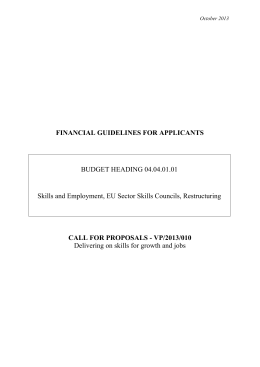
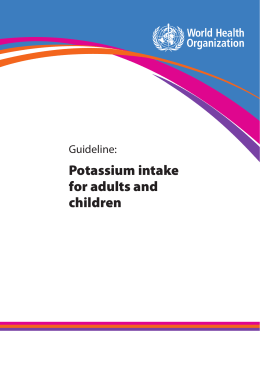
Clinical Nephrology, Vol. 75 – No. 3/2011 (218-225) Assessment of habitual physical activity and energy expenditure in dialysis patients and relationships to nutritional parameters Original ©2011 Dustri-Verlag Dr. K. Feistle ISSN 0301-0430 DOI 10.5414/CNP75218 A. Cupisti1, A. Capitanini2, G. Betti3, C. D’Alessandro1 and G. Barsotti1 1Division of Nephrology, Department of Internal Medicine, University of Pisa, Pisa, and Dialysis, Pescia Hospital, Pescia, and 3Nephrology and Dialysis, Massa-Carrara Hospital, Massa-Carrara, Italy 2Nephrology Physical activity in dialysis patients Key words physical activity – energy expenditure – dialysis – nutrition parameters – exercise – CKD Received May 10, 2010; accepted in revised from July 6, 2010 Correspondence to A. Cupisti, MD, PhD Division of Nephrology, Department of Internal Medicine, University of Pisa, Via Roma 67, 56126 Pisa, Italy [email protected] Abstract. Background and aim: Assessment of physical activity level and of energy expenditure is important in the clinical and nutritional care of dialysis patients, but it is not so easy to accomplish. The SenseWear™ Armband (SWA) is a novel multisensory device that is worn on the upper arm and collects a variety of physiologic data related to physical activity. Thus, duration and intensity of physical activity is recorded and expressed as METs (Metabolic Equivalent Task), and energy expenditure is estimated. The aim of our study was to assess interdialytic spontaneous physical activity in stable chronic hemodialysis (HD) patients and the relation to nutritional status and dietary nutrient intake. Patients and methods: In 50 stable patients on maintenance hemodialysis treatment and 33 normal subjects (control group), level of spontaneous physical activity and estimated daily energy expenditure was assessed by SWA and related to biochemistry and anthropometry data, bioelectric impedance vector analysis, and energy and nutrient intake information coming from a 3-day food recall. Results: In respect to controls, HD patients showed lower mean daily METs value (1.3 ± 0.3 vs. 1.5 ± 0.2, p < 0.01), a lower time spent on activities > 3 METs (89 ± 85 vs. 143 ± 104 min/day, p < 0.05), lower number of steps per day (5,584 ± 3,734 vs. 11,735 ± 5,130, p < 0.001), resulting in a lower estimated energy expenditure (2,190 ± 629 vs. 2,462 ± 443 Kcal/day, p < 0.05). 31 out of the 50 HD patients (62%) had a mean daily value < 1.4 METs and hence were defined as sedentary. They differed from the active patients for higher age (63 ± 12 vs. 54 ± 12 y, p < 0.01), lower energy intake (26.1 ± 6.4 vs. 32.4 ± 11.3 Kcal/day, p < 0.05) and lower phase angle (5.5 ± 1.0 vs. 6.3 ± 0.9, p < 0.05). SWAbased estimation of daily energy expenditure was negatively related to age (r = –0.31, p < 0.05), whereas positive relations were observed with BMI (r = 0.51, p < 0.001), phase angle (r = 0.40, p < 0.01), serum phosphate (r = 0.49, p < 0.001) and albumin (r = 0.41, p < 0.01). The mean daily METs values were strongly related to normalized energy intake (r = 0.47, p < 0.001) and also to protein intake (r = 0.33, p < 0.05) and to phase angle (r = 0.38, p < 0.01). Multiple regression analysis showed that energy intake and dietary protein intake were independently related to the intensity of physical activity. Conclusion: Our findings indicate that poor physical activity is highly prevalent in stable dialysis patients even when free from physical or neurological disabilities or severe comorbid conditions. The level and intensity of physical activity is positively related to body composition and to dietary nutrient intake. This confirms the strong interrelationship between exercise and nutrition, which in turn are associated with survival, rehabilitation and quality of life in dialysis patients. Introduction Previous studies have reported that the limits of physical capability are largely reduced in hemodialysis (HD) patients when compared with healthy subjects [1, 2, 3]. Dialysis patients may suffer from cardiovascular disease, diabetes, malnutrition, and depression, which limit their exercise capacity. Nevertheless, evidence exists that maintenance of regular physical exercise may favor rehabilitation of patients and correction of several cardiovascular, metabolic and nutritional abnormalities. Data from the literature suggest that inactivity is associated with increased mortality risk [4, 5, 6], whereas physical exercise is related to quality of life and nutrition [7, 8, 9, 10]. Namely, regular physical activity may ameliorate appetite and 219 Physical activity in dialysis patients maintain muscle mass. In turn, adequate energy and protein intake are mandatory for physical performance and good nutritional status. Several epidemiological studies showed that protein and energy intake in dialysis patients is largely lower than recommended [11, 12]. The minimum energy requirement should be no less than the total energy expenditure that is due to resting energy expenditure (60 – 75%) plus energy consumed during physical activity (25 – 40%). Therefore, evaluation of physical activity is important to assess nutritional requirements. This indicates that it would be valuable to determine rest energy expenditure as well as the type, quantity and intensity of physical activity in order to plan personalized dietary and rehabilitation programs and to test the efficacy of specific interventions in HD patients. Physical activity records and questionnaires provide a single, convenient, low-cost estimation of physical activity and/or energy expenditure, but they are quite subjective and not very reliable methods [13, 14, 15]. More reliable quantification of spontaneous physical activity can be obtained by tri-axial accelerometers, that is, electronic devices worn on the waist to detect movements in three planes of motion, namely mediolateral, anteroposterior, and vertical. Electric transducers and microprocessors detect accelerations and convert them into digital signals [2, 16]. The SenseWear™ Armband is a multisensory device including a two-axis accelerometer, heat flux sensor, skin temperature sensor, near-body ambient temperature sensor, and galvanic skin response sensor. It is worn on the upper arm and collects a variety of physiologic data related to physical activity. Duration and intensity of physical activity are recorded and daily energy expenditure is estimated by software based on a proprietary algorithm [17]. This multiple sensor array was designed to overcome the limitations of other objective or subjective energy expenditure assessment tools [18], and it has been validated and used in a number of physiological and pathological conditions [19, 20, 21, 22]. The aim of our study was to assess interdialytic spontaneous physical activity by SWA in stable chronic hemodialysis (HD) patients and the relation to nutritional status and dietary nutrient intake. Patients and methods Patients 50 stable patients (32 male, 18 female; aged 59 ± 13 y) on maintenance HD treatment (time on dialysis 89 ± 78 months), who had no major skeletal, muscular or neurological disabilities, or had not reported severe impairment with walking, were qualified for enrollment in the study. Patients with severe cardiac failure (Stage IV NYHA), or respiratory insufficiency, cancer, dementia, psychiatric or neurologic diseases, and inflammatory systemic diseases were excluded. Hospitalization within the last three months, therapies with steroids and/or immunosuppressive drugs were also considered as exclusion criteria. The underlying renal diseases were chronic glomerulonephritis in 13 cases, diabetic nephropathy in 6 cases, vascular nephropathy in 10 cases, polycystic kidney disease in 8 cases, chronic interstitial nephropathy in 5 and unknown in 8 cases. All the patients were on a thrice-weekly HD treatment, for 210 – 240 minutes; 23 patients were on on-line hemodiafiltration, 19 patients on standard bicarbonate dialysis and 8 patients on acetate-free biofiltration. In all the cases synthetic and highly biocompatible membranes were used (low-flux and high flux polysulphone, AN69, polyammide). Vascular access was native arteriovenous fistula in 41 cases, arteriovenous graft in 6 cases and permanent central vein catheter in 3 cases. 33 normal subjects, comparable for age, sex and body mass index, served as controls. All patients gave their informed consent to the study that was approved by the Ethics Committee of the Pisa University Hospital. Physical activity and energy expenditure assessment The level of physical activity and estimated daily total energy expenditure (TEE) under free-living conditions were assessed by SenseWear™ Armband (SWA, BodyMedia, Pittsburgh, PA, USA). This device is worn on the upper arm (the nondominant one or that is free from arteriovenous fistula or graft) over the triceps muscle, in the middle tract be- 220 Cupisti, Capitanini, Betti et al. tween acromion and olecranon processes. Subjects were instructed to maintain their usual daily life habits while wearing the monitor and to remove it only for showers or water activities. The SWA device collects a variety of physiologic data through multiple sensors (a two-axis accelerometer, heat flux sensor, skin temperature sensor, near-body ambient temperature sensor, and galvanic skin response sensor) that are uploaded and analyzed using software (InnerView™ Research Software, Version 6.1). This multichannel approach, which integrates information from a biaxial accelerometer and heat-related sensors, has shown to provide additional information that cannot be obtained solely from movement sensors and it has high sensitivity in detecting even small changes in energy expenditure associated with complex activities. The SWA reports actual wear time, avoiding the considerable challenge in determining whether a monitor was worn or not. These features provide several advantages over traditional uniaxial accelerometers for assessing physical activity. The validity of total energy expenditure (TEE) estimates from the SWA has been supported in studies using both indirect calorimetry and doubly labeled water [22]. The SWA has been validated both under laboratory conditions and under free living conditions, and it has potential advantages in accuracy when compared with traditional accelerometrybased monitors [17, 18, 19, 20, 21]. One of the easiest ways for quantifying the intensity of a physical activity is the Metabolic Equivalent Task (MET) method. Kilocalories and metabolic equivalent are converted using the following equation: MET = Kcal/h/Kg b.w. One MET is the energy expended at rest. Thus, two METs indicate twice the energy expended at rest, three METs triple the resting energy expenditure, and so on. For example, such activities as reading, listening to music, and knitting correspond approximately to 1.0 – 1.5 METs. Walking slowly corresponds to 1.5 – 2 METs; walking at 3 km/h or cycling at 8 km/h correspond to 2 – 3 METs; playing volleyball, cycling at 10 km/h, and household cleaning correspond to 3 – 4 METs; walking at 6 km/h, cycling at 16 km/h, skating at 15 km/h, or digging correspond approximately to 5 – 6 METs. Measurements were carried out during a mid-week interdialytic period of 48 h and included number of steps and minutes spent in physical activity with an intensity > 3 MET/min, between 6 and 9 MET/min, or > 9 MET/min. Mean daily METs values may be considered as a measure of the mean daily activity level; for example, a daily average value < 1.4 METs defines a sedentary patient, whereas average values > 1.6 METs are associated with an active life style. Total energy expenditure (reported as 24 h average value) was evaluated by a proprietary algorithm using information of movement, skin temperature, heat flow, near-body temperature and galvanic skin response, together with data about age, height, weight and gender. Total energy expenditure was also evaluated using a prediction equation, consisting of an estimation of resting energy expenditure multiplied by an activity factor. Namely, resting energy expenditure was calculated using the Harris-Benedict formula and the activity factor varied from 1.2 for minimal physical activity, up to 1.5 for moderate but significant physical activity and up to 1.8 for high physical activity [23]. Nutritional assessment Nutritional parameters included biochemistry, bioelectric impedance vector analysis (BIVA), height, and body weight before and after dialysis. Body mass index (BMI) was calculated as follows: post-dialysis body weight (kg)/height2 (m2). Predialysis biochemical determinations included serum albumin, C reactive protein, phosphorus, calcium, and hematocrit. Serum albumin was measured by the nephelometric method. Decreased albumin levels can be suggestive of protein malnutrition and/or inflammation [24] and represent an unfavorable prognostic sign. Serum urea level was determined before and after dialysis treatment to calculate a single pool Kt/V. BIVA was performed at the end of the hemodialysis session with a bioelectrical impedance analyzer (BIA/STA, Akern, Florence, Italy) with a distal, tetrapolar technique, delivering an excitation current at 50 kHz [25]. BIVA parameters were measured in du- 221 Physical activity in dialysis patients plicate. BIVA gives two bioelectric parameters: body resistance (R) and reactance (Xc), and the impedance vector (Z) is a combination of R and Xc across tissues. The arc tangent of Xc/R is called phase angle (PA), which is a derived measure obtained from the relation between the direct measures of resistance and reactance reflecting hydration status and soft tissue cellular mass. Reduced phase angle reflects increased extra- to intracellular water ratio as well as a decrease in body cell mass; it is a predictor of survival in a number of diseases and also in the dialysis population, where phase angle values lower than 4.0° are associated with increased mortality risk [26]. A BIVA-derived parameter with prognostic value is also the body cell mass index (BCMI): values < 8.0 kg/m2 are associated with unfavorable prognosis. Dietary nutrient intake assessment All the subjects were seen individually by registered dieticians to collect a 3-day food record for energy and nutrient intake assessment. The 3-day recalls were collected by interviews during which the subjects were provided with a color photo atlas of common foods and their servings in order to help them in estimating the real amounts of consumed food. The 3-day dietary recall included a dialysis day, a weekend day and a nondialysis day as suggested by recent guidelines [23, 27]. Dietary composition was assessed with a computerized diet software (MetaDieta®, Meteda, AP, Italy). Total energy and nutrient intakes and their distribution among meals were examined. The daily intake for each studied nutrient was calculated as the average of the 3-day food records. Daily energy requirement was estimated by calculation of daily energy expenditure, by Harris-Benedict equation multiplied by an activity factor, according to EBPG guideline on Nutrition [23]. Statistical analysis A statistical package, StatView 5 release 5.0.1 for personal computer, was used for processing data. Descriptive statistics are given as mean ± standard deviation. Statistical analysis was performed by Student’s t-test for unpaired data. Linear correlation analysis was performed by Pearson’s test. Stepwise multiple correlation analysis was used to study all the significant relationships with physical activity and energy expenditure. Differences were considered to be statistically significant when p < 0.05. Results Patients and controls did not differ as far as body weight (71 ± 17 vs. 69 ± 13 kg), BMI (24.8 ± 4.6 vs. 24.5 ± 3.3 kg/m2), and phase angle (5.79 ± 1.04 vs. 5.74 ± 0.85°) were concerned. In comparison with controls, HD patients showed lower daily average METs value (1.3 ± 0.3 vs. 1.5 ± 0.2, p < 0.01), a lower time spent on activities > 3 METs (89 ± 85 vs. 143 ± 104 min/d, p < 0.05), lower number of steps per day (5,584 ± 3,734 vs. 11,735 ± 5,130, p < 0.001), resulting in a lower estimated total energy expenditure (2,190 ± 629 vs. 2,462 ± 443 kcal/d, p < 0.05). In HD patients, a trend to a lower energy expenditure, calculated by SWA, was observed in dialysis days compared to nondialysis days (2,145 ± 558 vs. 2,388 ± 708 kcal/d, p = 0.07, respectively). Dietary protein intake was significantly lower in the HD patients than in control subjects (68.0 ± 18.2 vs. 81.5 ± 29.7 g/d, 1.01 ± 0.35 vs. 1.24 ± 0.32 g/kg/d, p < 0.05), whereas total energy intake were more similar (2,214 ± 618 vs. 2,462 ± 443 kcal/d, 28.5 ± 9.0 vs. 30.6 ± 5.8 kcal/kg/d, respectively). BIVA analysis showed similar phase angle values in patients and controls (5.8 ± 1.0 vs. 5.7 ± 0.8°), but BCMI was lower in HD patients (8.5 ± 2.0 vs. 9.5 ± 2.0 kg/m2, p < 0.05). Twelve of the 50 studied HD patients showed daily mean values of energy expenditure between 1.4 and 1.6 METs, and 7 patients over 1.6 METs; of consequence, 31 out of the 50 studied patients (62%) had a mean daily value < 1.4 METs, and thus they were defined as sedentary. The prevalence of a sedentary condition was significantly lower in the control group (18%, p < 0.01). Table 1 shows some clinical data of the sedentary and non-sedentary dialysis patients. Data about physical activity parameters derived by SWA elaboration analysis in the two groups are reported in Table 2. 222 Cupisti, Capitanini, Betti et al. Table 1. Clinical and biochemical data of the study subjects, divided by sedentary (< 1.4 METs) and active (³ 1.4 METs). Active n = 19 Sedentary n = 31 p Age, y 53.6 ± 11.8 63.3 ± 12.5 < 0.010 Dialysis age, months 123 ± 105 68 ± 48 < 0.02 Kt/V 1.4 ± 0.2 1.4 ± 0.2 ns 23.8 ± 4.0 25.4 ± 4.9 ns Phase angle, ° 6.3 ± 0.9 5.5 ± 1.0 < 0.01 S. Albumin, g/dl 3.9 ± 0.3 3.9 ± 0.4 ns nPNA, g/kg/d 1.16 ± 0.23 1.06 ± 0.24 ns Hemoglobin, g/dl 12.0 ± 1.6 12.0 ± 1.3 ns Hematocrit, % 37.3 ± 4.5 37.1 ± 4.1 ns 0.5 ± 0.6 0.5 ± 0.4 ns ns BMI, kg/m2 CRP, mg/dl 319 ± 289 267 ± 209 Ca ´P, mg2/dl2 49.4 ± 12.3 43,5 ± 12,5 HCO3–, mmol/l 19.6 ± 2.1 20.9 ± 1.8 = 0.03 EPO dose, IU/w 7210 ± 9420 7621 ± 7984 ns EPO res I 10.5 ± 13.9 9.1 ± 8.8 ns Table 2. Data from Sense-Wear Arm-band (SWA), and comparison of Total Energy Expenditure (TEE) with data from prediction equation and dietary recalls. Active n = 19 Sedentary n = 31 p-value 1.7 ± 0.2 1.1 ± 0.1 < 0.001 165 ± 80 34 ± 26 < 0.001 Data from SWA Time on 3 – 6 METs, min/d Time on > 6 METs, min/d 10 ± 10 0±0 < 0.001 8681 ± 3833 3173 ± 1890 < 0.001 Activity energy expenditure, kcal /d 799 ± 490 135 ± 132 < 0.001 SWA TEE, kcal/kg/d 35.0 ± 6.4 29.1 ± 6.0 0.002 32.4 ± 3.5 32.3 ± 5.2 ns Dietary energy intake, kcal/kg/d 32.4 ± 7.3 26.1 ± 6.4 < 0.05 Dietary protein intake, g/kg/d 1.04 ± 0.36 0.93 ± 0.25 ns Steps, n./d Data from prediction equation Equation TEE, kcal/kg/d Using the SWA-derived calculations, daily TEE negatively correlated with age (r = –0.33, p < 0.05), whereas positive correlations were observed with BMI (r = 0.51, p < 0.001), phase angle (r = 0.404, p < 0.01) phosphate (r = 0.49, p < 0.001), serum PTH (r = 0.32, p < 0.05) and albumin (r = 0.38, p < 0.01). In addition, significant correlations were also found between daily total energy expenditure and energy intake (r = 0.37, p < 0.01) and in particular with complex carbohydrates dietary intake (r = 0.48, p < 0.001). Similarly, the mean daily METs values were directly related to normalized protein (r = 0.36, p < 0.01) and energy intake (r = 0.42, p < 0.01) (Figure 1). iPTH, pg/ml METs, 24 h mean 5 patients were able to perform a physical activity over 6 METs beyond 5 minutes. Data from dietary recalls Evaluating the duration and intensity of physical activity, we observed that 11 patients had a physical expenditure greater than 3 METs for 30 – 60 minutes, 8 patients for 60 – 120 minutes and 15 patients for over 120 minutes, while 16 patients spent fewer than 30 minutes on 3 METs activities. Finally, only In our series, the minutes spent on a physical activity over 3 METs correlated positively with dialysis vintage (r = 0.41, p < 0.01), phase angle (r = 0.36, p < 0.01) and BCMI (r = 0.41, p < 0,01), and also to normalized energy (r = 0.51, p < 0.001) (Figure 2) and protein (r = 0.37, p < 0.01) dietary intake. No relationship was observed between parameters of physical activity and CRP, Kt/V, hemoglobin or hematocrit. Multiple regression analysis showed that energy intake and dietary protein intake were independently related to TEE evaluated by SWA and to the time of mild to moderate physical activity. As a whole, the estimated daily energy expenditure was similar when using SWA or the prediction equation (31.4 ± 7.2 vs. 32.4 ± 4.7 kcal/Kg/b.w., respectively). However, differences exist where sedentary or active dialysis patients are concerned. Table 2 shows that when using SWA, as expected, sedentary patients had a lower energy expenditure than non-sedentary patients; however, no difference resulted when using the prediction equation. The conclusion is that daily energy expenditure estimated by the prediction equation is higher than that recorded by SWA in sedentary patients, while a trend to underestimate occurs in active patients (Table 2). The analysis of 3-day dietary recalls showed that sedentary ate less than active patients (Table 2), and as a whole, reported energy intake is lower than estimated energy expenditure by SWA and also by the predic- Physical activity in dialysis patients Figure 1. Relationship between mean daily METs values (as a measure of the mean daily activity level) and the dietary energy intake in the hemodialysis studied patients. Figure 2. Relationship between minutes spent at physical activity > 3 METs (as a measure of intensity of physical performance) and the dietary energy intake in the hemodialysis studied patients. tion equation, both in patients and in controls (Table 2). Discussion The results of the study indicate that the level of exercise is quite low in dialysis patients and that it is related to age, body composition and dietary nutrient intake. They confirm that levels of physical activity were associated with phase angle [2], as an indicator of body composition and nutritional intake [32] among patients with ESRD and that 223 these patients were less active than sedentary controls. These similar conclusions were obtained using different methods for both physical activity measurement (namely SWA or tri-axis accelerometers) and dietary nutrient intake assessment (3-day food recall or food frequency questionnaires). In addition, we also observed an association between phase angle and minutes spent in activities greater than 3 METs, that is, with the intensity of the physical exercise The level of habitual physical activity measured with a simple method, SWA, in stable HD patients is directly correlated with phase angle and BCMI, which are markers of nutritional status and predictors of survival in dialysis patients. Namely, the lower the physical activity, the lower the phase angle, energy intake and protein intake. Implementation of regular physical activity is important to ameliorate quality of life, rehabilitation and even survival [28, 29], but exercise capacity in chronic HD patients is generally reduced because of the high prevalence of physical disabilities, social and psychological problems, and relevant comorbid conditions. Physical exercise is not for everyone, but it requires individual prescription. Dialysis staff commitment is important for the safety and success of physical activity programs, whereas dedicated exercise professionals may be needed depending on the type of the exercise training [30]. Assessment of habitual activity is not easy. Baecke self-administered habitual physical activity questionnaire or the Five-City Project 7-day recall physical activity questionnaire can be used, but they give only indirect measurements and are highly dependent on a patient’s mental skill and collaboration. Pedometers are very useful devices, but they count steps in a similar way during walking or running and, therefore, they do not give any information about the timing and intensity of physical activity. In addition, pedometers may not record physical activity in types of exercise different from walking or running, and so estimation of energy expenditure is far from accurate. Meanwhile, several studies have shown that SWA can give an accurate assessment of daily physical activity in general population [13]. This method is simple, noninvasive and low-cost. The major advantage of using SWA 224 Cupisti, Capitanini, Betti et al. in ambulatory settings is that it can record spontaneous physical activity for long periods of time and so evaluate daily energy expenditure, the timing, duration and intensity of physical exercise, and time spent during resting and sleeping. Our experience confirms that the SWA was user-friendly in terms of easy attachment/detachment, minimal discomfort, and little or no interference in daily life activities. Although the use of SWA has been validated in healthy individuals or athletes, there are not enough data to establish the reference values for SWA-determined physical activity in different groups of chronically ill patients. Phase angle was the only nutritional parameter that showed direct relationship with physical activity parameters, such as the daily mean METs values, the minutes spent in activities > 3 METs, or the daily TEE. It means that lower phase angle values, which are associated with higher mortality rate in dialysis patients, are associated with a sedentary condition, and poor physical performance capacity. Moreover, low physical activity is also associated with low energy and protein intake and contributes to decreased muscle tone and mass; in other words, poor physical activity is strongly associated with malnutrition and to changes predictive of poor prognosis. On the other hand, good physical activity increases lean body mass, increases food intake and contributes to the maintenance of good nutritional status. It may ameliorate a patient’s prognosis, quality of life, and rehabilitation. It must be underlined that our series included stable HD patients, without pathologies preventing them from performing physical activity. Hemoglobin levels reached target levels in most of the patients, so no relationship was expected with physical activity parameters. Similarly, no relationship was observed with dialysis dose and with inflammation markers as already reported in the literature [31, 32]. Spontaneous physical activity tended to be lower on dialysis days. This was already observed by Majchrzak et al. using a tri-axial accelerometer: physical activity was lower on dialysis days when compared with nondialysis days, and this decrease was attributed to the lack of movements during the 4-hour HD procedure [16]. Information from the 3-day recall indicated that daily energy intake was lower than total energy expenditure estimated by SWA in both in patients and controls (Table 2). This probably reflects the tendency to underestimation of the food dietary recall method. Obviously there could be a potential underestimation of energy and nutrients intake through dietary interviews, which could represent a limitation of this kind of investigation. Even if the food record analysis represents the most valid and simple tool for nutrient and calorie estimation, the occurrence of a conscious or unconscious underreporting is largely known and recently confirmed in healthy adults [33] as well as in renal failure patients [34, 35]. Furthermore, dietary intake may differ among a dialysis day, a weekend day and a nondialysis day. This is the reason we used the average values of these 3 days, according to Kidney Disease Outcomes Quality Initiative (K/DOQI) Recommendation for Nutritional Management [23, 27]. This method provides a closer insight into dietary habits, and it is preferred by patients who do not always comply with accurate recordings for a longer period. In conclusion, our findings indicate that poor physical activity is highly prevalent in dialysis patients even when free from physical or neurological disabilities or severe comorbid conditions. The level and intensity of physical activity is positively related to body composition and to dietary nutrient intake. This confirms the strong interrelationship between exercise and nutrition, which in turn are associated with survival, rehabilitation and quality of life of dialysis patients. References [1] [2] [3] [4] Gutman RA, Stead WW, Robinson RR. Physical activity and employment status of patients on maintenance dialysis. N Engl J Med. 1981; 304: 309-313. Johansen KL, Chertow GM, Ng AV et al. Physical activity levels in patients on hemodialysis and healthy sedentary controls. Kidney Int. 2000; 57: 2564-2570. Johansen KL. Exercise in the end-stage renal disease population. J Am Soc Nephrol. 2007; 18: 1845-1854. Elder SE, Bommer J, Fissell RB et al. Hemodialysis facilities in which more patients exercise have lower risks of mortality and hospitalization: international results from the DOPPS. J Am Soc Nephrol. 2005; 16: 94. Physical activity in dialysis patients [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] O’Hare AM, Tawney K, Bacchetti P, Johansen KL. Decreased survival among sedentary patients undergoing dialysis: results from the Dialysis Morbidity and Mortality Study Wave 2. Am J Kidney Dis. 2003; 41: 447-454. Sietsema KE, Amato A, Adler SG, Brass EP. Exercise capacity as a predictor of survival among ambulatory patients with end-stage renal disease. Kidney Int. 2004; 65: 719-724. Capitanini A, Cupisti A, Mochi N, Rossini D, Lupi A, Michelotti G, Rossi A. Effects of exercise training on exercise aerobic capacity and quality of life in hemodialysis patients. J Nephrol. 2008; 21: 738-743. Levendoglu F, Altintepe N, Okudan N, Ugurlu H, Gokbel H, Tonbul Z, Guney I, Turk S. A twelve week exercise program improves the psychological status, quality of life and work capacity in hemodialysis patients. J Nephrol. 2004; 17: 826832. Painter P, Moore G, Carlson L, Paul S, Myll J, Phillips W, Haskell W. Effects of exercise training plus normalization of hematocrit on exercise capacity and health-related quality of life. Am J Kidney Dis. 2002; 39: 257-265. Suh MR, Jung HH, Kim SB, Park JS, Yang WS. Effects of regular exercise on anxiety, depression and quality of life in maintenance hemodialysis patients. Ren Fail. 2002; 24: 337-345. Kalantar-Zadeh K, Kopple JD, Deepak S et al. Food intake characteristics of hemodialysis patients as obtained by Food Frequency Questionnaire. J Ren Nutr. 2002; 12: 17-31. Cupisti A, D’Alessandro C, Valeri A, Capitanini A, Meola M, Betti G, Barsotti G. Food intake and nutritional status in stable hemodialysis patients. Ren Fail. 2010; 32: 47-54. Leenders N Y, Sherman WM, Nagaraja HN, Kien CL. Evaluation of methods to assess physical activity in freeliving conditions. Med Sci Sports Exerc. 2001; 33: 1233-1240. Bassett DR Jr, Cureton AL, Ainsworth BE. Measurement of daily walking distance-questionnaire versus pedometer. Med Sci Sports Exerc. 2000; 32: 1018-1023. Conway JM, Seale JL, Jacob DR, Irwin ML, Ainsworth BE. Comparison of energy expenditure estimates from doubly labeled water, a physical activity questionnaire, and physical activity records. Am J Clin Nutr. 2002; 75: 519-525. Majchrzak KM, Pupim LB, Chen K, Martin CJ, Gaffney S, Greene JH, Ikizler TA. Physical activity patterns in chronic hemodialysis patients: comparison of dialysis and nondialysis days. J Ren Nutr. 2005; 15: 217-224. Fruin ML, Rankin JW. Validity of a multi-sensor armband in estimating rest and exercise energy expenditure. Med Sci Sports Exerc. 2004; 36: 1063-1069. Mafra D, Deleaval P, Teta D et al. New measurements of energy expenditure and physical activity in chronic kidney disease. J Ren Nutr. 2009; 19: 16-19. Jakicic JM, Marcus M, Gallagher KI et al. Evaluation of the SenseWear Pro Armband to assess energy expenditure during exercise. Med Sci Sports Exerc. 2004; 36: 897-904. 225 [20] Mignault D, St Onge M, Karelis AD, Allison DB, Rabasa-Lhoret R. Evaluation of the portable Health Wear Armband. Diabetes Care. 2005; 28: 225-227. [21] St Onge M, Mignault D, Allison DB, RabasaLhoret R. Evaluation of a portable device to measure daily energy expenditure in free-living adults. Am J Clin Nutr. 2007; 85: 742-749. [22] Johannsen DL, Calabro MA, Steward J, Franke W, Rood JC, Welk GJ. Accuracy of armband monitors for measuring daily energy expenditure in healthy adults. Med Sci Sport Exerc. 2010. doi: 10.1249/ MSS.0b013e3181e0b3ff. [23] Fouque D, Vennegoor M, Ter Wee P et al. EBPG Guideline on Nutrition. Nephrol Dial Transplant. 2007; 22 (Suppl): S45-S87. [24] Mitch WE. Malnutrition: a frequent misdiagnosis for hemodialysis patients. J Clin Invest. 2002; 110: 437-439. [25] Piccoli A, Rossi B, Pillon L et al. A new method for monitoring body fluid variation by bioimpedance analysis: The RXc graph. Kidney Int. 1994; 46: 534-539. [26] Chertow GM, Jacobs DO, Lazarus JM et al. Phase angle predicts survival in hemodialysis patients. J Ren Nutr. 1997; 7: 204-207. [27] Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis 2000; 35: 1-140 [28] Tentori F. Focus on: Physical exercise in hemodialysis patients. J Nephrol. 2008; 21: 808-812. [29] Krause R. WGRR-European Working group on renal rehabilitation and exercise physiology. Nephrologists view on exercise training in chronic kidney disease. Clin Nephrol. 2004; 61: 2-4. [30] Bennett PN, Breugelmans L, Barnard R, Agius M, Chan D, Fraser D, McNeill L, Potter L. Sustaining a hemodialysis exercise program: a review. Semin Dial. 2010; 23: 62-73. [31] Zamojska S, Szklarek M, Niewodniczy M, Nowicki M. Correlates of habitual physical activity in chronic haemodialysis patients. Nephrol Dial Transplant. 2006; 21: 1323-1327. [32] Hung AM, Chertow GM, Young BS, Carey S, Johansen KL. Inflammatory markers are unrelated to physical activity, performance and functioning in haemodialysis. Adv Ren Replac Ther 2003; 10: 232-240. [33] Slimani N, Bingham S, Runswick S et al. Group level validation of protein intakes estimated by 24-hour diet recall and dietary questionnaires against 24-hour urinary nitrogen in the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study. Cancer Epidemiol Biomarkers Prev. 2003; 12: 784-795. [34] Avesani CM, Kamimura MA, Draibe SA et al. Is Energy intake underestimated in nondialyzed chronic renal disease patients? J Ren Nutr 2005; 15: 159-165. [35] Kloppenburg WD, de Jong PE, Huisman RM. The contradiction of stable body mass despite low reported dietary energy intake in chronic hemodialysis patients. Nephrol Dial Transplant 2002; 17: 1628-1633.
Scaricare