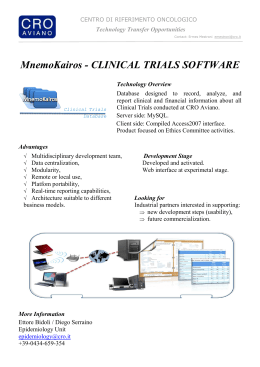
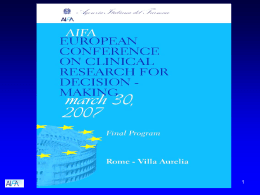
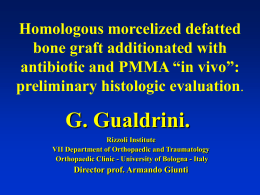
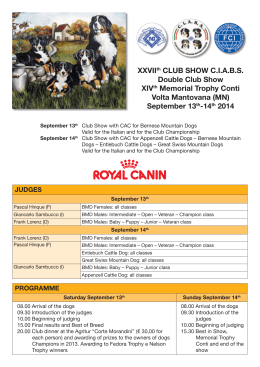
Is There Enough Evidence to Use Bisphosphonates in HIV-Infected Patients? A Systematic Review and Meta-analysis Marilia Rita Pinzone1, Santiago Moreno2, Bruno Cacopardo1 and Giuseppe Nunnari1 1Department of Clinical and Molecular Biomedicine, Division of Infectious Diseases, University of Catania, Catania, Italy; 2Department of Infectious Diseases, Institute for Health Research (IRICYS), University Hospital Ramón y Cajal, Madrid, Spain Abstract An increased prevalence of osteopenia and osteoporosis has been observed in HIV-infected cohorts. We investigated the effect of bisphosphonates on bone mineral density in adults with HIV infection. Outcomes of interest were bone mineral density changes measured by dual-energy X-ray absorptiometry at the lumbar spine, femoral neck, and total hip, and adverse events. Data were pooled using the fixed-effects model. We identified eight randomized controlled trials meeting our inclusion criteria, involving 328 participants. Five trials compared alendronate with placebo or no intervention; in three trials the intervention arm received zoledronate. A significant increase in bone mineral density at the lumbar spine was observed in the bisphosphonate group at 48 weeks (MD: 2.84%; 95% CI: 2.11-3.57) and 96 weeks (MD: 6.76%; 95% CI: 4.98-8.54); analogously, bisphosphonates were associated with an increase in total hip bone mineral density at 48 weeks (MD: 2.12%; 95% CI: 1.43-2.81) and 96 weeks (MD: 3.2%; 95% CI: 1.52-4.88). Bisphosphonates were generally well tolerated; no drug-related withdrawals were reported in the five randomized controlled trials assessing alendronate, whereas two patients out of 104 receiving zoledronate experienced acute-phase reactions. In conclusion, administration of oral and intravenous bisphosphonates was associated with increased bone mineral density at the lumbar spine and total hip over two years in HIV-positive patients. However, none of the included trials were long enough to detect the impact of bisphosphonates on a clinically important outcome such as fracture risk. Larger studies with extended follow-up are warranted. (AIDS Rev. 2014;16:213-22) Corresponding author: Giuseppe Nunnari, [email protected] Key words Alendronate. Bisphosphonate. HAART. HIV. Osteoporosis. Zoledronate. Introduction The natural history of HIV infection has been dramatically changed by the introduction of HAART. Most patients taking HAART experience durable control of Giuseppe Nunnari Department of Clinical and Molecular Biomedicine Division of Infectious Diseases ARNAS Garibaldi Nesima, University of Catania Via Palermo 636, 95125 Catania, Italy E-mail: [email protected] HIV replication, so that the incidence of AIDS-related events has significantly declined1. However, a concomitant increase in the morbidity and mortality attributable to noninfectious complications, such as malignancies, cardiovascular, renal, and bone disease, has been observed2-5. Osteoporosis is a skeletal disorder characterized by micro-architectural abnormalities and reduced bone mineral density (BMD), which results in increased fracture risk6. Osteopenia refers to a milder degree of bone demineralization. The BMD is usually measured using dualenergy X-ray absorptiometry (DXA) and expressed as standard deviations from the population mean, either as a z-score (compared to age- and sex-matched data) © Permanyer Publications 2014 Marilia Rita Pinzone, et al.: Bisphosphonates for Increasing BMD in HIV No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. AIDS Rev. 2014;16:213-22 213 214 Search strategy, assessment of risk of bias, and statistical methods We did a systematic review and meta-analysis in accordance with the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-analyses) guidelines37. All RCTs comparing bisphosphonates to controls for the treatment of low BMD in HIV-infected adults were included. Outcomes of interest were BMD changes measured by DXA at the lumbar spine, femoral neck, and total hip, and adverse events. Relevant RCTs were identified by electronic searching of the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library, MEDLINE, EMBASE, LILACS, the conference databases Aegis and NLM, the prospective trials registers ClinicalTrials.gov and Current Controlled Trials (www.controlled-trials.com/). Searches were conducted in September 2013. An update was made in July 2014, with the inclusion of the study presented at CROI 2014 by Negredo, et al.36. Two authors (Pinzone and Nunnari) independently reviewed all studies identified by the search strategy and assessed the risk of bias by means of the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials38. Data were analyzed using Review Manager 5.2.7. For dichotomous outcomes (i.e. number of participants with adverse events), we calculated risk ratios (RR) and 95% confidence intervals (CI). For quantitative outcomes (i.e. BMD) we estimated the difference in mean percentage change from baseline in the bisphosphonate and control group. When BMD values were not presented in the manuscript text, an electronic caliper was used to extract the data from figures39. For continuous outcomes, the effect estimates were combined using the fixedeffects model (also known as the weighted-average method). We examined statistical heterogeneity by the I² statistic and the Chi² test40. Additional data on the search strategy and statistical methods are shown as Supplementary data. Main characteristics of included studies The literature searches retrieved a total of 387 citations (Fig. 1). From these, 13 articles were selected for further scrutiny and nine were included in the systematic review29-35,41,42. Two of these articles41,42 were extensions of a previously published trial33 and were considered as a single study in the systematic review. Our search for ongoing trials retrieved two studies that potentially met our inclusion criteria: one trial (ClinicalTrials.gov Identifier No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. or a t-score (compared to the mean BMD for a healthy, young (25-35 years old), sex- and ethnicity-matched reference population). The World Health Organization classifies osteopenia as a t-score between –1 and –2.5 and osteoporosis as a t-score of –2.5 or less6. Decreased BMD has been observed in several HIVinfected cohorts7-11. A recent meta-analysis reported the prevalence of osteoporosis and osteopenia in HIVpositive patients as 15 and 67%, respectively12. Osteoporosis was three times more prevalent in HIV-infected individuals compared with HIV-uninfected controls. The causes of altered bone mass acquisition and bone loss are not completely understood. Traditional risk factors, such as smoking, alcohol use, vitamin D deficiency, hypogonadism, physical inactivity, and low body weight, may contribute to the increased risk of osteopenia/osteoporosis7,13,14. The HIV virus itself can directly or indirectly alter osteoblastogenesis and osteoclastogenesis. In fact, HIV viral proteins vpr and gp120 have been shown to stimulate osteoclast activity15,16, whereas p55-gag was found to suppress osteoblast activity and induce osteoblast apoptosis17. Furthermore, increased production of proinflammatory cytokines, such as interleukin-6 and tumor necrosis factor-α, may promote bone resorption18,19. Though several studies have suggested an association between BMD loss and certain antiretroviral drugs, such as tenofovir (TDF)14,20,21 and protease inhibitors (PI)7,22, other studies have reported a 2-6% decrease in BMD after initiation of HAART regardless of the initial regimen choice23. The reasons for the early loss of BMD following HAART initiation are unclear. Moreover, longitudinal studies have found that after the initial bone loss, BMD seems to stabilize over time despite prolonged HAART administration24,25. Bisphosphonates are pyrophosphate analogues that inhibit bone resorption by binding to hydroxyapatite crystals26. Bisphosphonates are the most widely used drugs in the treatment of postmenopausal osteoporosis27. In HIV-infected patients, both alendronate and zoledronate have been used to increase BMD5. However, in a systematic review of Lin and Rieder28, the authors concluded that no recommendation could be made concerning the use of bisphosphonates in HIVpositive patients with low BMD as only three short-term small studies were available when their systematic review was published29-31. Other randomized controlled trials (RCTs) have been subsequently performed32-36. In light of recently published studies, we aimed at reviewing the current evidence on the use of bisphosphonates to increase BMD in patients with HIV infection. © Permanyer Publications 2014 AIDS Reviews. 2014;16 Additional records identified through other sources (n = 0) Records after duplicates removed (n = 154) Records screened (n = 154) Records excluded (n = 143) Articles assessed for eligibility (n = 13) Articles excluded (n = 3) n = 1 secondary analysis of a randomized controlled trial included in this systematic review n = 1 not a randomized controlled trial n = 1 ongoing trial Studies included in qualitative synthesis (n = 8) corresponding to 10 publications Studies included in quantitative synthesis (meta-analysis) (n = 8) Figure 1. Flow diagram of studies considered for inclusion (adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009;6:e1000097. For more information, visit www.prisma-statement.org). NCT00795483) evaluated the efficacy and safety of annual and biennial zoledronic acid for the treatment of osteoporosis in HIV-positive patients. At the time of our first search, no results had been published; however, an abstract was presented at CROI 201436 and these results were used to update our meta-analysis in July 2014, for a total of eight studies meeting our inclusion criteria. The other trial (ClinicalTrials.gov Identifier NCT00662077) aimed at evaluating the efficacy and safety of ibandronate for the treatment of osteoporosis in HIV-infected adults. However, it has currently been suspended due to financial difficulties. The characteristics of the studies included in the systematic review are described in table 1. We identified and included eight RCTs29-36, which assessed the effect of bisphosphonates on BMD in a total of 328 adult participants with HIV infection. The trials were conducted in the USA30,32,34, France35, Italy29, New Zealand33, and Spain31,36. The majority of participants were male and taking HAART at baseline. Most of them had consistent suppression of viral replication at the time of enrollment. Median baseline CD4+ T-cell counts ranged from 422 to 561 cells/μl. Four studies32-35 provided details on the number of patients receiving TDF, which ranged from 0 to 53%. Four trials30,32,33,35 reported the number of participants treated with regimens that included a PI (range 37-66%). Three studies31,35,36 recruited only participants who had BMD t-score ≤ –2.5, two studies29,30 recruited participants with BMD t-score < –1, two studies32,34 included participants with BMD t-score ≤ –1.5, and one trial33 enrolled subjects with BMD t-score ≤ –0.5. Five trials29-32,35 assessed alendronate versus placebo or no intervention in 224 participants. In all five studies, oral alendronate was given in a dose of 70 mg weekly. Three trials33,34,36 assessed zoledronate versus placebo or no drug in 104 participants. Intravenous zoledronate was given in a single dose of 5 mg in the Huang trial34; in the Bolland trial33,41,42, patients received two annual 4 mg doses of zoledronate. In the Negredo 2014 trial36, patients in the intervention arm received an annual or biennial 5 mg dose of zoledronate; moreover, all participants received lifestyle modifications. In © Permanyer Publications 2014 Records identified through database searching (n = 387) No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. Included Eligibility Screening Identification Marilia Rita Pinzone, et al.: Bisphosphonates for Increasing BMD in HIV 215 216 Italy USA Spain USA New Zealand USA France Spain Guaraldi, et al. 200429 Mondy, et al. 200530 Negredo, et al. 200531 McComsey, et al. 200732 Bolland, et al. 200733, 200841, 201242 Huang, et al. 200934 Rozenberg, et al. 201235 Negredo, et al. 201436 96 96 52 96†† 48 96 48 52 19 – 100 ≤ –2.5 at the LS 100 and/or hip ≤ –1.5 at the LS 27 or hip < –0.5 at the LS 7 or total hip ≤ –1.5 at the LS 21 Calcium carbonate 1 g/day and vitamin D 400 IU/day Two annual 5 mg doses Lifestyle of intravenous modifications zoledronate vs. one biennial 5 mg dose of intravenous zoledronate vs. no drug Calcium carbonate 500 mg/day and vitamin D 400 IU/day Single 5 mg infusion of Calcium 1 g/day zoledronate vs. placebo and vitamin D 400 IU/day Alendronate 70 mg/ week vs. placebo 44 44 – 45‡ 49 49 48‡ – 95 90 100 71 96 87 71 Age Male (years)† participants (%) Dietary counseling 49§/40¶ to ensure a calcium dietary intake of 1.2 g/day Calcium carbonate 1 g/day and vitamin D 400 IU/day Calcium carbonate 1 g/day and vitamin D 500 IU/day Co-interventions Two annual 4 mg doses Calcium 400 mg/ of intravenous day and vitamin D zoledronate vs. placebo 50,000 IU/month Alendronate 70 mg/ week vs. placebo Alendronate 70 mg/ week vs. no drug Alendronate 70 mg/ week vs. no drug Alendronate 70 mg/ week vs. no drug Participants Intervention with osteoporosis (%)* ≤ –2.5 at the LS, 100 hip or trochanter < –1 at the LS < –1 at the LS or FN 31 (21/10)§§ < –2.5 at the LS, hip and/ ortrochanter 44 (20/24) 30 (15/15) 43 (21/22) 82 (42/40) 26 (12/14) 31 (15/16) 41 (18/23) Trial Sample size BMD t-score duration (treatment/ for inclusion (weeks) control group) (n) – 422‡ 523 540 469‡ 346§/367¶ 561‡ 533 CD4+ T-cell count (cells/μl)† – 84 –‡‡ 81** 91 88** – – – 100 97 100 99 100 100 100 – 32 53 0 38 – – – – 57 – 37 66 – 61 – Participants Participants Participants Participants with HIV viral on HAART (%) on TDF (%) on PI (%) load < 400 copies/ml (%) No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. © Permanyer Publications 2014 *BMD t-score ≤ –2.5. †Mean unless otherwise indicated. ‡Median. §Median value in the intervention group. ¶Median value in the control group. **Participants with HIV viral load < 50 copies/ml. ††The initial trial duration was 96 weeks33, however patients were followed up for an additional four years after completion of the trial in an unblinded, open-ended extension study and results were published41,42. ‡‡The majority of participants had HIV viral load < 400 copies/ml, but the exact proportion was not stated. §§Patients were initially randomized in a 2:1 fashion to receive zoledronate (n = 21) plus lifestyle modifications or lifestyle modifications only (n = 10). At week 48, subjects from the zoledronate group were reallocated to the annual group (n = 12, zoledronate 5 mg/year for two years) or biennial group (n = 9, one 5 mg dose in two years). BMD: bone mineral density; FN: femoral neck; LS: lumbar spine; PI: protease inhibitors; TDF: tenofovir; –: not reported. Country Study authors, year [reference] Table 1. Characteristics of included studies AIDS Reviews. 2014;16 Effect of bisphosphonates on bone mineral density percentage change after 48 weeks of treatment Lumbar spine Four trials29,30,32,35 involving 198 patients compared the effect of alendronate versus placebo or no treatment. A significant increase in BMD at the lumbar spine was observed at 48 weeks in the treatment group (MD: 2.45%; 95% CI: 1.64-3.26). However, there was evidence for substantial statistical heterogeneity between trials (I2 = 71%, Chi2 p = 0.02). Three trials33,34,36 involving 104 patients compared the effect of zoledronate versus placebo or no drug. Zoledronate improved lumbar BMD by 4.6% (95% CI: 2.89-6.32) after 48 weeks. There was no evidence for statistical heterogeneity between trials (I2 = 33%; Chi2 p = 0.22). Pooling 48-week results for trials assessing oral and intravenous bisphosphonates, the positive effects of bisphosphonates on BMD at the lumbar spine were confirmed (MD: 2.84%; 95% CI: 2.11-3.57). However, there was evidence for statistical heterogeneity between trials (I2 = 67%, Chi2 p = 0.005) (Fig. 2). Femoral neck Three trials involving 154 patients evaluated the effect of alendronate on femoral neck BMD at 48 weeks29,30,32. Alendronate significantly improved BMD at the femoral neck (MD: 1.27%; 95% CI: 0.39-2.16). There was no statistically significant heterogeneity between trials (I2 = 34%, Chi2 p = 0.22). In two trials comparing zoledronate to placebo33,34, BMD at the femoral neck did not significantly differ between the two groups (MD: 0.6%; 95% CI: –1.56-2.76). There was substantial statistical heterogeneity between trials (I2 = 75%, Chi2 p = 0.05). Pooling 48-week results for trials assessing oral and intravenous bisphosphonates, a positive effect of bisphosphonates on BMD at the femoral neck was observed (MD: 1.18%; 95% CI: 0.35-2). There was evidence for moderate statistical heterogeneity between trials (I2 = 46%, Chi2 p = 0.12) (Fig. 3). Total hip In three trials comparing alendronate versus placebo or no treatment30,32,35, alendronate increased total hip BMD by 2.26% (95% CI: 1.45-3.07) after 48 weeks. There was no evidence for statistical heterogeneity between trials (I2 = 36%, Chi2 p = 0.21). In three trials involving 104 patients33,34,36, zoledronate was found to increase BMD at the total hip (MD: 1.74%; 95% CI: 0.43-3.06). Pooling 48-week results for trials assessing oral and intravenous bisphosphonates, a positive effect of bisphosphonates on total hip BMD was observed (MD: 2.12%; 95% CI: 1.43-2.81). There was no statistically significant heterogeneity between trials (I2 = 28%, Chi2 p = 0.22) (Fig. 4). Effect of bisphosphonates on bone mineral density percentage change after 96 weeks of treatment Lumbar spine Only three studies evaluated BMD at the lumbar spine after 96 weeks. In the zoledronate trials33,36, a significant increase in lumbar spine BMD was observed in the treatment group when compared to the control arm (MD: 7.12%; 95% CI: 4.74-9.51). Analogously, in the Rozenberg trial35 alendronate had a positive impact on lumbar spine BMD (MD: 6.3%; 95% CI: 3.61-8.99). Pooling 96-week results, the positive effects of bisphosphonates on BMD at the lumbar spine were confirmed (MD: 6.76%; 95% CI: 4.98-8.54). No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. the majority of studies, vitamin D and calcium supplements were given to all participants. In the Negredo 2005 trial31, participants received dietary counseling to ensure adequate daily calcium intake. In two trials, the duration of administration of bisphosphonates was 48 weeks30,32, in two trials it was 52 weeks29,34, in four trials it was 96 weeks31,33,35,36. However, Bolland, et al. followed up patients for an additional four years after completion of the trial in an unblinded, open-ended extension study without administration of additional antiresorptive medication41,42. Those studies were included in the qualitative analysis, but not in the quantitative one. In the Negredo 2014 trial36, patients assigned to the zoledronate group were reallocated at week 48 to the annual group (5 mg per year, two doses in two years) or biennial group (one dose in two years). As a consequence, at week 96 only data from subjects belonging to the annual group could be included in the quantitative analysis. The review authors’ judgments regarding risk of bias in the included studies are shown as Supplementary data. © Permanyer Publications 2014 Marilia Rita Pinzone, et al.: Bisphosphonates for Increasing BMD in HIV 217 Favors control Total Weight Mean difference IV, fixed, 95% CI 23 40 16 24 103 12.9% 51.1% 9.5% 8.3% 81.8% 0.30 (–1. 73, 2.33) 2.28 (1.26, 3.30) 3.90 (1.53, 6.27) 5.20 (2.66, 7.74) 2.45 (1.64, 3.26) 22 15 10 47 4.6% 7.9% 5.7% 18.2% 5.00 (1.59, 8.41) 3.00 (0.40, 5.60) 6.50 (3.44, 9.56) 4.60 (2.89, 6.32) Total (95% CI) 152 150 100.0% Heterogeneity: Chi2 = 18.32, df= 6 (p = 0.005); I2 = 67% Test for overall effect: Z = 7.63 (p < 0.00001) Test for subgroup differences: Chi2 = 4.96; df = 1 (p = 0.03); I2 = 79.8% 2.84 (2.11, 3.57) Study or subgroup Mean SD Total Mean SD Alendronate versus placebo or no drug Guaraldi 2004 4 3.36 18 3.7 3.2 McComsey 2007 3.38 2.76 42 1.1 1.9 Mondy 2005 5.2 2.63 15 1.3 4 Rozenberg 2012 5.5 4.7 20 0.3 3.7 Subtotal (95% CI) 95 Heterogeneity: Chi2 = 10.37; df = 3 (p = 0.02); I2 = 71% Test for overall effect: Z = 5.95 (p < 0.00001) Zoledronate versus placebo or no drug Bolland 2007 8.4 5.4 21 3.4 6 Huang 2009 3.7 4.1 15 0.7 3.1 Negredo 2014 5.9 3 21 –0.6 4.48 Subtotal (95% CI) 57 Heterogeneity: Chi2 = 2.99; df = 2 (p = 0.22); I2 = 33% Test for overall effect: Z = 5.27 (p < 0.00001) –4 –2 Favors control 0 2 4 Favors bisphosphonate Figure 2. Forest plot of the effect of bisphosphonates on lumbar spine bone mineral density after 48 weeks of treatment. Femoral neck Only Bolland, et al.33 reported on femoral neck BMD at 96 weeks; BMD did not significantly differ in the two groups (MD: 2.3%; 95% CI: –0.69-5.29). Total hip Three RCTs evaluated the impact of bisphosphonates on total hip BMD at 96 weeks. Zoledronate significantly increased BMD at the total hip (MD: 3.67%; 95% CI: 1.66-5.69)33,36. In the Rozenberg trial35, the difference between the alendronate and control group was not statistically significant (MD: 2.1%; 95% CI: –0.95-5.15). Pooled 96-week data showed BMD significantly increased in the bisphosphonate group (MD: 3.2%; 95% CI: 1.52-4.88). There was no evidence for statistical heterogeneity between trials (I2 = 0%, Chi2 p = 0.54). In the Negredo 2014 trial, no significant differences in BMD at the lumbar spine and total hip were 218 observed over 96 weeks between patients receiving annual and biennial zoledronate36. Analogously, Bolland, et al. reported that the effects of two annual 4 mg doses of zoledronate on BMD persisted for at least five years after the second dose41,42. In fact, the authors have shown patients receiving zoledronate had significantly higher BMD at the lumbar spine (+3.7%; 95% CI: 0.3-7%) and total hip (+2.3%; 95% CI: 0.3-4.3%) between one and five years after the second dose. The Negredo 2005 trial31 could not be included in the meta-analysis of quantitative outcomes because the authors did not report on BMD percentage change over time (only t-scores were provided) and did not provide standard deviations. For the Guaraldi trial29, we imputed standard deviation from the average standard deviation of the other RCTs assessing alendronate, which were included in the meta-analysis. Sensitivity analysis with exclusion of this trial did not significantly change the results (data not shown). No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. Favors bisphosphonate © Permanyer Publications 2014 AIDS Reviews. 2014;16 Study or subgroup Mean SD Total Favors control Mean SD Total Weight Mean difference IV, fixed, 95% CI 23 40 16 79 14.0% 65.3% 6.2% 85.6% 3.00 (0.81, 5.19) 1.00 (–0.02, 2.02) 0.24 (–3.05, 3.53) 1.27 (0.39, 2.16) 22 15 37 11.6% 2.9% 14.4% –0.50 (–2.91, 1.91) 5.00 (0.16, 9.84) 0.60 (–1.56, 2.76) Alendronate versus placebo or no drug Guaraldi 2004 –0.5 3.93 18 –3.5 3 McComsey 2007 2.2 2.56 42 1.2 2.12 Mondy 2005 2.33 5.3 15 2.09 3.88 Subtotal (95% CI) 75 Heterogeneity: Chi2 = 3.04; df = 2 (p = 0.22); I2 = 34% Test for overall effect: Z = 2.81 (p = 0.005) Zoledronate versus placebo or no drug Bolland 2007 2.5 4.7 21 3 3.2 Huang 2009 3.2 2.2 15 –1.8 9.3 Subtotal (95% CI) 36 Heterogeneity: Chi2 = 3.98; df = 1 (p = 0.05); I2 = 75% Test for overall effect: Z = 0.54 (p = 0.59) Total (95% CI) 111 116 100.0% Heterogeneity: Chi2 = 7.34, df= 4 (p = 0.12); I2 = 46% Test for overall effect: Z = 2.81 (p = 0.005) Test for subgroup differences: Chi2 = 0.32; df = 1 (p = 0.57); I2 = 0% 1.18 (0.35, 2.00) –4 –2 Favors control 0 2 4 Favors bisphosphonate Figure 3. Forest plot of the effect of bisphosphonates on femoral neck bone mineral density after 48 weeks of treatment. Tolerability profile of bisphosphonates Alendronate All included studies29-32,35 reported on adverse events; however, we were able to combine data in a metaanalysis only for gastrointestinal side effects. For other adverse events we presented the data in narrative form. In two trials30,31, the authors did not report any adverse events in either the treatment or control group. In one study29, no serious drug-related adverse events occurred. The incidence of gastrointestinal side effects, a concern with bisphosphonates, was reported to be 10% in both groups. The Rozenberg trial35 reported only on serious adverse events: 19 serious adverse events occurred in 13 patients, comprising four patients in the alendronate arm (acute prostatitis and lithotripsy; adrenal insufficiency and left otitis externa; iron deficiency anemia; and death after diagnosis of epidermoid carcinoma) and nine patients in the placebo arm (three episodes of benzodiazepine withdrawal syndrome, Helicobacter pylori gastritis, and a depressive syndrome; inferior myocardial infarction; pneumopathy; viral gastroenteritis; vitrectomy; Mycoplasma pneumoniae pneumonia; lung superinfection; pneumonia; and an allergic reaction). However, none of these adverse events appeared clearly associated with alendronate use. The incidence of gastrointestinal adverse events was not reported. In the McComsey trial32, the incidence of serious adverse events was 19% in the alendronate group and 35% in the placebo group. Two out of 42 participants in the alendronate group compared with four out of 40 participants in the placebo group suffered from gastrointestinal manifestations. No drug-related withdrawals were reported in the five RCTs assessing alendronate versus placebo or no intervention29-32,35. Four trials29-32 involving 180 patients reported on gastrointestinal adverse events. There was no statistically significant difference in the risk of gastrointestinal side effects in the alendronate group versus the control No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. Favors bisphosphonate © Permanyer Publications 2014 Marilia Rita Pinzone, et al.: Bisphosphonates for Increasing BMD in HIV 219 Favors control Total Weight Mean difference IV, fixed, 95% CI 40 16 24 80 56.5% 7.8% 8.3% 72.6% 2.64 (1. 72, 3.56) 0.55 (–1.93, 3.03) 1.30 (–1.09, 3.69) 2.26 (1.45, 3.07) 22 15 10 47 11.2% 2.0% 14.2% 27.4% 0.50 (–1.56, 2.56) 5.00 (0.16, 9.84) 2.25 (0.42, 4.08–) 1.74 (0.43, 3.06–) Total (95% CI) 134 127 100.0% Heterogeneity: Chi2 = 6.98, df= 5 (p = 0.22); I2 = 28% Test for overall effect: Z = 6.02 (p < 0.00001) Test for subgroup differences: Chi2 = 0.44; df = 1 (p = 0.51); I2 = 0% 2.12 (1.43, 2.81) Study or subgroup Mean SD Total Mean SD Alendronate versus placebo or no drug McComsey 2007 3.95 2.21 42 1.31 2.03 Mondy 2005 2.79 3.88 15 2.24 3.08 Rozenberg 2012 2.7 4.6 20 1.4 3.2 Subtotal (95% CI) 77 Heterogeneity: Chi2 = 3.11; df = 2 (p = 0.21); I2 = 36% Test for overall effect: Z = 5.48 (p < 0.00001) Zoledronate versus placebo or no drug Bolland 2007 2.5 3.2 21 2 3.7 Huang 2009 3.2 2.2 15 –1.8 9.3 Negredo 2014 3.5 2.07 21 1.25 2.58 Subtotal (95% CI) 57 Heterogeneity: Chi2 = 3.43; df = 2 (p = 0.18); I2 = 42% Test for overall effect: Z = 2.59 (p = 0.010) –4 –2 Favors control 0 2 4 Favors bisphosphonate Figure 4. Forest plot of the effect of bisphosphonates on total hip bone mineral density after 48 weeks of treatment. group (RR: 0.72; 95% CI: 0.22-2.37). There was no evidence for heterogeneity between trials (I2 = 0%, Chi2 p = 0.43). Zoledronate Adverse events occurring in RCTs assessing zoledronate versus placebo could not be pooled together in a meta-analysis, so we presented a narrative synthesis. In the Huang trial34, one patient developed uveitis within 72 hours of the drug infusion. In addition, the authors reported that serum calcium levels dropped slightly over the study period in zoledronate recipients as compared to placebo. Premedication with 1 g acetaminophen was offered to all participants prior to the infusion. In the Bolland trial33, no premedication was given. Two patients in the zoledronate group experienced acute-phase reactions that led them to discontinue study treatment after the first infusion. No 220 other treatment-related adverse events were reported. During the extension studies41,42, none of the participants had any potential adverse events from zoledronate. In the Negredo 2014 trial36, two patients in the zoledronate group had asthenia and two had fever within 48 hours after the infusion; these symptoms were treated with acetaminophen or ibuprofen. No discontinuations were due to drug-related adverse events. Discussion In our systematic review, we evaluated the effect of oral and intravenous bisphosphonates on BMD in HIVinfected adults. We found that bisphosphonates significantly increased BMD at the lumbar spine and total hip after 48 and 96 weeks of treatment. The BMD also increased at the femoral neck after 48 weeks, though the estimated effect was driven by alendronate RCTs, with zoledronate showing no significant impact on femoral neck BMD at 48 and 96 weeks. No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. Favors bisphosphonate © Permanyer Publications 2014 AIDS Reviews. 2014;16 week is also recommended to prevent bone loss as well as smoking cessation and limitation of alcohol intake5. Our meta-analysis has several limitations: first, it was based on a limited number of trials with a small sample size and a short length of follow-up. None of the trials were adequately powered to detect the impact of bisphosphonates on a clinically important outcome such as fracture risk. Secondly, for quantitative outcomes there was considerable statistical heterogeneity among trials. Several factors, including different study design and enrollment criteria, may have contributed to heterogeneity. However, heterogeneity describes variation in the magnitude not the direction of the effect, with all effect measures consistent with an increase in BMD at the lumbar spine and total hip over the short-term for both oral and intravenous bisphosphonates. Thirdly, considering the small number of included studies, we were not able to conduct a sensitivity analysis with exclusion of trials at high risk of bias. Finally, we could not assess whether differences in HAART regimens across studies might have contributed to the observed changes in BMD. In conclusion, our meta-analysis showed that administration of oral and intravenous bisphosphonates was associated with increased BMD at the lumbar spine and total hip over two years in patients with HIV infection. However, the majority of participants were relatively young men with well-controlled HIV and a low risk of fragility fractures in the immediate future. Further studies in high-risk populations, such as older persons and postmenopausal women, are warranted. Larger studies with extended follow-up are needed to better define the longterm safety and efficacy profile of bisphosphonates for the treatment of low BMD in the setting of HIV infection. Acknowledgements We thank the following trial authors who responded to our requests for further information: Mark Bolland, Eugenia Negredo, and Giovanni Guaraldi. We also thank Katharine Ker for her valuable comments and suggestions. Conflict of interest None of the authors have any conflict of interest to declare. Funding sources None to declare. Supplementary Data Supplementary data is available at AIDS Reviews journal online (http://www. aidsreviews.com). This data is provided by the author and published online to benefit the reader. The contents of all supplementary data are the sole responsibility of the authors. No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. The ultimate goal of long-term osteoporosis treatment is the prevention of fractures. However, since fractures may occur at a variable length of time after the onset of osteoporosis, short-term trials are not able to find significant differences between patients receiving bisphosphonates and patients who do not. In addition, it is unclear if patients receiving bisphosphonates may discontinue treatment after a few years without increasing their fracture risk. Extension studies in postmenopausal women taking bisphosphonates suggest that patients with a t-score < –2.5 at the femoral neck after 3-5 years of treatment are still at increased risk of vertebral fractures and may benefit from continued therapy43. In patients with HIV infection, the only extension study evaluating the long-term effect of zoledronate was published in 2012 by Bolland, et al.42. The authors showed that the effects of two annual doses of 4 mg zoledronate on BMD in HIV-positive men persisted for five years after the second dose. However, the study was relatively small and was not powered to detect significant differences in fracture risk. In addition, the authors enrolled relatively young men with a baseline t-score < –0.5 and well-controlled HIV; as a consequence, their results may not be generalizable to populations with lower BMD or uncontrolled HIV infection. Bisphosphonates were generally well-tolerated. No drug-related withdrawals were reported in the five RCTs assessing alendronate versus placebo or no intervention. The incidence of gastrointestinal adverse events was similar in the treatment and control group. As for zoledronate, one patient in the Huang trial34 developed uveitis and two patients in the Bolland trial33 discontinued treatment after the first dose because of acute-phase reactions. Major concerns associated with prolonged use of bisphosphonates are osteonecrosis of the jaw44 and atypical femoral fractures due to over-suppression of bone turnover45. These complications were not reported in any trial included in our systematic review. This is not unexpected considering the rarity of these adverse effects as well as the small number of participants involved and the short duration of RCTs. Adequate calcium and vitamin D intake is important to prevent BMD loss and reduce the risk of fractures5. Vitamin D deficiency has been shown to be highly prevalent in HIV-positive subjects46. As a consequence, current European guidelines suggest screening patients at risk for vitamin D hypovitaminosis and consider calcium/vitamin D supplementation when dietary intake is insufficient to maintain good bone health47. Lifelong participation in 30 minutes of weight-bearing and muscle-strengthening exercise at least three days a © Permanyer Publications 2014 Marilia Rita Pinzone, et al.: Bisphosphonates for Increasing BMD in HIV 221 1. Palella F, Baker R, Moorman A, et al. HIV Outpatient Study Investigators. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27-34. 2. Scarpino M, Pinzone M, Di Rosa M, et al. Kidney disease in HIV-infected patients. Eur Rev Med Pharmacol Sci. 2013;17:2660-7. 3. Pinzone M, Fiorica F, Di Rosa M, et al. Non-AIDS-defining cancers among HIV-infected people. Eur Rev Med Pharmacol Sci. 2012;16:1377-88. 4. Castronuovo D, Cacopardo B, Pinzone M, Moreno S, Nunnari G. Bone disease in the setting of HIV infection. Eur Rev Med Pharmacol Sci. 2013;17:2413-9. 5. McComsey G, Tebas P, Shane E, et al. Bone disease in HIV infection: a practical review and recommendations for HIV care providers. Clin Infect Dis. 2010;51:937-46. 6. World Health Organization Study Group. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Technical Report Series. 1994;843:1-129. 7. Tebas P, Powderly W, Claxton S, et al. Accelerated bone mineral loss in HIV-infected patients receiving potent antiretroviral therapy. AIDS. 2000;14:F63-7. 8. Teichmann J, Stephan E, Lange U, et al. Osteopenia in HIV-infected women prior to highly active antiretroviral therapy. J Infect. 2003;46:221-7. 9. Arnsten J, Freeman R, Howard A, Floris-Moore M, Lo Y, Klein R. Decreased bone mineral density and increased fracture risk in aging men with or at risk for HIV infection. AIDS. 2007;21:617-23. 10. Arnsten J, Freeman R, Howard A, Floris-Moore M, Santoro N, Schoenbaum E. HIV infection and bone mineral density in middle aged women. Clin Infect Dis. 2006;42:1014-20. 11. Yin M, Dobkin J, Brudney K, et al. Bone mass and mineral metabolism in HIV+ postmenopausal women. Osteoporos Int. 2005;16:1345-52. 12. Brown T, Qaqish R. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS. 2006;20:2165-74. 13. Mondy K, Yarasheski K, Powderly WG, et al. Longitudinal evolution of bone mineral density and bone markers in human immunodeficiency virus-infected individuals. Clin Infect Dis. 2003;36:482-90. 14. Gallant J, Staszewski S, Pozniak A, et al. Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral naïve patients: a 3-year randomized trial. JAMA. 2004;292:191-201. 15. Fakruddin J, Laurence J. HIV envelope gp120-mediated regulation of osteoclastogenesis via receptor activator of nuclear factor kappa B ligand (RANKL) secretion and its modulation by certain HIV protease inhibitors through interferon-gamma/RANKL cross-talk. J Biol Chem. 2003;278:48251-8. 16. Fakruddin J, Laurence J. HIV-1 Vpr enhances production of receptor of activated NF-kappa B ligand (RANKL) via potentiation of glucocorticoid receptor activity. Arch Virol. 2005;150:67-78. 17. Cotter E, Malizia A, Chew N, Powderly W, Doran P. HIV proteins regulate bone marker secretion and transcription factor activity in cultured human osteoblasts with consequent potential implications for osteoblast function and development. AIDS Res Hum Retroviruses. 2007;23:1521-30. 18. Lam J, Takeshita S, Barker J, Kanagawa O, Ross F, Teitelbaum S. TNF-alpha induces osteoclastogenesis by direct stimulation of macrophages exposed to permissive levels of RANK ligand. J Clin Invest. 2000;106:1481-8. 19. Ishimi Y, Miyaura C, Jin C, et al. IL-6 is produced by osteoblasts and induces bone resorption. J Immunol. 1990;145:3297-303. 20. McComsey G, Kitch D, Daar E, et al. Bone and limb fat outcomes of ACTG A5224s, a substudy of ACTG A5202: a prospective, randomized, partially blinded phase III trial of ABC/3TC or TDF/FTC with EFV or ATV/r for initial treatment of HIV-1 infection. In: Program and abstracts of the 17th CROI, February 2010, San Francisco. [Abstract 106LB]. 21. Stellbrink H, Moyle G, Orkin C, et al. Assessment of safety and efficacy of abacavir/lamivudine and tenofovir/emtricitabine in treatment-naïve HIV-1 infected subjects. ASSERT: 48-Week Result. In: Program and abstracts of the 12th European AIDS Conference, November 2009, Cologne, Germany. 22. Duvivier C, Kolta S, Assoumou L, et al. Greater decrease in bone mineral density with protease inhibitor regimens compared with nonnucleoside reverse transcriptase inhibitor regimens in HIV-1 infected naive patients. AIDS. 2009;23:817-24. 23. Brown T, McComsey G, King M, Qaqish R, Bernstein B, da Silva B. Loss of bone mineral density after antiretroviral therapy initiation, independent of antiretroviral regimen. J Acquir Immune Defic Syndr. 2009;51:554-61. 222 24. Bolland M, Grey A, Horne A, et al. Bone mineral density remains stable in HAART-treated HIV-infected men over 2 years. Clin Endocrinol (Oxf). 2007;67:270-5. 25. Dolan S, Kanter J, Grinspoon S. Longitudinal analysis of bone density in human immunodeficiency virus-infected women. J Clin Endocrinol Metab. 2006;91:2938-45. 26. Russell R. Bisphosphonates: from bench to bedside. Ann NY Acad Sci. 2006;1068:367-401. 27. Bilezikian J. Efficacy of bisphosphonates in reducing fracture risk in postmenopausal osteoporosis. Am J Med. 2009;122:S14-21. 28. Lin D, Rieder M. Interventions for the treatment of decreased bone mineral density associated with HIV infection. Cochrane Database Syst Rev. 2007;18:CD005645. 29. Guaraldi G, Orlando G, Madeddu G, et al.Alendronate reduces bone resorption in HIV-associated osteopenia/osteoporosis. HIV Clin Trials. 2004;5:269-77. 30. Mondy K, Powderly W, Claxton SA, et al. Alendronate, vitamin D, and calcium for the treatment of osteopenia/osteoporosis associated with HIV infection. J Acquir Immune Defic Syndr. 2005;38:426-31. 31. Negredo E, Martinez-Lopez E, Paredes R, et al. Reversal of HIV-1-associated osteoporosis with once-weekly alendronate. AIDS. 2005;19:343-5. 32. McComsey G, Kendall M, Tebas P, et al. Alendronate with calcium and vitamin D supplementation is safe and effective for the treatment of decreased bone mineral density in HIV. AIDS. 2007;21:2473-82. 33. Bolland M, Grey A, Horne A, et al. Annual zoledronate increases bone density in highly active antiretroviral therapy-treated human immunodeficiency virus-infected men: a randomized controlled trial. J Clin Endocrinol Metab. 2007;92:1283-8. 34. Huang J, Meixner L, Fernandez S, McCutchan J. A double-blinded, randomized controlled trial of zoledronate therapy for HIV-associated osteopenia and osteoporosis. AIDS. 2009;23:51-7. 35. Rozenberg S, Lanoy E, Bentata M, et al. ANRS 120 Fosivir Study Group. Effect of alendronate on HIV-associated osteoporosis: a randomized, double-blind, placebo-controlled, 96-week trial (ANRS 120). AIDS Res Hum Retroviruses. 2012;28:972-80. 36. Negredo E, Bonjoch A, Pérez-Álvarez N, et al. A randomized open label study for comparing two doses of zoledronic acid in HIV infected patients [poster 782]. In: Program and abstracts of the 21st CROI, March 2014, Boston. 37. Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. 38. Higgins J, Altman D, Sterne J on behalf of the CSMG and the CBMG. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (eds.). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Available from: www.cochrane-handbook.org 39. Barnard A, Vickers R. Estimating effect sizes from graphs using electronic calipers: An analysis of the reliability and accuracy of a data-gathering method. Available from www.dtic.mil/dtic/tr/fulltext/u2/a520853.pdf 40. Deeks J, Higgins J, Altman D on behalf of the CSMG. Chapter 9: Analysing data and undertaking metaanalyses. In: Higgins JPT, Green S (eds.). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Available from: www.cochrane-handbook.org 41. Bolland M, Grey A, Horne A, et al.Effects of intravenous zoledronate on bone turnover and BMD persist for at least 24 months. J Bone Miner Res. 2008;23:1304-8. 42. Bolland M, Grey A, Horne A, et al. Effects of intravenous zoledronate on bone turnover and bone density persist for at least five years in HIVinfected men. J Clin Endocrinol Metab. 2012;97:1922-8. 43. Black D, Bauer D, Schwartz A, Cummings S, Rosen C. Continuing bisphosphonate treatment for osteoporosis-for whom and for how long? N Engl J Med. 2012;366:2051-3. 44. Khan A, Sandor G, Dore E, et al. Bisphosphonate associated osteonecrosis of the jaw. J Rheumatol. 2009;36:478-90. 45. Odvina C, Zerwekh J, Rao D, Maalouf N, Gottschalk F, Pak C. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005;90:1294-301. 46. Pinzone M, Di Rosa M, Malaguarnera M, et al. Vitamin D deficiency in HIV infection: an underestimated and undertreated epidemic. Eur Rev Med Pharmacol Sci. 2013;17:1218-32. 47. European AIDS Clinical Society. Guidelines: prevention and management of co-morbidities in HIV-positive persons. Available at: http://www. eacsociety.org/Portals/0/140601_EACS%20EN7.02.pdf. No part of this publication may be reproduced or photocopying without the prior written permission of the publisher. References © Permanyer Publications 2014 AIDS Reviews. 2014;16
Scaricare