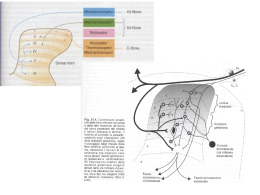
Recettore oppioidi mu, K, Delta (pre e post sinaptico) LIGANDE (pre e post sinaptico) Recettore oppioidi mu, K, Delta Endocitosi Apoptosi riciclo Recettore oppioidi mu, K, Delta Endocitosi Apoptosi riciclo la maggioranza dei endo-peptidi oppioidi subisce una rapida degradazione enzimatica (Egleton et al., 1998). vescicola Reticolo di Golgi vescicola Reticolo di Golgi Stimolo cronico BRADICHININA CAPSAICINA ATP-R Ca2+ vescicola Reticolo di Golgi MOR vescicola Reticolo di Golgi α β GAMMA ricevitore AP2: The AP2 adaptor complex works on the plasma membrane to internalise cargo G protein-coupled receptor kinase INTERNALIZZAZIONE riciclo degradazione E il LIGANDE CHE FINE FA? ENDOSOMA LISOSOMA LIGANDE la maggioranza dei peptidi oppioidi subisce una rapida degradazione enzimatica (Egleton et al., 1998).. La maggior parte degli enzimi extracellulari come il peptide di “degradazione” terminale sono legati alla membrana attraverso eso-ed endopeptidasi: l’aminopeptidasi N è uno di questi enzimi le cui azioni sono cruciali per il turn-over recettore/ligande . APN è un prodotto della proteasi transmembranaria in una vasta gamma di tessuti e tipi di cellule (endoteliali, epiteliali, fibroblasti, leucociti), che è in grado di modulare le risposte di peptidi bioattivi e di influenzare le funzioni immunitarie. CHEMIOTERAPICI . AMINOPEPTIDASI W o METALLOPROTEINASI DELLA MATRICE BESTATIN LEUCYL-AMINOPEPTIDASI METALLO PROTEASI DI MEMBRANA CHEMIOTERAPICI . AMINOPEPTIDASI W o METALLOPROTEINASI DELLA MATRICE BESTATIN LEUCYL-AMINOPEPTIDASI METALLO PROTEASI DI MEMBRANA . CO-SOMMINISTRAZIONE DI DIVERSE PEPTIDASI Bestatina + amastatin per inibire l’APN + Thiorphan, o Phosphoramidon per inibire la NEP Captopril per inibire l’enzima angiotensina Amino_Peptidasi - APN EndoPeptidasi neutra - NEP neutral endopeptidase (NEP) L’AMINO PEPTIDASI N è responsabile della degradazione di diversi peptidi biologicamente attivi, substrati compresi Enkerphaline, neurochinina A e beta-EP quindi, può essere considerato come un utile marker clinico. Si può prevedere che l'attività dei peptidi oppioidi a comando neurale sia potenziato da inibitori delle peptidasi. Endopeptidasi neutra (NEP) L'effetto antinocicettivo (intra tecale) somministrando Phosphoramidon + Bestatina IT RISPOSTA : si valuta la zampa in cui viene iniettata la capsaicina che induce IL TOPO inizialmente a leccare e successivamente mordere il sito di iniezione come massima risposta (autolesionismo), RISPOSTA che viene significativamente antagonizzata dal naltrindole, antagonista selettivo dei DOR. . Si può prevedere che l'attività dei peptidi oppioidi a comando neurale è potenziato dagli inibitori delle peptidasi. peptidi oppioidi Peptidasi peptidi oppioidi Peptidasi inibitori peptidasi peptidi oppioidi Peptidasi inibitori peptidasi + Attività peptidi oppioidi - peptidi oppioidi Peptidasi inibitori peptidasi + Attività peptidi oppioidi - peptidi oppioidi BESTATINA inibitori peptidasi + Attività peptidi oppioidi - Come un potente inibitore della APN, la sua azione a livello del sistema immunitario è stata ricercata, per le sue funzioni di molecola capace di “modificare” alcune risposte immunologiche (Umezawa et al, 1976;. Mathe, 1991), o il recupero immunologico (immunorecovery, Bruley-Rosset et al, 1979. . Ota e Ogawa, 1990), l’ematopoiesi (Talmadge et al, 1990), l’antinocicezione (Mathe, 1991 Ozaki et al. (1994) firstly discovered that Bestatin could increase the ileal twitch inhibitory potency caused by ME as well as transient inhibition of twitch contraction after tetanic stimulation. These results suggested that Bestatin-sensitive aminopeptidase participated in the post-tetanic twitch inhibition. After a further study, the quantitatively different mechanisms of action in the opioid system between Bestatin and morphine were elucidated based on the fact that when challenged with NLX after a long exposure to the Bestatin and morphine respectively, the former didn’t induce any NLXinduced contraction which morphine did although they had similar effects on the post-tetanic contraction, which suggested the possibility that Bestatin had a smaller dependence liability (Ozaki, 2002). La strategia da sviluppare: insieme all’analgesico fisiologico “ligande ideale”, privo degli effetti collaterali (endomorphin), è l'applicazione degli inibitori e dei bloccanti le peptidasi (inibizione del metabolismo delle peptidasi) AEA CBR AEA CBR AEA CBR AEA CBR FAAH inhibition increases the duration of anandamide’s analgesic effect, prolonging pain relief at the site of release…. read more: http://www.faqs.org/sec-filings/091116/INFINITYPHARMACEUTICALS-INC_8-K/dex991.htm#ixzz1HWjiSiVv AEA CBR IPI 940 AEA CBR IPI 940 INIBITORI “DUALI” una volta all'interno del cervello si formano inibitori selettivi due - il blocco di entrambi i tipi di -Enzima zinco metallopeptidase - dell’enzima enkaphalinase con conseguente aumento della concentrazione di enkephaline i risultati di questi enzimi sono tali da costituire dati promettenti “farmaci inibitori” per lo sviluppo futuro di una nuova classe di analgesici che potrebbe essere di grande interesse nelle sindromi da dolore grave e persistente. (Roques e Noble, 1995; Le Guen et al, 2003;. Nobile e Roques, 2007) Alcuni AA sono fermamente convinti che, un giorno, una classe completamente nuova ed efficace di analgesici derivati dalla Bestatina (neuropeptidi) emergerà come terapia di prima scelta per diversi stati di malattie. A tal proposito alcuni analoghi del peptide per l’endomorphin-2, che realizza una analgesia senza effetti collaterali sono stati sintetizzati con successo (Fichna et al, 2005).. 1 2 3 così si ridurrebbero gli effetti collaterali indesiderati associati alla somministrazione di oppiacei, come la tolleranza etc. I recettori per gli oppioidi sono trasportati intra-assonali verso i peocessi neuronali, e si ritrovano in periferia nei terminali sensoriali nervosi periferici. Studi sulla co-localizzazione hanno confermato la presenza di recettori sulle fibre C- e A, mentre anche TPRV della variante V1 a livello di deprimere recettori per gli oppioidi viscerali e su neuroni esprimenti la isolectina B4, la SP e/o il Calcitonin-generelated peptide coesistente con il fenotipo 12003. I nn simpatici e le cellule immuinitarie possono anche loro esprimere recettori per gli oppiacei ma il loro ruolo nel controllo del dolore è poco chiaro, le affinità dei recettori periferici sono simili. Peripheral opioid receptors: a new therapeutic concept to target inflammation Christoph Stein 2003 Tutti 3 tipi di recettori per gli oppioidi mediano l’inibizione di correnti ad alto voltaggio in culture di nn afferenti primari. Questi effetti sono trasdotti da proteine-G (Gi o Go), in aggiunta gli oppioidi lavorano attraverso l’inibizione dell’adenil ciclase. Tutti e 3 I tipi di recettori oppioidei mediano l’inibizione di correnti calciche ad alto voltaggio nelle culture di recettori per gli oppiacei a livello di culture di neuroni afferenti (Mu). Questi effetti sono trasdotti da proteine da proteine G. (Gi and/or Go). Consistent with their effects on ion channels, opioids attenuate the excitability of peripheral nociceptor terminals, the propagation of action potentials, the release of excitatory proinflammatory neuropeptides (substance P, calcitonin gene related peptide) from peripheral sensory nerve endings, and vasodilatation evoked by stimulation of C-fibers. All of these mechanisms result in analgesia and/or antiinflammatory actions Peripheral opioid analgesic effects are augmented under conditions of tissue injury such as inflammation, neuropathy, or bone damage. One underlying mechanism is an increased number („upregulation“) of peripheral opioid receptors. In dorsal root ganglia, the synthesis and expression of opioid receptors can be increased by peripheral tissue inflammation. Subsequently, the axonal transport of opioid receptors is greatly enhanced (leading to their upregulation and to enhanced agonist efficacy at peripheral nerve terminals. In addition, the specific milieu (low pH, prostanoid release) of inflamed tissue can increase opioid agonist efficacy by enhanced Gprotein coupling and by increased neuronal cyclic adenosine monophosphate level Peripheral opioid analgesic effects are augmented under conditions of tissue injury such as inflammation, neuropathy, or bone damage. One underlying mechanism is an increased number („upregulation“) of peripheral opioid receptors. In dorsal root ganglia, the synthesis and expression of opioid receptors can be increased by peripheral tissue inflammation. Subsequently, the axonal transport of opioid receptors is greatly enhanced (leading to their upregulation and to enhanced agonist efficacy at peripheral nerve terminals. In addition, the specific milieu (low pH, prostanoid release) of inflamed tissue can increase opioid agonist efficacy by enhanced Gprotein coupling and by increased neuronal cyclic adenosine monophosphate level Of inflammation also leads to an increase in the number of sensory nerve terminals (“sprouting”) and disrupts the perineurial barrier, thus facilitating the access of opioid agonists to their receptors. Clinical studies have indicated that the perineural application of opioid agonists along uninjured nerves (e.g. axillary plexus) does not reliably produce analgesic effects, supporting the notion that inflammation promotes accessibility and/or efficient coupling of opioid receptors in primary afferent neurons The expression of immune-derived opioids is stimulated by viruses, endotoxins, cytokines, corticotropin releasing hormone (CRH) and adrenergic agonists. POMC mRNA, betaendorphin, met-enkephalin and dynorphin are found in circulating cells and lymph nodes in conditions of painful inflammation. These peptides are upregulated in lymphocytes, monocytes/macrophages and granulocytes within injured tissue. In patients undergoing knee surgery, opioid cells accumulate in the inflamed synovium and attenuate postoperative pain (Stein et al. 1993). Apparently, these immune-derived opioids do not induce cross-tolerance to locally administered morphine (Stein et al. 1996; Likar et Circulating opioid-containing leukocytes migrate to injured tissue directed by adhesion molecules and chemokines. In inflamed tissue, beta-endorphin-containing leukocytes coexpress L-selectin, and opioid cells, vascular Pselectin, ICAM-1 and PECAM-1 are simultaneously upregulated. Blocking selectins or ICAM-1 reduces the number of opioid cells and intrinsic analgesia. The release of opioids from immunocytes can be stimulated by environmental stress, sympathetic neuron-derived noradrenaline, interleukin-1beta (IL-1), CRH or chemokines (Binder et al. 2004; Rittner et al. 2005; 2006). This release is receptor-specific and calciumdependent, and it is mimicked by elevated extracellular potassium, consistent with a regulated secretory pathway, as in neurons and endocrine cells (Cabot et al. 1997; Mousa et al. 2004; Rittner et al. 2006). In vivo, the secreted opioid peptides bind to opioid receptors on sensory neurons and elicit analgesia within injured tissue (Stein et al. 1993; Schäfer et al. 1994; Schäfer et al. 1996). The efficacy of this pain inhibition is proportional to the number of opioid-producing immunocytes (Rittner et al. 2001). CRH-, IL-1 and stress-induced analgesia can be extinguished by immunosuppression (Stein et al. 1990; Schäfer et al. 1994), and by blocking the extravasation of opioid-containing leukocytes (Machelska et al. 1998, 2002). In In patients undergoing knee surgery, opioid cells accumulate in the inflamed synovium and attenuate postoperative pain (Stein et al. 1993). Apparently, these immune-derived opioids do not induce cross-tolerance to locally administered morphine (Stein et al. 1996; Likar et al. 2004). Preclinical Studies Preclinical Studies on Analgesic and Antiinflammatory Effects This basic research has stimulated the development of novel opioid ligands acting exclusively in the periphery without central sideeffects. A common approach is the use of hydrophilic compounds with minimal capability to cross the blood-brain-barrier. Among the first compounds were the mu-agonist loperamide (originally known as an antidiarrheal drug) and the kappa-agonist asimadoline. Peripheral restriction was also achieved with newly developed arylacetamide and peptidic kappaagonists (reviewed in Stein et al. 2003). While earlier attempts to demonstrate peripheral opioid analgesia in normal tissue failed, they were more successful in models of pathological pain (Stein 1993). In inflammation of the rat paw, the local injection of low, systemically inactive doses of mu-, delta- and kappa agonists produced analgesia that was dosedependent, stereospecific and reversible by selective antagonists. Some agonists produced both peripheral analgesic and antiinflammatory effects. Possible underlying mechanisms of the latter include a reduced release of proinflammatory neuropeptides or cytokines, and a diminished expression of adhesion molecules. Potent antinociception was also shown in models of nerve damage and of visceral, thermal and bone pain (reviewed in Stein et al. 2003). Clinical Studies on Analgesic and Antiinflammatory Effects Controlled studies have demonstrated significant analgesic effects following the local application of opioids at sites of injury. The intraarticular administration of the mu-agonist morphine is the best examined clinical application. After knee surgery, it dose-dependently reduces pain scores and/or supplemental analgesic consumption by a peripheral mechanism of action and without side-effects (reviewed in Kalso et al. 2002; Stein et al. 2003). Intraarticular morphine is active in the presence of opioid containing inflammatory cells (Stein et al. 1996; Likar et al. 2004) and in chronic rheumatoid and osteoarthritis (Stein et al. 1999). Its effect is similar to a standard intraarticular local anesthetic or steroid injection and is long lasting (up to 7 days), possibly due to morphine’s anti-inflammatory activity. Other trials showed efficacy of local opioid injections in bone pain, dental pain, corneal abrasions and visceral pain. Several studies found no peripheral effects of opioids. The majority of those trials examined the injection of agonists into the noninflamed environment along nerve trunks. This suggests that intraaxonal opioid receptors may be „in transit“, and not available as functional receptors at the membrane. Novel peripherally restricted opioids have recently entered human trials, including a kappaagonist that markedly reduced visceral pain in patients with chronic pancreatitis without severe side effects. . Beyond the absence of central side-effects, such novel compounds may offer advantages such as anti-inflammatory effects, lack of tolerance, lack of constipation, lack of gastrointestinal, hepatic, renal and thromboembolic complications (typically associated with nonsteroidal anti-inflammatory drugs), and efficacy in neuropathic pain (Stein et al. 2003). .. .. .. .. .. .. .. ..
Scaricare