioscia, Cosimo Damiano Inchingolo Anatomic Pathology Unit L. Bonomo Andria - ASL BT OBJECTIVES Kaposi sarcoma (KS) is a low-grade vascular tumor associated with Human Herpes Virus 8 (HHV-8) infection. KS lesions evolve from early (patch stage) macules to plaques (plaque stage) that grow into larger nodules (tumor stage), these involve skin, mucosa, lymph nodes and rarely visceral, as well as respiratory and gastrointestinal tracts, developing in 1 of 4 different epidemiologic-clinical setting (classic, African, AIDS-associated and iatrogenic). We described a case of 64 years old female submitted to surgery (2013) to acute abdomen by suspected colon perforation. Previously, patient had a diagnosis of chronic ulcerative colitis on a rectal and colic biopsy and a nodular KS of the skin. METHODS Sixty-four years old woman was presented in surgery to acute abdomen by suspected colon perforation. Computed tomographic scan revealed free fluid in the abdominal cavity and diffuse thickening of the walls colic, compatible with injuries from rectum ulcerative colitis (RCU). Patient was submitted to left colectomy surgery for perforated abscess neoplasm suspected. We observed 55 cm left colectomy. In left colectomy we appreciated numerous polypoid nodules of the colic mucosa by necrotic-hemorrhagic appearance (diameter ranging from 0.6 cm to 2.2 cm). In pericolic adipose cellular there was a fistula between colon and abscess perforated cavity. By pericolic cellular fat ten lymph nodes were isolated. Microscopic analysis revealed a diffuse Kaposi sarcoma localizations in bowel and in two lymph nodes. Patient died two days from after surgery for resistant thrombocytopenia to platelet transfusion. a) TAC image b) Gross image radial section of large bowel, “Intestinal Kaposi’s sarcoma. A case report.” Rosanna Nenna, Daniela Di Clemente, Teresa Addati, Virginia Losito, Giusi Elicio, Pina Miscioscia, Cosimo Damiano Inchingolo Anatomic Pathology Unit L. Bonomo Andria - ASL BT RESULTS Histopathological final left colectomy diagnosis was: “Visceral Kaposi Sarcoma with diffuse and ulcerated polypoid nodular localization involving thickness of the colic wall complicated by fistula and perforated abscess and involving two lymph nodes”. Microscopically, nodules examination showed several fascicles of spindle-shaped tumor cells, with a chronic infiltrate inflammatory composed of lymphocytes, plasma cells and macrophages with hemosiderin in a bloody background characterized by slit like spaces. Spindle-shaped tumor cells showed pleomorphism and a significant number of mitotic figures. These features were confirmed by immunohistochemistry. The neoplastic cells showed a positive reaction for Vimentina, CD31, CD34, HHV-8 and a negative reaction for muscle actin HHF-35, CD117, DOG-1, S100 and Desmina. Mitotic index was 10/10 HPF. GRAPHS & TABLES b) d) a) d) f) c) e) g) a) Mucosal and sub-mucosal localization of KS (EE: 2.5X), b) Mucosal ulceration (EE: 10X), c) KS (EE: 40X), d) CD34 (40X), e) CD31 (40X), f) HHV-8 (40X), g) KI-67 (40X), “Intestinal Kaposi’s sarcoma. A case report.” Rosanna Nenna, Daniela Di Clemente, Teresa Addati, Virginia Losito, Giusi Elicio, Pina Miscioscia, Cosimo Damiano Inchingolo Anatomic Pathology Unit L. Bonomo Andria - ASL BT b) a) c) a) Perilinfonodal localization of KS (EE: 10X), b) CD34 (10X), c) HHV-8 (40X). CONCLUSIONS Kaposi sarcoma is a low-grade vascular tumor HHV-8 associated. The biological behavior of KS depends to epidemiology-clinical settings and lost immunity. Histopathology is the same in different settings and rare visceral involvement is associated with poor prognosis. The colic localization of KS and its complications are uncommon and critical, such as perforation and obstruction. This report shows that visceral KS could mimic RCU setting, mistaking diagnostic interpretation, if clinical history is not correctly reported. A clinic history and a previous diagnosis of KS skin (HHV-8 correlated) and immunodeficiency, as the RCU setting-like on endoscopic biopsy, could facilitate the clinical identification of non-specific symptoms and encourage early histological diagnosis in order to establish suitable therapies to prevent fatal complications. a) References 1.Radu O., Pantanowitz L. “Kaposi sarcoma” Arch Pathol Lab Med-Vol 137, February 2013: 289-294; 2.Arora M., Goldeberg E.M. “Kaposi sarcoma involving the gastrointestinal tract” Gastroenterology & Hepatology-Vol 6, Issue 7, July 2010: 459-462; 3.Egwuonwu S. et al. “Gastrointestinal Kaposi sarcoma with appendiceal involvement” South med J. 2011; 104: 278281; 4.Weber J.N. et al. “Kaposi’s sarcoma of the bowel-presenting as apparent ulcerative colitis” Gut, 2013 August, 26: 295300; 5.Majewski S. et al. “Nodular Kaposi’s sarcoma associated with colon cancer” Acta Dermatoven Vol 20, 2011, 83-85; 6.Zoufaly A. et al. “Intestinal Kaposi’s sarcoma may mimic gastrointestinal stromal tumor in HIV infection” World Journal of gastroenterology 2007 September 7; 13: 4514-4516.
Scaricare