European Journal of Clinical Nutrition (2013) 67, 536–540 & 2013 Macmillan Publishers Limited All rights reserved 0954-3007/13 www.nature.com/ejcn REVIEW Fish oil omega-3 fatty acids and cardio-metabolic health, alone or with statins Anne Marie Minihane The impact of the fish-derived omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) on cardiovascular disease (CVD) and type 2 diabetes incidence and risk has been widely investigated. Although the balance of evidence suggests substantial benefits with respect to CVD mortality, there is little evidence for an impact of these fatty acids on insulin sensitivity and diabetes incidence, despite very promising data from animal models. The focus here will be the plasma lipid modulatory effects of EPA and DHA and will include an exploration of the potential and demonstrated complementarity between statins and EPA/DHA on overall CVD risk and the plasma cholesterol and triglyceride profile. Although there is some justification for greater general population and patient EPA þ DHA intakes, an often overlooked major obstacle is that global fish stocks are limited and insufficient to meet demands. The potential of emerging ‘non-fish foods’ to provide affordable and sustainable sources of EPA þ DHA will also be briefly discussed. European Journal of Clinical Nutrition (2013) 67, 536–540; doi:10.1038/ejcn.2013.19; published online 13 February 2013 Keywords: omega-3 fatty acids; fish oils; EPA and DHA; cardiovascular; insulin sensitivity; plasma lipids INTRODUCTION Each year cardiovascular disease (CVD) causes over four million deaths in Europe and is responsible for 42% of total mortality in men and 52% in women.1 Through more effective acute post myocardial infarction and stroke management, extensive use of revascularisation procedures, lifestyle changes and widespread use of pharmacotherapy such as statins (HMGCoA reductase inhibitors), CVD death rates have dropped considerably over the past 30 years in northern and western Europe.1 However there are concerns that CVD morbidity and eventually mortality will once again rise due to the rapid escalation in the incidence of obesity and type 2 diabetes (T2DM) that now occurs in 8.3% of adults globally, with the number predicted to increase by 450% by 2030 (www.idf.org/diabetesatlas). Over the last 50 years, a large amount of research has been conducted on the cardiovascular benefits of the long-chain omega-3 fatty acids found in fish, namely eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), with 4400 papers on the topic published in EJCN in its 25-year lifetime. Although not fully consistent, the balance of evidence supports a role of EPA and DHA in both the primary and secondary prevention of CVD. The three-fold-increased CVD risk associated with adiposity and diabetes2 is manifested through classical and emerging risk factors such as insulin insensitivity, hypertrigylceridaemia, elevated small dense low-density lipoprotein (LDL), inflammation and vascular dysfunction, many of which are known to be responsive to omega-3 fatty acid intervention.3,4 The purpose of this paper is to provide an overview of the dietary sources, recommended intakes and sustainability of omega-3 fatty acids, along with their impact alone or in combination with statins on CVD and T2DM risk and on optimising the plasma lipid profile. Source and recommended intakes of omega-3 fatty acids In the diet, a-linolenic acid (aLNA) derived mainly from seed oils and the longer chain EPA and DHA from oily fish or fish oil supplements represent the main omega-3 fatty acids. Habitual intakes of aLNA of between 0.5–2.0% of dietary energy are recommended.5 Although there is some suggestions that aLNA may have independent cardioprotective benefits, its protection is mainly thought to occur when it replaces saturated fat in the diet or as a precursor for EPA and DHA synthesis.6 Although the process of elongation and desaturation that converts the aLNA (C18:3) to EPA and DHA is inefficient, with normally only 0.2–6% conversion to EPA and 0–0.5% to DHA in humans,7,8 for non-fish eaters, this pathway is responsible for the majority of tissue EPA and DHA.9 Undoubtedly direct consumption of EPA and DHA is the most effective means of improving status, with oily fish providing 1.5–3.5 g per portion (Table 1). Alternatively, EPA and DHA may be consumed as fish oil supplements or DHA-rich oil supplements derived from microalgae oil that is suitable for consumption by vegetarians. Omacor or MaxEPA represent commonly prescribed sources of the long-chain omega-3 fatty acids (Table 1). With the exception of pregnant females, current omega-3 fatty acid recommendations in adults are based on their cardioprotective actions. Although some variability exists, national and international organisations typically recommend a minimum of 0.5 g EPA þ DHA per day to be achieved through consumption of two portions of fish per week, one of which should be oily.10,11 In the UK, the National Institute for Health and Clinical Excellence (NICE) recommend that post-myocardial infarction patients should be advised to consume at least 7 g of omega-3 fatty acids per week from two to four portions of oily fish.12 For those not achieving this intake from fish, a 1 g ‘omega-3 ethyl ester’ Department of Nutrition, Norwich Medical School, University of East Anglia, Norwich, UK. Correspondence: Professor A Marie Minihane, Department of Nutrition, Norwich Medical School, University of East Anglia, Norwich NR4 7TJ, UK. E-mail: [email protected] Received 7 January 2013; accepted 10 January 2013; published online 13 February 2013 Fish oil omega-3 fatty acids and cardio-metabolic health A Marie Minihane 537 Table 1. Main dietary and supplementary sources of long-chain omega-3 fatty acids Source Herringa Mackerela Salmon (wild)a Salmon (canned)a Sardines (canned)a Tuna, bluefinb Tuna (canned)a,b Trouta Coda Plaicea Prawnsa Roast beef/pork/lamba Chickena Cod liver oil Omacor (Abbott HealthCare) MaxEPA (Seven Seas) 18: 3n-3 - Linolenic acid Δ6 Desaturase EPA þ DHAg/100 g 18: 4n-3 Stearidonic acid 1.2 1.8 1.8 1.4 1.6 1.5 0.2–0.3 1.1 0.2 0.3 0.1 0.02–0.05 0.03 19 (0.19 g/g capsule) 0.84 g/g capsule 0.29 g/g capsule Elongase 20: 4n-3 Eicosatetraenoic acid Δ5 Desaturase 20: 5n-3 EPA Elongase 22: 5n-3 DPA Abbreviations: DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid. a (BNF 1999). bKennedy et al. (2012).14 Elongase 24: 5n-3 Tetracosapentaenoic acid (Omacor) supplement is recommended. This dose of 1 g per day of EPA and DHA for secondary prevention is equivalent to that recommended by the American Heart Association (AHA).11 Current estimates indicate that for most countries, average population intakes of EPA and DHA are o0.2 g per day. However, given that oily fish or fish oil supplement intake trends are bimodal, these average consumption figures are misleading with regular oily fish consumers (o10% population) skewing the data to the right. For non-supplement users who eat oily fish less than once per month, that is, the vast majority of western populations, intakes are likely to be o0.05 g per day, i.e. 410-fold lower than the minimum recommended intake. For example, an Australian study reported a median intake of 0.03 g per day in adults with a mean intake of 0.19 g per day.13 In the UK, European Prospective Investigation into Cancer and Nutrition (EPIC) Norfolk cohort, EPA þ DHA intakes of 0.26 g per day were evident in fish-eaters with intakes of only 0.01–0.04 g per day in non-fish-eating vegan, vegetarians and meat eaters.9 Cost and global sustainability of EPA and DHA: a need for ‘non-fish’ sources Affordability of fish and supplements is a recognised major barrier to EPA and DHA intake. Calculations based on a recent publication estimate that an expenditure of h6–21 per month14(depending on oily fish oil source) is required to provide the minimum of 0.5 g EPA þ DHA per day, with consumption of this dose as either a standard fish oil or microalgae oil (see below) costing h3–5 and h20–25 per month respectively. Furthermore, although in principal increased intakes of EPA and DHA above current intakes either alone or as an adjunct to prescribed medications is likely to produce significant health benefits, in reality, existing dwindling worldwide marine stocks, which produce one million tonnes of fish oils annually, are wholly inadequate to meet any substantial increase in demand. The harvesting of Krill (small crustaceans, Euphausia superba) in the Antarctic Ocean has produced an alternative source of marine EPA þ DHA largely used by the aquaculture industry. A limited number of human randomised controlled trials (RCTs) have demonstrated that its bioefficacy is comparable to traditional fish oils.15 Although Krill has a large overall biomass, given its fundamental role near the bottom of the marine food chain, international treaties are in place to limit ‘over-fishing’ and & 2013 Macmillan Publishers Limited Δ6 Desaturase 24: 6n-3 Tetracosahexaenoic acid B-oxidation 22: 5n-3 DHA Figure 1. EPA and DHA biosynthesis. ensure sustainability of the species. Farmed marine microalgae (for example, Schizochytrium) provide a rich source of omega-3 fatty acids and in particular DHA16 suitable for vegetarians and vegans, but high production costs are a critical hurdle in terms of large-scale production. Land plant foods are devoid of EPA and DHA as they lack the desaturase enzymes necessary for the bioconversion (Figure 1). However, seeds and nuts are a significant source of the shorter chain aLNA, with commonly consumed oils such as rapeseed oil and soybean having B10% aLNA, with higher amounts found in the less frequently consumed flaxseed oil (45–55%). The initial step in the EPA/DHA biosynthesis pathway from aLNA, namely its conversion to stearidonic acid (SDA), catalysed by q6 desaturase is the rate-limiting step in the reaction. Consumption of SDA is low,17 but it leads to a more efficient conversion to EPA than does aLNA. The recently developed transgenic SDA-soybean holds considerable potential regarding a viable source of EPA in humans, with supplemental studies indicating enhanced plasma and tissue EPA status, with a bioequivalency of B5:1 following SDA soybean intervention (Note: see the Journal of Nutrition Mar 2012 supplemental issue on ‘Heart Health Omega-3 for food: stearidonic acid (SDA) as a sustainable choice’). However, little impact on DHA status following SDA-soybean oil has been observed. The recently developed EPA-rich Camelina oil (wildflax) also hold tremendous promise, although the complexities of the metabolic engineering of seed oils means that enhancing the levels of DHA in transgenic plants is a major challenge.18 European Journal of Clinical Nutrition (2013) 536 – 540 Fish oil omega-3 fatty acids and cardio-metabolic health A Marie Minihane 538 glucose and insulin metabolism,41 but recent studies using more physiological fish oil intakes have observed no effect. For example, in one of the largest RCTs conducted to date, the LIPGENE study, the addition of 1.2 g EPA þ DHA per day for 12 weeks had no impact on insulin sensitivity.42 In a 2008 Cochrane review that included 23 RCTs, no significant impact of fish oils on plasma glucose, insulin of HbA1c was evident.43 In a recent meta-analysis of prospective cohort studies, with follow-ups of 4.0–16.7 years, and 25 670 cases, no association between intakes of fish or seafood or EPA and DHA, nor circulating levels EPA and DHA biomarkers and incident T2DM was observed.44 However, considerable heterogeneity in association was evident with an additional 2012 meta-analysis, indicating geographical differences in the associations between EPA þ DHA status and intake and T2DM.45 The cardiovascular benefits of EPA and DHA Since the highly cited publications of Jørn Dyerberg and Hans Olaf Bang in Greenland Inuits,19 the impact of EPA and DHA on cardiovascular risk has been investigated in a large number of human association studies and secondary prevention trials. Although two recent meta-analyses of RCTs have cast a ‘shadow of a doubt’ on the benefits of EPA and DHA on a range of cardiovascular end-points,20,21 the comprehensive literature is, in general, supportive of their cardioprotective benefits.22–27 The underlying physiological mechanisms mediating the effects include:28 Anti-arrhythmic29 Improved heart rate30 Reduced platelet aggregation and thrombosis24 Improved endothelial and overall vascular function31 Reduce blood pressure32 Anti-inflammatory33 Increased plaque stability34 Hypotriglyceridaemia35 Increased high-density lipoprotein (HDL)-cholesterol36 Decreased LDL337 Impact of EPA and DHA on triglycerides and the atherogenic lipoprotein phenotype Although the literature is not suggestive of on overall protective impact of EPA and DHA on insulin sensitivity and T2DM risk, there is significant evidence to suggest that fish oils are particularly effective at counteracting the dyslipidaemia associated with obesity and T2DM, which is referred to as the atherogenic lipoprotein phenotype (ALP).46 Elevated circulating triglyceride (TG) levels are thought to be the metabolic driver of the dyslipidaemic triad of the (ALP) that is associated with lower HDL-cholesterol levels and an increased number of LDL particles in the small dense LDL3 form (Figure 2). As we have recently reviewed, TG, and in particular, non-fasting TG levels are a highly significant risk factor for CVD, with the size effects on CVD risk between extreme quintiles comparable to that of LDL- and totalcholesterol.47 Earlier studies using high doses of EPA and DHA (43 g per day) showed highly significant 20–50% reductions in fasting TG and associated modest increases in both LDL- and HDL-cholesterol,35 with hyperlipidaemic individuals being particularly responsive. In (ALP) men, we observed a 35 and 26% decrease in TG and LDL3 levels, respectively, following supplementation with 3 g EPA þ DHA per day, with no impact on HDL-cholesterol. This consistent TG-lowering effect of fish oil fatty acids, has led to the Responsiveness of the various CVD risk markers is very much dose-dependent with anti-arrhythmic actions evident at intakes as little as 200 mg per day, and intakes of 2–3 g per day thought to be needed to cause any meaningful reduction in the plasma inflammatory profile, vascular function and blood pressure.27,38,39 However, the distinct lack of adequately powered RCTs that have fed doses of EPA þ DHA of between 1–3 g per day, makes it difficult to conclude with any degree of certainty regarding the size effect of these intakes on individual CVD end-points. Impact of EPA and DHA on insulin sensitivity and diabetes risk Earlier animal studies that provided considerable evidence of the insulin-sensitising impact of increased EPA and DHA intakes,40 led to the suggestion that fish oils may positively modulate glucose and insulin metabolism in humans and thereby reduce T2DM risk and incidence. In fact, the earlier human RCTs were suggestive of the opposite; with a deleterious impact of fish oils on whole body More atherogenic relative to LDL1 and LDL2 ↑ small dense LDL3 LDL Enhanced inflammation HL TG CE CE CETP CE ↑ TRL TG HL Endothelial dysfunction ↑ small dense HDL3 CE enriched TRL remnants Sequesters cholesterol into artery wall TG Figure 2. HL HDL Rapidly removed from circulation decreasing HDL-C Free cholesterol, phospholipid, protein, CE Impact of increased triglyceride-rich lipoproteins on HDL & LDL metabolism. European Journal of Clinical Nutrition (2013) 536 – 540 & 2013 Macmillan Publishers Limited Fish oil omega-3 fatty acids and cardio-metabolic health A Marie Minihane 539 AHA recommending 2–4 g EPA þ DHA per day as an effective hypotrigylceridaemic dose.11 Although it was originally thought that such high intakes were necessary to bring about meaningful changes in TG, more recent RCTs have indicated that lower intakes can also be effective. In the FINGEN study, supplementation with 0.7 and 1.8 g EPA þ DHA per day resulted in group mean reductions in TG of 8% and 11%, with APOE4 carriers (25% Caucasians) and men being particularly responsive.48 There has also been considerable interest in establishing the individual impact of EPA versus DHA on plasma lipid and other CVD biomarkers, in particular in an era where the production of ‘tailor-made’ transgenic oils, with variable fatty acid composition is becoming increasingly feasible. Available evidence is suggestive that both EPA and DHA are TG-lowering with slightly greater reductions with DHA.49–51 DHA also appears to most effective at increasing the size of both LDL and HDL particles.50,51 Fish oils as an adjunct to statins Large clinical trials over the past two decades have established statins as a cost-effective, efficacious and first-line lipid lowering therapy.52,53 In the UK, statin therapy is recommended for adults with clinical evidence of CVD and as part of a management strategy for the primary prevention of CVD in adults who have a X20% 10-year risk of developing CVD.54 In patients at high risk of CVD events, there is currently a great deal of interest in the use of combined therapies driven by the observations that high-risk statin-treated patients often continue to have high rates of cardiovascular events, and the fact that TG levels are high correlates of residual risk in patients on statins.53,55,56 A number of adjunct lipid modulating therapies are available, including fibrates, niacin and fish oils, with combined therapies in particular recommended in patients with TG X500 mg/dl (7 mmol/l). The benefit of a combined statin plus fish oil has the effect of potentiating the TG-lowering, anti-inflammatory and vascularmodulating impact of both compounds with statins ameliorating the LDL-C elevation evident following high-dose fish oils in hyperlipidaemic individuals.35,37 In the Japan EPA Lipid Intervention Study (JELIS), 18 645 hypercholesterolaemic patients (total cholesterol 46.5 mmol/l) were assigned to statins or statins þ 1.8 g EPA per day. At 4.6-year follow-up, a 19% reduction in major coronary events was evident in the EPA-supplemented group along with a reduction in unstable angina and non-fatal coronary events.26 In subgroup analysis in patients with elevated TG (42.1 mmol/l) and low HDL-cholesterol (o1.1 mmol/l), a greater risk of coronary heart disease (hazards ratio, 95% confidence interval of 1.71, 1.11–2.64) was evident with a 53% reduction following EPA intervention.57 Subsequent short-term studies have confirmed that statins in combination with fish oils/EPA concentrate has a more favourable impact on plasma lipoproteins size and lipid concentrations than statins alone.58,59 CONCLUSION Multiple cardiovascular risk factors are positively affected by fish oil fatty acids. The lipid modulatory, and in particular, TG-lowering impact of EPA and DHA have been consistently described, with a relatively comprehensive understanding of dose-response relationships, at least at a population level. Although modest reductions in population LDL-cholesterol levels are evident over the last 25 years,60 raised TG levels are becoming increasingly prevalent due to its association with obesity and insulin resistance. Accumulating evidence, in particular, the output from the JELIS trial suggests that a statin þ EPA/DHA intervention may be a particularly effective therapy, and especially in those with elevated TG levels. In these individuals, it is likely that EPA/DHA will counteract a substantial portion of the residual risk following & 2013 Macmillan Publishers Limited statin intervention alone. However, further long-term studies with clinical end-points are needed to confirm the synergistic benefits of statins and omega-3 supplements on cardiovascular incidence and mortality. A more widespread use of omega-3 fatty acids will require the availability of a sufficient affordable supply, which could potentially be provided by novel transgenic seeds oils. The bioefficacy of these new oils, relative to fish oils, has not yet been comprehensively studied. CONFLICT OF INTEREST The author declares no conflict of interest. REFERENCES 1 Nichols M, Townsend N, Scarborough P, Rayner M. European Heart Network and European Society of Cardiology: European Cardiovascular Disease Statistics 2012. 2 Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364: 937–952. 3 Calder PC. Mechanisms of action of (n-3) fatty acids. J Nutr 2012; 142: 592S–599SS. 4 Roth EM, Harris WS. Fish oil for primary and secondary prevention of coronary heart disease. Curr Atheroscler Rep 2010; 12: 66–72. 5 Aranceta J, Perez-Rodrigo C. Recommended dietary reference intakes, nutritional goals and dietary guidelines for fat and fatty acids: a systematic review. Br J Nutr 2012; 107(Suppl 2): S8–22. 6 Pan A, Chen M, Chowdhury R, Wu JH, Sun Q, Campos H et al. alpha-Linolenic acid and risk of cardiovascular disease: a systematic review and meta-analysis. Am J Clin Nutr 2012; 96: 1262–1273. 7 Burdge GC. Metabolism of alpha-linolenic acid in humans. Prostaglandins Leukot Essent Fatty Acids 2006; 75: 161–168. 8 Burdge GC, Finnegan YE, Minihane AM, Williams CM, Wootton SA. Effect of altered dietary n-3 fatty acid intake upon plasma lipid fatty acid composition, conversion of [13C]alpha-linolenic acid to longer-chain fatty acids and partitioning towards beta-oxidation in older men. Br J Nutr 2003; 90: 311–321. 9 Welch AA, Shakya-Shrestha S, Lentjes MA, Wareham NJ, Khaw KT. Dietary intake and status of n-3 polyunsaturated fatty acids in a population of fish-eating and non-fish-eating meat-eaters, vegetarians, and vegans and the product-precursor ratio [corrected] of alpha-linolenic acid to long-chain n-3 polyunsaturated fatty acids: results from the EPIC-Norfolk cohort. Am J Clin Nutr 2010; 92: 1040–1051. 10 Scientific Advisory Committee on Nutrition (SACN) and Committee on Toxicology (COT). Advice on Fish Consumption: Benefits and Risks. TSO. The Stationary Office: Norwich, UK, 2004. 11 Kris-Etherton PM, Harris WS, Appel LJ. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002; 106: 2747–2757. 12 NICE. Post Myocardial Infarction Secondary Prevention in primary and Secondary Care for Patients Following a Myocardial Infarction. Royal College of General Practioners, 2007. 13 Meyer BJ, Mann NJ, Lewis JL, Milligan GC, Sinclair AJ, Howe PR. Dietary intakes and food sources of omega-6 and omega-3 polyunsaturated fatty acids. Lipids 2003; 38: 391–398. 14 Kennedy ET, Luo H, Ausman LM. Cost implications of alternative sources of (n-3) fatty acid consumption in the United States. J Nutr 2012; 142: 605S–609SS. 15 Vigerust NF, Bjorndal B, Bohov P, Brattelid T, Svardal A, Berge RK. Krill oil versus fish oil in modulation of inflammation and lipid metabolism in mice transgenic for TNF-alpha. Eur J Nutr 2012, e-pub ahead of print 28 August 2012. 16 Adarme-Vega TC, Lim DK, Timmins M, Vernen F, Li Y, Schenk PM. Microalgal biofactories: a promising approach towards sustainable omega-3 fatty acid production. Microb Cell Fact 2012; 11: 96. 17 Whelan J, Rust C. Innovative dietary sources of n-3 fatty acids. Ann Rev Nutr 2006; 26: 75–103. 18 Sayanova O, Napier JA. Transgenic oilseed crops as an alternative to fish oils. Prostaglandins Leukot Essent Fatty Acids 2011; 85: 253–260. 19 Dyerberg J, Bang HO. A hypothesis on the development of acute myocardial infarction in Greenlanders. Scand J Clin Lab Inves Suppl 1982; 161: 7–13. 20 Kwak SM, Myung SK, Lee YJ, Seo HG. Efficacy of omega-3 fatty acid supplements (eicosapentaenoic acid and docosahexaenoic acid) in the secondary prevention of cardiovascular disease: a meta-analysis of randomized, double-blind, placebocontrolled trials. Arch Int Med 2012; 172: 686–694. 21 Rizos EC, Ntzani EE, Bika E, Kostapanos MS, Elisaf MS. Association between omega3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis. JAMA 2012; 308: 1024–1033. European Journal of Clinical Nutrition (2013) 536 – 540 Fish oil omega-3 fatty acids and cardio-metabolic health A Marie Minihane 540 22 Delgado-Lista J, Perez-Martinez P, Lopez-Miranda J, Perez-Jimenez F. Long chain omega-3 fatty acids and cardiovascular disease: a systematic review. Br J Nutr 2012; 107(Suppl 2): S201–S213. 23 GISSI. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet 1999; 354: 447–455. 24 Harris WS, Miller M, Tighe AP, Davidson MH, Schaefer EJ. Omega-3 fatty acids and coronary heart disease risk: clinical and mechanistic perspectives. Atherosclerosis 2008; 197: 12–24. 25 Wang C, Harris WS, Chung M, Lichtenstein AH, Balk EM, Kupelnick B et al. n-3 Fatty acids from fish or fish-oil supplements, but not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: a systematic review. Am J Clin Nutr 2006; 84: 5–17. 26 Yokoyama M, Origasa H, Matsuzaki M, Matsuzawa Y, Saito Y, Ishikawa Y et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet 2007; 369: 1090–1098. 27 Musa-Veloso K, Binns MA, Kocenas A, Chung C, Rice H, Oppedal-Olsen H et al. Impact of low v. moderate intakes of long-chain n-3 fatty acids on risk of coronary heart disease. Br J Nutr 2011; 106: 1129–1141. 28 Adkins Y, Kelley DS. Mechanisms underlying the cardioprotective effects of omega-3 polyunsaturated fatty acids. J Nutr Biochem 2010; 21: 781–792. 29 Leaf A, Kang JX, Xiao YF, Billman GE. Clinical prevention of sudden cardiac death by n-3 polyunsaturated fatty acids and mechanism of prevention of arrhythmias by n-3 fish oils. Circulation 2003; 107: 2646–2652. 30 Mozaffarian D, Geelen A, Brouwer IA, Geleijnse JM, Zock PL, Katan MB. Effect of fish oil on heart rate in humans: a meta-analysis of randomized controlled trials. Circulation 2005; 112: 1945–1952. 31 Pase MP, Grima NA, Sarris J. Do long-chain n-3 fatty acids reduce arterial stiffness? A meta-analysis of randomised controlled trials. Br J Nutr 2011; 106: 974–980. 32 Campbell F, Dickinson HO, Critchley JA, Ford GA, Bradburn M. A systematic review of fish-oil supplements for the prevention and treatment of hypertension. Eur J Prev Cardiol 2012; 20: 107–120. 33 Calder PC. Fatty acids and inflammation: the cutting edge between food and pharma. Eur J Pharmacol 2011; 668(Suppl 1): S50–S58. 34 Thies F, Garry JM, Yaqoob P, Rerkasem K, Williams J, Shearman CP et al. Association of n-3 polyunsaturated fatty acids with stability of atherosclerotic plaques: a randomised controlled trial. Lancet 2003; 361: 477–485. 35 Harris WS. n-3 fatty acids and serum lipoproteins: human studies. Am J Clin Nutr 1997; 65(5 Suppl): 1645S–1654SS. 36 Balk EM, Lichtenstein AH, Chung M, Kupelnick B, Chew P, Lau J. Effects of omega-3 fatty acids on serum markers of cardiovascular disease risk: a systematic review. Atherosclerosis 2006; 189: 19–30. 37 Minihane AM, Khan S, Leigh-Firbank EC, Talmud P, Wright JW, Murphy MC et al. ApoE polymorphism and fish oil supplementation in subjects with an atherogenic lipoprotein phenotype. Arterioscler Thromb Vasc Biol 2000; 20: 1990–1997. 38 Mozaffarian D, Rimm EB. Fish intake, contaminants, and human health: evaluating the risks and the benefits. JAMA 2006; 296: 1885–1899. 39 Albert CM, Hennekens CH, O’Donnell CJ, Ajani UA, Carey VJ, Willett WC et al. Fish consumption and risk of sudden cardiac death. JAMA 1998; 279: 23–28. 40 Andersen G, Harnack K, Erbersdobler HF, Somoza V. Dietary eicosapentaenoic acid and docosahexaenoic acid are more effective than alpha-linolenic acid in improving insulin sensitivity in rats. Ann Nutr Metab 2008; 52: 250–256. 41 Nettleton JA, Katz R. n-3 long-chain polyunsaturated fatty acids in type 2 diabetes: a review. J Am Diet Assoc 2005; 105: 428–440. European Journal of Clinical Nutrition (2013) 536 – 540 42 Tierney AC, McMonagle J, Shaw DI, Gulseth HL, Helal O, Saris WH et al. Effects of dietary fat modification on insulin sensitivity and on other risk factors of the metabolic syndrome--LIPGENE: a European randomized dietary intervention study. Int J Obes (Lond) 2011; 35: 800–809. 43 Hartweg J, Perera R, Montori V, Dinneen S, Neil HA, Farmer A. Omega-3 polyunsaturated fatty acids (PUFA) for type 2 diabetes mellitus. Cochrane Database Syst Rev 2008; CD003205. 44 Wu JH, Micha R, Imamura F, Pan A, Biggs ML, Ajaz O et al. Omega-3 fatty acids and incident type 2 diabetes: a systematic review and meta-analysis. Br J Nutr 2012; 107(Suppl 2): S214–S227. 45 Wallin A, Di Giuseppe D, Orsini N, Patel PS, Forouhi NG, Wolk A. Fish consumption, dietary long-chain n-3 fatty acids, and risk of type 2 diabetes: systematic review and meta-analysis of prospective studies. Diabetes Care 2012; 35: 918–929. 46 Austin MA. Triglyceride, small, dense low-density lipoprotein, and the atherogenic lipoprotein phenotype. Curr Atheroscler Rep 2000; 2: 200–207. 47 Jackson KG, Poppitt SD, Minihane AM. Postprandial lipemia and cardiovascular disease risk: Interrelationships between dietary, physiological and genetic determinants. Atherosclerosis 2012; 220: 22–33. 48 Caslake MJ, Miles EA, Kofler BM, Lietz G, Curtis P, Armah CK et al. Effect of sex and genotype on cardiovascular biomarker response to fish oils: the FINGEN Study. Am J Clin Nutr 2008; 88: 618–629. 49 Buckley R, Shewring B, Turner R, Yaqoob P, Minihane AM. Circulating triacylglycerol and apoE levels in response to EPA and docosahexaenoic acid supplementation in adult human subjects. Br J Nutr 2004; 92: 477–483. 50 Cottin SC, Sanders TA, Hall WL. The differential effects of EPA and DHA on cardiovascular risk factors. Proc Nutr Soc 2011; 70: 215–231. 51 Mozaffarian D, Wu JH. (n-3) fatty acids and cardiovascular health: are effects of EPA and DHA shared or complementary? J Nutr 2012; 142: 614S–625S. 52 Gotto Jr. AM, Moon JE. Management of cardiovascular risk: the importance of meeting lipid targets. Am J Cardiol 2012; 110(1 Suppl): 3A–14A. 53 Maki KC, Bays HE, Dicklin MR. Treatment options for the management of hypertriglyceridemia: Strategies based on the best-available evidence. J Clin Lipidol 2012; 6: 413–426. 54 NICE. TA94: Statins for the Prevention of Cardiovascular Events. National Institute for Health and Clinical Excellence: London, 2006. 55 Dujovne CA, Williams CD, Ito MK. What combination therapy with a statin, if any, would you recommend? Curr Atheroscler Rep 2011; 13: 12–22. 56 Gotto Jr AM, Moon JE. Recent clinical studies of the effects of lipid-modifying therapies. Am J Cardiol 2012; 110(1 Suppl): 15A–26A. 57 Saito Y, Yokoyama M, Origasa H, Matsuzaki M, Matsuzawa Y, Ishikawa Y et al. Effects of EPA on coronary artery disease in hypercholesterolemic patients with multiple risk factors: sub-analysis of primary prevention cases from the Japan EPA Lipid Intervention Study (JELIS). Atherosclerosis 2008; 200: 135–140. 58 Ballantyne CM, Bays HE, Kastelein JJ, Stein E, Isaacsohn JL, Braeckman RA et al. Efficacy and safety of eicosapentaenoic acid ethyl ester (AMR101) therapy in statin-treated patients with persistent high triglycerides (from the ANCHOR Study). Am J Cardiol 2012; 110: 984–992. 59 Maki KC, Bays HE, Dicklin MR, Johnson SL, Shabbout M. Effects of prescription omega-3-acid ethyl esters, coadministered with atorvastatin, on circulating levels of lipoprotein particles, apolipoprotein CIII, and lipoprotein-associated phospholipase A2 mass in men and women with mixed dyslipidemia. J Clin Lipidol 2011; 5: 483–492. 60 Carroll MD, Lacher DA, Sorlie PD, Cleeman JI, Gordon DJ, Wolz M et al. Trends in serum lipids and lipoproteins of adults, 1960-2002. JAMA 2005; 294: 1773–1781. & 2013 Macmillan Publishers Limited
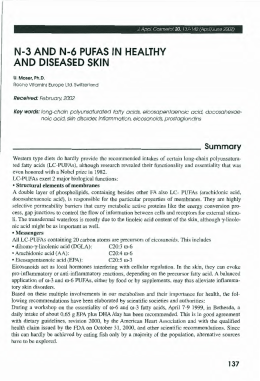
Scaricare