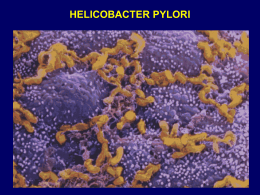
ROBERTO TESTA Direttore s.c. Gastroenterologia A.O. Santa Corona – Pietra Ligure L’Infezione da Helicobacter Pylori Manifestazioni Cliniche e Percorso Diagnostico L’Infezione da Helicobacter Pylori (Hp) è tra le più comuni infezioni in tutto il mondo. Patologie gastrointestinali correlate all’infezione da Hp: • Gastrite Cronica • Ulcera Peptica • Linfoma MALT • Adenocarcinoma Gastrico Figure 48-1 Seroprevalence of Helicobacter pylori as a function of age in developing countries and developed countries. (Data from Graham DY, Adam E, Reddy GT, et al: Seroepidemiology of Helicobacter pylori infection in India: Comparison of developing and developed countries. Dig Dis Sci 36:1084, 1991.) Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier Figure 48-2 Seroprevalence of Helicobacter pylori in the United States as a function of age in asymptomatic African Americans, Hispanics, and whites. (From Malaty HM, Evans DG, Evans DJJ, Graham DY: Helicobacter pylori in Hispanics: Comparison with blacks and whites of similar age and socioeconomic class. Gastroenterology 103:813, 1992.) Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier Figure 48-4 Seroprevalence of Helicobacter pylori (Hp) in the United States in spouses and children of parents who are seropositive or seronegative for H. pylori infection. (From Malaty HM, Graham DY, Evans DG, et al: Transmission of Helicobacter pylori infection. Studies in families of healthy individuals. Scand J Gastroenterol 26:927, 1991.) Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier Figure 34.5 Vacuolating cytotoxin, VacA. A. Pathogenic regions of VacA. B. Effects of VacA on the host. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 34.8 Functional consequences of H. pylori infection. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 34.7 Common topographic patterns of chronic active gastritis. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 49-3 Chronic nonspecific gastritides. A and B, Normal mucosal biopsy from the gastric body and antrum, respectively. C, Diffuse antral gastritis. The glands show an infiltrate of neutrophils, in addition to an increase in inflammatory cells in the lamina propria. This lesion is typically associated with Helicobacter pylori infection. D, Multifocal atrophic gastritis with intestinal metaplasia. Note several glands lined by goblet cells (arrow). Biopsy is from the gastric body, and similar changes were present in the antrum. E, Diffuse corporal atrophic gastritis in a man with pernicious anemia. The gland in the lower left is lined by goblet cells. Nests of enter-ochromaffin-like cells are also visible (arrows). Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier Figure 34.9 How antral H. pylori causes duodenal ulcers. H. pylori colonizes duodenal gastric metaplasia and reduces antral somatostatin activity, resulting in increased gastrin and enhanced acid secretion by parietal cells. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 35.7 Hormonal changes in duodenal and gastric ulceration. A. In H. pylori-associated antral-predominant gastritis, the illustrated hormonal changes lead to hypergastrinemia and increased acid production from the uninflamed gastric corpus. The increased acid load on the duodenum may lead to ulceration (see text for full explanation). B. In pangastritis, the same hormonal changes pertain, but the inflamed corpus produces reduced acid despite the hypergastrinemia. Such stomachs are at increased risk of gastric ulceration and adenocarcinoma. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 35.7 Hormonal changes in duodenal and gastric ulceration. A. In H. pylori-associated antral-predominant gastritis, the illustrated hormonal changes lead to hypergastrinemia and increased acid production from the uninflamed gastric corpus. The increased acid load on the duodenum may lead to ulceration (see text for full explanation). B. In pangastritis, the same hormonal changes pertain, but the inflamed corpus produces reduced acid despite the hypergastrinemia. Such stomachs are at increased risk of gastric ulceration and adenocarcinoma. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 50-3 Pie charts depicting conditions associated with peptic ulcer disease. The percentages shown are rough approximations based on studies from Western countries. The relative contributions of H. pylori infection and NSAID use to peptic ulcer vary considerably among different populations and, within populations, vary with age and socioeconomic status. Also, the separation depicted in this figure is somewhat artificial because NSAID use and H. pylori infection often coexist. ZE, Zollinger-Ellison syndrome. Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier Figure 50-7 Range of COX-1 and COX-2 selectivity of NSAIDs. (Modified from Warner TD, Mitchell JA: Cyclooxygenases: New forms, new inhibitors, and lessons from the clinic. FASEB J 18:790, 2004.) COX, cyclooxy-genase; IC50, concentration of NSAID that inhibits COX by 50%, NSAID, nonsteroidal antiinflammatory drug. Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier Figure 7.1 Overlap of gastrointestinal symptoms. Overlap between heartburn, epigastric pain, and early satiety in 3234 subjects from the general population with upper gastrointestinal symptoms. Figures do not add up to 100% due to rounding errors. Downloaded from: Clinical Gastroenterology and Hepatology (on 4 May 2008 11:39 AM) © 2007 Elsevier Figure 34.10 Possible mechanisms linking H. pylori and cancer. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 34.11 Evolution of premalignant changes into cancer in patients with H. pylori infection. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 37.1 Host genetic factors contributing to H. pylori-related gastric cancer. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Sintomi e Segni di Allarme • • • • • • Ematemesi o Melena Disfagia Perdita di Peso Vomito Persistente Massa Addominale Anemia da Possibile Sanguinamento Gastrointestinale RACCOMANDAZIONI DIAGNOSTICHE • La Ricerca di Hp è indicata nei pazienti con Ulcera Peptica in atto, pregressa storia di ulcera documentata, linfoma MALT. • La Ricerca di Hp dovrebbe essere eseguita solo se il medico ha programmato di trattare il paziente nel caso in cui l’esito dell’esame risultasse positivo. Tests Diagnostici di Infezione da Hp Sensibilità % Specificità % • Tests Invasivi • • • Urease Test Istologia Coltura 85-95 90-95 80-95 95-100 95-98 100 85-95 85-95 70-90 95-97 95-97 65-90 • Tests non Invasivi • • • C13 Urea Breath Test Hp Antigene Fecale Hp Anticorpi Sierici RACCOMANDAZIONI DIAGNOSTICHE • Nei pazienti che non abbiano ricevuto un PPI nelle 2 settimane precedenti o un Antibiotico entro le 4 settimane precedenti l’Esame Endoscopico, il test rapido all’ureasi è accurato e poco costoso. • Per i pazienti che sono stati trattati con PPI, la ricerca endoscopica di Hp deve includere biopsie dall’antro al corpo gastrico per l’evidenza istologica di Hp. Figure 34.12 Urease test. Top: positive; bottom: negative. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Figure 36.1 Biopsy protocol. Schematic representation of the biopsy protocol recommended by the Updated Sydney System when the objective is to map the severity and extent of gastritis. A minimum of two specimens is obtained from each of the antrum (A1 and A2 - lesser and greater curvature) and the corpus (B1 and B2 - lesser and greater curvature). In addition, one biopsy specimen from the incisura angularis (IA) is recommended to detect early atrophic and metaplastic changes, represented in blue. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier RACCOMANDAZIONI DIAGNOSTICHE • L’Esame Colturale o con PCR è raccomandato per testare la Sensibilità antibiotica, ma non è utilizzabile routinariamente. • L’Esame Colturale non è sensibile come il test rapido o l’esame istologico. Tests non Invasivi per Identificare Hp Urea Breath Test • Caratteristiche: Diagnosi di infezione in atto, rilevata dall’attività ureasica Hp dipendente nello stomaco. • Vantaggi: Sensibilità e Specificità >90%, utilizzabile nei bambini. Utile per la diagnosi iniziale e per valutare il trattamento. • Svantaggi: Richiede apparecchiature per rilevare C13, relativamente costose. Figure 34.13 Principles and results of C13 urea breath testing. Note the rapid rise in [13C]carbon dioxide following administration of [13C]urea. Downloaded from: Clinical Gastroenterology and Hepatology (on 27 April 2008 09:16 AM) © 2007 Elsevier Tests non Invasivi per Identificare Hp Tests Sierologici • Caratteristiche: Rileva Anticorpi anti-Hp IgG nel siero. • Vantaggi: I tests approvati hanno alta sensibilità e specificità. Poco costoso. Utile per screening iniziale. • Svantaggi: Rileva infezione pregressa, no infezione in atto. Utilità limitata per valutare l’eradicazione di Hp (riduzione lenta del titolo anticorpale). Tests non Invasivi per Identificare Hp Tests Fecali • Caratteristiche: Rileva l’antigene dell’Hp. • Vantaggi: Rileva l’infezione in atto. Utile per valutare l’eradicazione. Eccellente specificità e sensibilità. Poco costoso. Può essere il test di scelta nei bambini. • Svantaggi: La raccolta dei campioni di feci può costituire problema. RACCOMANDAZIONI DIAGNOSTICHE • Per Valutare l’Eradicazione di Hp sia Urea Breath Test sia Ricerca Hp Antigene nelle feci devono essere eseguiti dopo almeno 2 settimane dal termine della terapia. Figure 48-5 Proposed natural history of Helicobacter pylori infection in humans. Downloaded from: Gastrointestinal and Liver Disease 8e (on 27 April 2008 07:48 AM) © 2007 Elsevier
Scaricare