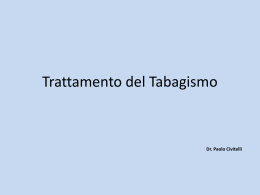
Associazione Scientifica Interdisciplinare per lo Studio delle Malattie Respiratorie 1 h) c r a N I ciSe ION TED S C ( A IT D TR D E S E D B A PAN IENCE AND X E ES D C E S X X S A / E E IND IND ORTS IN TAB A N P D O O E C TI LS ITA TION R NOW A RAPHI C E A AND LIOG ENC AL CIT I C BIB - S URN R E EVI - JO S L S, E U P O - SC M u ltid is c ip lin a ry R e s p ira to ry M e d ic in e Poste Italiane Spa - Spedizione in Abbonamento Postale - D.L. 353/2003 (convertito in L. 27/02/2004 n. 46) art. 1 comma 1, DCB MILANO ® Donner CF AIMAR Top Seminars 2009 “Inflammation and infection in the upper and lower respiratory tract”, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 1-4, 2009: background statements AIMAR Top Seminars 2009 “Infiammazione e infezione nelle vie respiratorie superiori e inferiori”, Seminario di consenso/dissenso – l’opinione degli esperti, Stresa, 1-4 aprile 2009: le basi razionali Uskul BT, Baysungur V, Aksoy F, Turan FE, Sevilgen G, Turker H, Halezeroglu S Combined use of transbronchial needle aspiration and PET/CT in mediastinal nodal staging of non small cell lung cancer Uso combinato di PET/CT e agoaspirato transbronchiale per la stadiazione linfonodale mediastinica del cancro polmonare non a piccole cellule Carrozzi L, Lazzaro C, Nardini S, Pistelli F, Silvi P, Viegi G La cessazione del fumo in pazienti con malattie respiratorie: alta priorità, componente integrante della terapia Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy anno 4 - n. 1 - Reg.Trib. Novara n.120 dell’11/11/2005 ISSN 1828-695X Multidisciplinary Respiratory Medicine vol. 4 n.1/february 2009:1-90 4 volume number february 2009 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 1 MULTIDISCIPLINARY RESPIRATORY MEDICINE OFFICIAL SCIENTIFIC JOURNAL OF AIMAR An Italian scientific journal of AIMAR dedicated to the advancement of knowledge in all fields of respiratory medicine. MRM publishes - in Italian and English - original articles, new methodological approaches, reviews, points of view, editorials, states of the art, position papers and congress proceedings. Editors Fernando De Benedetto, Chieti Claudio F. Donner, Borgomanero (NO) Claudio M. Sanguinetti, Roma Associazione Scientifica Interdisciplinare per lo Studio delle Malattie Respiratorie Multidisciplinary Respiratory Medicine Managing Editor Gianfranco Sevieri, Viareggio (LU) Editorial Office Manager Stefano Nardini, Vittorio Veneto (TV) Editorial Board Coordinator: Mario Polverino, Cava de’ Tirreni (SA) Sabina Antoniu, Iasi, Romania Alberto Braghiroli, Veruno (NO) Mauro Carone, Veruno (NO) Lucio Casali, Terni Mario Cazzola, Roma Stefano Centanni, Milano George Cremona, Milano Roberto Dal Negro, Bussolengo (VR) Filippo De Marinis, Roma Francesco Ioli, Veruno (NO) Giovanni Paolo Ligia, Cagliari Rasmi Magadle, Baka El-Garbia, Israel Riccardo Pela, Ascoli Piceno Luca Richeldi, Modena Roberto Torchio, Torino AIMAR Scientific Committee Coordinator: Luigi Allegra (MI) Allergology and Environmental Medicine: Emanuele Errigo (PV) Cardiac Surgery: Mario Viganò (PV) Cardiology: Nazzareno Galié (BO), Alessandro Palmarini (MI) Endocrinology: Aldo Pinchera (PI) Epidemiology: Fernando Romano (CH) Formation and Quality: Maurizio Capelli (BO), Piera Poletti (PD) Gastroenterology: Gabriele Bianchi Porro (MI), Lucio Capurso (RM) General Medicine: Claudio Cricelli (FI) Geriatrics: Emanuele Tupputi (BA), Stefano M. Zuccaro (RM) Imaging: Alessandro Carriero (NO), Francesco Schiavon (BL) Immunology: Giuseppe Montrucchio (TO) Infectivology: Ercole Concia (VR) Intensive Care: Marco Ranieri (TO) Internal Medicine: Roberto Corinaldesi (BO) Microbiology: Giancarlo Schito (GE) Neurology: Luigi Ferini Strambi (MI) Occupational Medicine: Plinio Carta (CA), Giacomo Muzi (PG) Oncology: Filippo De Marinis (RM), Cesare Gridelli (AV) Otolaryngology: Michele De Benedetto (LE), Desiderio Passali (SI) Pediatrics: Angelo Barbato (PD), Fernando M. De Benedictis (AN) Pharmacology: Ilario Viano (VC) Pneumology: Francesco Blasi (MI), Lucio Casali (TR), Mario Cazzola (RM), Giuseppe U. Di Maria (CT), Giuseppe Girbino (ME), Carlo Grassi (MI), Dario Olivieri (PR), Pier Luigi Paggiaro (PI), Paolo Palange (RM), Riccardo Pela (AP), Mario Polverino (Cava de’ Tirreni, SA). Relationships with Patients’ Organizations: Mariadelaide Franchi (RM) Thoracic Surgery: Francesco Sartori (PD) Editorial Office Novamedia s.r.l. Via Monsignor Cavigioli 10, 28021 Borgomanero (NO) Tel +39 0322 846549 – Fax +39 0322 843222 Lilia Giannini [email protected] Elisa Rossi [email protected] Editorial Supervision Rosemary Allpress, Alberto Braghiroli [email protected] Marketing & Advertising Gaudenzio Nidasio Tel +39 346 6964117 [email protected] MRM 1 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 2 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 3 Le raccomandazioni ERS in lingua italiana: un aiuto per smettere di fumare ERS guidelines in Italian: an aid help patients stop smoking 6 Piergiorgio Zuccaro Original Article / Articolo Originale Combined use of transbronchial needle aspiration and PET/CT in mediastinal nodal staging of non small cell lung cancer Uso combinato di PET/CT e agoaspirato transbronchiale per la stadiazione linfonodale mediastinica del cancro polmonare non a piccole cellule INDICE / INDEX Editoriale / Editorial 8 Bahadir T. Uskul, Volkan Baysungur, Ferda Aksoy, Fatma E. Turan, Gokcen Sevilgen, Hatice Turker, Semih Halezeroglu Documento ufficiale / Official statement La cessazione del fumo in pazienti con malattie respiratorie: alta priorità, componente integrante della terapia Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy 15 Laura Carrozzi, Carlo Lazzaro, Stefano Nardini, Francesco Pistelli, Patrizia Silvi, Giovanni Viegi Bacground statements / Basi razionali, AIMAR Top Seminars 2009 “Inflammation and infection in the upper and lower respiratory tract”, Expert Opinion Consensus/Dissensus Seminar, Stresa, Italy, April 1-4, 2009 AIMAR Top Seminars 2009 “Inflammation and infection in the upper and lower respiratory tract”, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 1-4, 2009: background statements AIMAR Top Seminars 2009 “Infiammazione e infezione nelle vie respiratorie superiori e inferiori”, Seminario di consenso/dissenso - l’opinione degli esperti, Stresa, 1-4 aprile 2009: le basi razionali 46 Claudio F. Donner Pathogenesis of respiratory inflammation Patogenesi dell'infiammazione respiratoria 50 Giuseppe Di Maria Cytology of inflammation Citologia dell'infiammazione 50 Matteo Gelardi, Maria Luisa Fiorella, Cosimo Russo, Raffaele Fiorella Inflammation in upper and lower airways: similarities and differences Infiammazione nelle vie respiratorie superiori e inferiori: somiglianze e differenze 52 Glenis Scadding Relation between infection and inflammation in the airways Relazione tra infezione e infiammazione nelle vie aeree 54 Wisia Wedzicha Diagnostic approach: clinical implications of the new experimental evidence L'approccio diagnostico: implicazioni cliniche delle nuove evidenze sperimentali 55 Mario Cazzola MRM 3 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 4 Integrated care approach to the upper airway patient Terapia integrata nella patologia delle vie aeree superiori 56 Delfo Casolino, Davide Padovani, Daria Salsi, Caterina Bruzzi Integrated care approach to the lower airways patient Il trattamento integrato del paziente con patologie delle basse vie respiratorie 57 Fernando De Benedetto Pharmacology of inhaled drugs Farmacologia dei farmaci assunti per via inalatoria 58 Francesco Scaglione Clinics of inhaled drugs Apetti clinici dei farmaci inalatori 60 Fulvio Braido Pharmacology of antibiotics Farmacologia degli antibiotici 61 Federico Pea Clinical aspects of antibiotic therapy in respiratory tract infections Aspetti clinici della terapia antibiotica nelle infezioni del tratto respiratorio 62 Pierluigi Viale Clinical implications of pharmacologic evidence: inflammation Conseguenze cliniche delle evidenze farmacologiche: l'infiammazione 63 Fulvio Braido Clinical implications of pharmacologic evidence: management approach to infection Conseguenze cliniche delle evidenze farmacologiche: approccio al trattamento delle infezioni 64 Lucio Casali, Valentina Malafoglia Pathogenetic and clinical framework of rhinosinusal disease Inquadramento patogenetico e clinico nella patologia rinosinusale 66 Luisa Bellussi Links between allergic rhinitis and asthma I legami tra asma e rinite allergica 67 Attilio Boner Medical treatment of allergic rhinitis and rhinosinusitis Terapia medica della rinite allergica e della rinosinusite 69 Michele de Benedetto Acute exacerbations of COPD Riacutizzazioni della BPCO 70 Gianni Balzano Inflammation in COPD and tobacco smoking L'infiammazione nella BPCO e nel fumo di tabacco 71 Stefano Nardini, Caterina Baghiris New evidence from large international trials Nuove evidenze da ampi studi internazionali Robert Stockley 4 MRM 72 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 5 Rhinitis and sinusitis Le rinosinusiti 73 Desiderio Passali Asthma and rhinitis Asma e rinite 74 Alfredo Potena COPD BPCO 75 Stefano Centanni, Silvia Della Fiore Upper and lower respiratory tract infections Infezioni delle alte e basse vie respiratorie 77 Pierluigi Viale, Luigia Scudeller Innovation in pharmacological respiratory research Innovazione nella ricerca farmacologica in campo respiratorio 78 Giuseppe Recchia 80 From the CFC Bulletin 83 L'Angolo della Cultura (non solo Medicina...) Nello sguardo dell’amico scopriamo noi stessi In the eyes of a friend we discover ourself 85 RUBRICHE AIMAR Newsletter Francesco Iodice 88 Meeting Calendar Avviso importante ai Soci Si rammenta a tutti i Soci che, come più volte comunicato negli scorsi numeri di MRM, la rivista, non sarà più inviata senza la regolarizzazione dell'iscrizione ad AIMAR. A coloro che regolarizzeranno la loro posizione societaria in occasione del 2° Convegno Nazionale di Napoli (4-7 marzo prossimi) Mrm 1/09 sarà inviata nel corso del mese di marzo. Le modalità di pagamento della quota societaria per l'anno 2009 sono riportate nella penultima pagina di questo numero. MRM 5 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 6 Editoriale / Editorial Le raccomandazioni ERS in lingua italiana: un aiuto per smettere di fumare ERS guidelines in Italian: an aid help patients stop smoking Piergiorgio Zuccaro Istituto Superiore di Sanità, Osservatorio Fumo, Alcol e Droga Il documento “Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy” prodotto dalla Task Force on Smoking Cessation della Società Respiratoria Europea (ERS) [1] che viene pubblicato su questo numero di Multidisciplinary Respiratory Medicine (e che da qualche mese è disponibile sul sito dell'Osservatorio Fumo, Alcol e Droga dell'Istituto Superiore di Sanità all'indirizzo http://www.iss.it/ofad/index.php?lang=1) oltre che sancire in maniera inequivocabile che il fumo di tabacco è un importante determinante per le malattie respiratorie, introduce una serie di nuovi elementi di riflessione, non soltanto per coloro ai quali è destinato, cioè gli specialisti pneumologi e tutti coloro che si occupano di malattie respiratorie, ma anche per tutti gli altri professionisti sanitari e per i decisori politici. Come tutti sappiamo il fumo rappresenta il maggior fattore di rischio per lo sviluppo della broncopneumopatia cronica ostruttiva (BPCO) e del tumore polmonare e peggiora il controllo dell'asma. E sappiamo anche, come ribadito dai più recenti piani sanitari nazionali, che l'importanza epidemiologica di queste malattie respiratorie è seconda solo a quella delle malattie cardiovascolari. Quindi riuscire a far smettere di fumare i fumatori attivi “sani”, aiuta a prevenire, prima di tutto, le principali malattie respiratorie. Tuttavia, come accennato, il documento non si limita a ribadire questi concetti, al limite ovvi, ma, basandosi sulle evidenze disponibili e sul consenso di un panel di esperti, sottolinea che la cessazione dal fumo è uno dei mezzi più importanti - quando non il più importante - per migliorare la prognosi e la qualità di vita ai pazienti con malattie respirato- + Piergiorgio Zuccaro Istituto Superiore di Sanità, Osservatorio Fumo, Alcol e Droga Viale Regina Elena 299, 00161 Roma, Italia email: [email protected] Multidisciplinary Respiratory Medicine 2009; 4(1): 6-7 6 MRM rie e dovrebbe essere parte integrante di ogni servizio di pneumologia. A mia cognizione è la prima volta che la disassuefazione dal fumo viene definita come misura destinata a una popolazione selezionata, in un'ottica di vera e propria terapia e non di prevenzione. Ma non è l'unica novità Infatti, dopo aver ribadito la necessità dell'utilizzo di terapia sia farmacologica sia comportamentale per ottenere i migliori risultati in termine di cessazione definitiva del fumo, il documento raccomanda di includere stabilmente la disassuefazione e il controllo del fumo nella valutazione routinaria dei pazienti pneumopatici e ribadisce la necessità di fornire una copertura economica alle attività di disassuefazione (almeno quelle rivolte a malati: per esempio oltre agli pneumopatici, anche cardiopatici o oncologici). Quindi, la disassuefazione non solo come pratica terapeutica essenziale, ma anche come parte integrante del follow up dei malati respiratori. Il documento ha importanti risvolti - diretti e indiretti - anche per il nostro Paese. La traduzione italiana è stata promossa e sostenuta anche dall'osservatorio Fumo, Alcol e Droga (OssFAD) e, come accennato, da mesi fa parte della documentazione disponibile gratuitamente sul sito. Tale iniziativa si affianca ed è in continuità con una serie di altre iniziative tutte tese a migliorare il più possibile gli strumenti per il controllo del fumo a disposizione della classe medica e dei decisori politici. Un altro esempio di questo impegno dell'OssFAD è l'aggiornamento 2008 delle linee guida italiane per smettere di fumare destinate alle MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 7 riconosciuta come intervento sanitario e come tale incluso nei livelli essenziali di assistenza, in modo da poter essere tariffata a livello di ogni singola regione. L'obiettivo potrebbe essere quello di garantire la disassuefazione a tutti i fumatori dietro pagamento di un ticket, riservando il trattamento gratuito (a somiglianza di altri farmaci la cui prescrizione avviene su nota CUF) a coloro i quali, per causa di una malattia fumo-correlata in atto, sono nelle condizioni di dover a tutti i costi smettere di fumare. Ancora, i decisori politici debbono - conformemente a quanto raccomandato dall'Organizzazione Mondiale della Sanità nel suo documento per le politiche di disassuefazione in Europa [3] - decidersi a conferire risorse alla disassuefazione dal fumo in modo specifico e adeguato. Gli investimenti debbono essere tali da rendere possibile sia la realizzazione della formazione sulla disassuefazione dal fumo sugli operatori sanitari a tutti i livelli, dall'infermiere allo specialista sulla disassuefazione, sia la ricerca sulla disassuefazione come strumento terapeutico, oltre che preventivo. Un'idea potrebbe essere che una parte almeno delle risorse economiche provenienti dal controllo del fumo e dalla tassazione delle vendite dei prodotti derivati dal tabacco sia destinata alla disassuefazione dal fumo. Nell'attesa che un simile auspicio prenda corpo, un sentito ringraziamento per il lavoro svolto va ai colleghi che hanno partecipato alla stesura del documento originale e alle traduzioni in italiano. Le professionalità e la passione che mettono nel loro lavoro ci fanno sperare in un “futuro senza fumo” e dovrebbero essere di esempio anche ad altre categorie di specialisti in malattie fumo-correlate per le quali anche la disassuefazione dal fumo rappresenta una “elevata priorità, parte integrante della terapia”. P Zuccaro Editoriale - Editorial cure primarie e, segnatamente, alla medicina generale [2]. Il problema da affrontare prioritariamente oggi è però costituito dal fatto che, a fronte di un consenso nella comunità scientifica sulla “alta priorità” della cessazione e di numerosi documenti ufficiali di società scientifiche e organismi istituzionali e, financo, di direttive governative apparentemente stringenti (si pensi all'importanza data al fumo nel piano sanitario nazionale), a fronte di tutto ciò, la pratica clinica sembra in generale ignorare l'importanza del trattamento del fumatore, sia in prevenzione sia in terapia. Ne è riprova la non centralità del tema tabagismo nei congressi scientifici, la mancanza di relazioni nei corsi di aggiornamento professionale, lo scarso successo di vendite di farmaci per la cessazione, pur se sostenuti da evidenze di sicura efficacia. Come vediamo, sono in corso numerose iniziative e la traduzione del documento dell'ERS è una di queste - per cambiare questo stato di cose. Tuttavia, per dare operatività alle iniziative “tecniche” quali quelle descritte, è necessario che le istituzioni diano slancio alla disassuefazione dal fumo, investendovi almeno tante risorse quante ne vengono impiegate nella cosiddetta prevenzione del fumo nei ragazzi. Se è vero che le cinque raccomandazioni contenute nel documento e riportate nell'abstract dovrebbero essere memorizzate e tornare alla mente ogni volta che uno pneumologo si trovi di fronte un paziente con patologie respiratorie, è anche vero che i decisori politici non possono ignorare che le raccomandazioni contenute nel documento necessitano, per essere messe in pratica, di una “istituzionalizzazione” degli interventi di disassuefazione sui fumatori. Ciò presuppone che la disassuefazione dal fumo sia Bibliografia 1. Carrozzi L, Lazzaro C, Nardini S, Pistelli F, Silvi P, Viegi G. La cessazione del fumo in pazienti con malattie respiratorie: alta priorità, componente integrante della terapia. Traduzione del documento prodotto dalla ERS Task Force on Smoking Cessation: “Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy. P Tønnesen, L Carrozzi, KO Fagerström, C Gratziou, C Jimenez-Ruiz, S Nardini, G Viegi, C Lazzaro, IA Campbell, E Dagli, R West. Eur Respir J 2007;29:390-417.”. Multidisciplinary Respiratory Medicine 2009;5:4:15-45. 2. Istituto Superiore di Sanità. Linee guida per promuovere la disassuefazione dal fumo. ISS Roma, 2001- aggiornamento 2008 (http://www.iss.it/ofad) 3. WHO European Strategy for smoking cessation policy. Traduzione italiana: OMS. La strategia europea per la disassuefazione dal fumo. (http://www.aimarnet.it) MRM 7 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 8 Original Article / Articolo Originale Combined use of transbronchial needle aspiration and PET/CT in mediastinal nodal staging of non small cell lung cancer Uso combinato di PET/CT e agoaspirato transbronchiale per la stadiazione linfonodale mediastinica del cancro polmonare non a piccole cellule Bahadir T. Uskul1, Volkan Baysungur2, Ferda Aksoy3, Fatma E. Turan1, Gokcen Sevilgen2, Hatice Turker1, Semih Halezeroglu2 1 Chest Diseases Department, Sureyyapasa Chest Diseases and Thoracic Surgery Hospital, Istanbul, Turkey Thoracic Surgery Department, Sureyyapasa Chest Diseases and Thoracic Surgery Hospital, Istanbul, Turkey 3 Pathology Department, Sureyyapasa Chest Diseases and Thoracic Surgery Hospital, Istanbul, Turkey 2 ABSTRACT Background and Aims: We evaluated the combined use of conventional transbronchial needle aspiration (TBNA) and integrated positron emission tomography/computed tomography (PET/CT) in the mediastinal staging of non-small cell lung cancer (NSCLC). Materials and Methods: A total of 37 NSCLC patients with enlarged mediastinal lymph nodes (≥ 1 cm) that underwent both TBNA and PET/CT scanning were included. Histological examination of the surgical specimen was used as the “gold standard” to confirm lymph node metastasis, unless patients were found to be inoperable, due to N3 disease or extensive N2 disease, as determined by conventional TBNA. Results: Conventional TBNA was successfully conducted for 49 mediastinal lymph nodes in 37 patients and proved the presence of malignancy in 35 lymph node stations in 28 patients. PET/CT identified 52 positive and 32 negative lymph nodes. TBNA had 78% sensitivity, 100% specificity, 100% positive predictive value, 29% negative predictive value, and 80% accuracy, whereas the corresponding values for PET/CT were 88, 66, 73, 83, and 77%, respectively. The combined use of TBNA and PET/CT had an accuracy rate of 92% for nodal staging of NSCLC. Conclusions: Our results demonstrate that the combination of conventional TBNA, a minimally invasive procedure performed during routine diagnostic procedures, and the non-invasive PET/CT procedure provides high accuracy for nodal staging of NSCLC. Keywords: Bronchoscopy, integrated positron emission tomography/computed tomography, lung cancer, mediastinal staging, transbronchial needle aspiration. RIASSUNTO Scopo dello studio: Abbiamo valutato l'uso combinato dell'agoaspirazione transbronchiale convenzionale (TBNA) e dell'integrazione tomografia ad emissione di positroni/tomografia computerizzata (PET/CT) nella stadiazione linfonodale mediastinica del cancro polmonare non a piccole cellule (NSCLC). Materiali e metodi: Sono stati inclusi nello studio un totale di 37 pazienti con NSCLC e con linfoadenomegalia mediastinica (≥ 1 cm) che sono stati sottoposti sia a TBNA che a PET/CT. L'esame istologico del pezzo chirurgico è stato usato come “gold standard” per confermare la presenza di metastasi ai linfonodi mediastinici, a meno che i pazienti non risultassero inoperabili a causa della presenza di malattia N3 o N2 estesa, così come diagnosticato con la TBNA convenzionale. Risultati: La TBNA convenzionale è stata eseguita con successo su 49 linfonodi mediastinici in 37 pazienti e dimostrava la presenza di malignità in 35 stazioni linfonodali di 28 pazienti. La PET/CT identificava 52 linfonodi positivi e 32 negativi. La TBNA aveva una sensibilità del 78%, una specificità del 100%, un valore predittivo positivo del 100%, un valore predittivo negativo del 29% e un'accuratezza dell'80%, mentre per la PET/CT i rispettivi valori erano 88%, 66%, 73%, 83% e 77%. L'uso combinato della TBNA e della PET/CT raggiungeva un'accuratezza del 92% nella stadiazione linfonodale mediastinica dello SNCLC. + Bahadir T. Uskul Chest Diseases Department, Sureyyapasa Chest Diseases and Thoracic Surgery Hospital Zumrutevler mah. Nil cad. Hukukcular sitesi A-3 Blok Da: 8 Maltepe, Istanbul 34852, Turkey email: [email protected] Data di arrivo del testo: 24/11/2008 - Accettato per la pubblicazione: 14/1/2009 Multidisciplinary Respiratory Medicine 2009; 4(1): 8-14 8 MRM MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 9 Parole chiave: Agoaspirazione transbronchiale, broncoscopia, integrazione PET/CT, stadiazione mediastinica, tumore del polmone. INTRODUCTION Lung cancer is a common malignancy worldwide, with an increasing incidence. The extension of the tumor is the major determinant of treatment selection; thus, the evaluation of mediastinal lymph nodes is of the utmost importance. The identification of contralateral lymph node involvement in potentially resectable lung cancer [≥ Stage IIIB, N3 according to the tumor node metastases (TNM) classification system] is an indication of inoperability. Additionally, growing evidence suggests dramatically decreased 5-year survival rates associated with the malignant involvement of the ipsilateral mediastinal or subcarinal lymph nodes [1]. The benefits of neoadjuvant therapy prior to surgical resection have been demonstrated in stage IIIA (N2 by the TNM classification) non-small cell lung cancer (NSCLC) cases [2]. Computed tomography (CT) of the thorax is the standard initial method for the anatomical demonstration of enlarged mediastinal lymph nodes; however, it has limited sensitivity and specificity for metastases. Positron emission tomography (PET) imaging has higher sensitivity and specificity for the evaluation of mediastinal lymph nodes. The pooled sensitivities of CT and PET in the staging of lung cancer are 57 and 84%, and their specificities are 82 and 89%, respectively [3]. Higher sensitivity (89%), specificity (94%), and accuracy (93%) have been reported with the integrated use of PET/CT for the nodal staging of NSCLC [4]. However, up to 10-15% false positive rates have been reported with this method; thus, cytopathological confirmation of positive results is recommended [5,6]. Transbronchial needle aspiration (TBNA) is a helpful, reliable, and minimally invasive bronchoscopic biopsy technique used in the diagnosis and staging of lung cancer. According to a recent systematic review, the sensitivity and specificity for TBNA of mediastinal lymph nodes are 76 and 96%, respectively. This sensitivity is close to that of cervical mediastinoscopy (81%) [7], which is performed in the operating room under general anesthesia and has an associated 2-3% complication rate and 0.1% surgical mortality [8]. Overall, TBNA is safe and inexpensive compared to mediastinoscopy. A positive TBNA may preclude the need for additional surgical staging of the mediastinum [9]. The present study evaluated the use of TBNA alone, PET/CT alone, or combined TBNA and PET/CT in the identification of mediastinal lymph nodes with malignant involvement, for nodal staging of NSCLC. MATERIALS AND METHODS NSCLC patients who underwent TBNA of mediastinal lymph nodes during fiber optic bronchoscopy and PET/CT examination at our clinic for staging purposes during a two-year period were retrospectively reviewed. Among the 71 patients who underwent TBNA during the study period, 45 also underwent PET/CT. Of these patients, 37 diagnosed with NSCLC [26 (70%) patients with squamous cell carcinoma, 11 (30%) with adenocarcinoma] were included (mean age, 59 ± 9 years; 34 males, 3 females). The remaining eight patients had malignancies other than NSCLC. The study protocol was approved by our institutional ethics committee. Bronchoscopy Bronchoscopy and TBNA were performed under local anesthesia and sedation, using a standard videobronchoscope (EB-270T; Fujinon Europe, Willich, Germany). The indication for TBNA was the presence of a significantly enlarged mediastinal lymph node (≥ 1 cm in diameter) upon CT of the chest. The procedure was performed for the right paratracheal, left paratracheal, and subcarinal lymph nodes [10]. When the patient showed an N3 lymph node upon thorax CT, the N3 lymph node was sampled before N2 nodes. To avoid false positive TBNA results, the procedure was done as an initial step, prior to the observation of distal airways and other conventional biopsy techniques (e.g. brushing, endobronchial biopsy, or transbronchial lung biopsy). All TBNA samples were obtained using a 22-gauge Wang needle (MW-122; Bard Endoscopic Technologies, Billerica, USA). TBNA aspirates were smeared on slides and placed in 95% ethanol. As a pathologist was not present during the bronchoscopy procedure, the adequacy of the material was initially evaluated by the physician performing the bronchoscopy. The same physician performed all bronchoscopies and TBNAs. All preparations were then examined by the same pathologist, who was blind to patient data. Materials obtained by TBNA were classified as either adequate or inadequate. Preparations with a definitive diagnosis of malignancy were defined as “adequate-positive”, preparations with abundant amounts of lymphocytes but no evidence of malignancy were defined as “adequate-negative”, and suspicious preparations having bronchial epithelia or cellular atypia were deemed inadequate samples. BT Uskul, V Baysungur, F Aksoy, FE Turan, G Sevilgen, H Turker, S Halezeroglu TBNA and PET/CT for mediastinal staging of NSCLC - Stadiazione N mediastinica nel NSCLC Conclusioni. I nostri risultati dimostrano che la combinazione della TBNA convenzionale, una procedura minimamente invasiva eseguibile nel corso di esami broncoscopici routinari, con la PET/CT, esame non invasivo, fornisce un'elevata accuratezza per la stadiazione linfonodale mediastinica del NSCLC. PET/CT PET/CT scans were performed using a multi-detector CT integrated high-resolution PET/CT scanner (Siemens Biograph LSO HI-RES Integrated PET/CT Scanner; Siemens Medical Solutions, Knoxville, USA) 60 min after an intravenous injection of 18 F-fluoro-2-deoxyglucose (FDG), at a dose of 5 MBq/kg body weight. To minimize insulin activity, patients were required to fast for a minimum of 12 h prior to the administration of FDG. The CT comMRM 9 Multidisciplinary Respiratory Medicine 2009; 4(1): 8-14 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 10 ponent of the procedure was performed without intravenous contrast and with low current (70 mA, 5mm section thickness), and was only used for the purpose of attenuation correction and assistance in the localization of PET images. Images were evaluated by two experienced nuclear medicine physicians, who were blind to the pathology results, and their consensus was classified as one of the following: negative, no typical uptake for malignancy (standard uptake value < 2.5); or positive, typical uptake for malignancy (standard uptake value ≥ 2.5). Surgical procedures Surgical decisions for pulmonary resection with mediastinoscopy and/or complete lymph node dissection in patients diagnosed with NSCLC were made at a weekly meeting of a multidisciplinary institutional panel consisting of pulmonologists, chest surgeons, pathologists, oncologists, and nuclear medicine specialists. Patients refusing or unsuitable for surgical intervention were not scheduled for surgery, but were referred to the Oncology Department to be evaluated for chemotherapy and/or radiotherapy. Patients with surgically resectable tumors and who were positive for N2 at a single station upon TBNA received neoadjuvant chemotherapy. Patients were re-evaluated after three courses of chemotherapy. Pulmonary resection with mediastinoscopy and/or complete lymph node dissection was performed in patients demonstrating regression. However, patients with extensive N2 disease (bulky disease or multiple N2-positive nodes) or N3 disease, as determined by TBNA, were considered inoperable. Statistical analyses For purposes of the statistical evaluation, all preparations positive for malignancy were considered “true positives,” because of the high specificity of the TBNA technique [1]. Among preparations negative for malignancy, only those confirmed with mediastinoscopy and/or mediastinal lymph node dissection were considered “true negatives.” All inadequate samples and “adequate-negative” preparations not confirmed by surgery were considered “false negatives.” FDG uptake results in mediastinal lymph nodes on PET/CT imaging were evaluated in the context of positive TBNA and surgical histopathology results. True positive, true negative, false negative, and false positive rates were also determined for PET/CT. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy were calculated for TBNA, PET/CT, and the combined use of TBNA and PET/CT. The chisquared test was used for the comparison of independent ratios, and the McNemar test was used for dependent ratios. Results were evaluated at 95% confidence intervals and p values < 0.05 were deemed to be statistically significant. 10 MRM RESULTS TBNA of mediastinal lymph nodes gave positive results for malignancy in 28 (76%) of 37 patients. Of these 28 patients, 10 were scheduled for neoadjuvant chemotherapy, because of the presence of N2 mediastinal lymph node involvement at a single station. These patients were reviewed after three courses of chemotherapy; 5 demonstrated regression and 5 showed progression. Of the 5 patients with regression, 2 underwent lung resections with complete lymph node dissection following mediastinoscopy, 2 underwent lung resection with complete lymph node resection, and the remaining patient underwent only mediastinoscopy. For the 5 progressing patients, systemic chemotherapy was continued. Of the 28 patients with positive TBNA results for malignancy, 16 (2 with N3 disease, 5 with multiple N2, 9 with bulky N2) were referred to the Oncology Department for systemic chemotherapy. Two other TBNA-positive patients were also referred to the Oncology Department for systemic chemotherapy and/or radical radiotherapy (one refusing surgery, one unsuitable for surgery). In 3 (8%) of 37 patients, TBNA of mediastinal lymph nodes was reported as adequate-negative. Following mediastinoscopy, these three patients had curative surgical resections, with mediastinal lymph node dissection. Histopathological examinations did not show malignant involvement. In 6 (16%) of 37 patients, TBNA of mediastinal lymph nodes resulted in inadequate specimens. Four of these patients had curative surgical resections, with mediastinal lymph node dissection, following mediastinoscopy; one had a curative surgical resection, with mediastinal lymph node dissection. The remaining patient refused to undergo a curative surgical resection; thus, no histopathological diagnosis of mediastinal lymph nodes could be obtained. The distribution of the 37 NSCLC patients who underwent TBNA of mediastinal lymph nodes is shown in Figure 1. TBNA results and comparison to surgical histology TBNA of 49 mediastinal lymph nodes was performed in 37 patients, and adequate samples were obtained from 41 (83%) lymph nodes. Thirty-five (71%) TBNA samples were positive for malignancy, 6 (12%) were negative, and 8 (16%) were inadequate for examination (Figure 2). Of the 35 TBNApositive lymph nodes, 5 were surgically confirmed following neoadjuvant chemotherapy. Four of 6 negative lymph nodes were confirmed surgically. Five of the 8 nodes with inadequate aspiration samples were surgically evaluated: 4 were negative for malignancy and 1 was positive. The examination of 49 lymph node aspirations yielded the following results: 35 true positives, 4 true negatives, and 10 false negatives. Thus, the sensitivity, specificity, PPV, NPV, and accuracy of mediastinal lymph node TBNA were 78% (35/45), 100% (4/4), 100% (35/35), 29% (4/14) and 80% (39/49), respectively. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 11 NSCLC patients (n = 37) TBNA-positive (n = 28) NC N2 positive (n = 10) Surgery M (n = 1) M + T (n = 2) T (n = 2) C Multiple N2 (n = 5) Bulky N2 (n = 9) N3 positive (n = 2) C/R Rejected surgery (n = 1) Not fit for surgery (n = 1) TBNA-negative (n = 3) TBNA-inadequate (n = 6) Surgery M + T (n = 3) Surgery M + T (n = 4) T (n = 1) Rejected surgery (n = 1) C Progression (n = 5) Definition of abbreviations: C, chemotherapy; M, mediastinoscopy; NC, neoadjuvant chemotherapy; R, radiotherapy; T, thoracotomy with complete lymph node dissection. Comparison of pathological examination results with integrated PET/CT PET/CT demonstrated FDG uptake in 84 mediastinal lymph nodes (52 positive for malignancy, 32 negative for malignancy) in 37 patients. Of these 84 nodes, a final pathological diagnosis was obtained in 78 (93%; Figure 3). The sensitivity of PET/CT scanning was 35/40 (88%), its specificity was 25/38 (66%), its PPV was 35/48 (73%), its NPV was 25/30 (83%), and its accuracy was 60/78 (77%). Upon PET/CT imaging, 25% of mediastinal lymph nodes positive for malignancy were false positives. When TBNA was performed for 6 of the 13 false BT Uskul, V Baysungur, F Aksoy, FE Turan, G Sevilgen, H Turker, S Halezeroglu TBNA and PET/CT for mediastinal staging of NSCLC - Stadiazione N mediastinica nel NSCLC FIGURE 1: OVERVIEW OF 37 NON-SMALL CELL LUNG CANCER (NSCLC) PATIENTS UNDERGOING MEDIASTINAL TRANSBRONCHIAL NEEDLE ASPIRATION (TBNA) FOR LYMPHADENOPATHY FIGURE 2: TRANSBRONCHIAL NEEDLE ASPIRATION (TBNA) RESULTS OF 49 LYMPH NODES IN 37 PATIENTS TBNA samples (n = 49) TBNA-positive (n = 35) TBNA-negative (n = 6) Surgical histology# No surgical histology† (n = 5) (n = 30) Surgical histology (n = 4) Cancer (n = 3) No cancer‡ (n = 2) No cancer (n = 4) No surgical histology†† (n = 2) TBNA-inadequate (n = 8) Surgical histology (n = 5) No surgical histology‡‡ (n = 3) Cancer (n = 1) No cancer (n = 4) # Five TBNA-positive nodes from five patients were surgically evaluated following neoadjuvant chemotherapy. TBNA positive for lymph node involvement, subsequently yielded negative results upon curative resection after neoadjuvant chemotherapy (successful down staging). † Due to the high specificity of TBNA procedure, 30 lymph nodes with surgically unconfirmed positive results were accepted as malignant. †† Aspiration of subcarinal lymphadenopathy showed malignant involvement in the patient, with abundant lymphocytes on right paratracheal lymph node aspiration. Similarly, the patient with abundant lymphocytes on subcarinal lymph node aspiration had positive malignant involvement upon aspiration of right paratracheal lymphadenopathy. ‡‡ The patient with inadequate right paratracheal lymph node aspiration had malignant involvement of the subcarinal lymph node, and, similarly, the patient with inadequate subcarinal lymph node aspiration had positive left paratracheal lymphadenopathy aspiration. The patient with inadequate right paratracheal lymph node aspiration refused surgical intervention. ‡ MRM 11 Multidisciplinary Respiratory Medicine 2008; 4(1): 8-14 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 12 FIGURE 3: COMPARISON OF INTEGRATED POSITRON EMISSION TOMOGRAPHY/COMPUTED TOMOGRAPHY (PET/CT) AND PATHOLOGICAL EXAMINATION OF 84 LYMPH NODES IN 37 PATIENTS PET/CT versus pathology (n = 84) PET/CT positive (n = 52) Cancer (n = 35) No cancer (n = 13) PET/CT negative (n = 32) No pathological results (n = 4) positive lymph nodes on PET/CT imaging, 4 (67%) were true negatives (confirmed by surgery) and 2 had inadequate aspiration samples. Of the mediastinal lymph nodes with negative uptake for malignancy on PET/CT imaging, 16% were histologically confirmed to be false negatives. TBNA was done for 3 of 5 false negative lymph nodes on PET/CT imaging and all were positive for malignancy (100%). Relationship between histological tumor type and diagnostic yield of TBNA and PET/CT The diagnostic yield of TBNA of mediastinal lymph nodes was 96% (24/25) in squamous cell carcinoma and 100% (11/11) in adenocarcinoma. The diagnostic yield of PET/CT imaging of mediastinal lymph nodes was 86% (25/29) in squamous cell carcinoma and 91% (10/11) in adenocarcinoma. There was no significant relationship between histological type of tumors and the diagnostic yields of TBNA and PET/CT imaging of mediastinal lymph nodes (p > 0.05). Combined use of TBNA and PET/CT for the detection of malignant lymph nodes The combined sensitivity of TBNA and PET/CT for the detection of mediastinal lymph node involvement was 38/45 (84%), specificity was 29/38 (76%), PPV was 38/47 (81%), NPV was 29/36 (81%), and accuracy was 67/83 (81%). No statistically significant difference was found between the sensitivity, specificity, and diagnostic accuracy rates of TBNA and PET/CT. TBNA had a higher PPV and a lower NPV compared to PET/CT (chisquared test, p = 0.001, p = 0.001, respectively). The combined use of TBNA and PET/CT had significantly higher diagnostic accuracy for the detection of malignant lymph node involvement compared to PET/CT alone (81% versus 77%, McNemar test, p = 0.016). Effectiveness of TBNA alone, PET/CT alone, and combined use of TBNA and PET/CT in nodal staging of NSCLC Nodal stages of the 37 NSCLC patients were as fol- 12 MRM No cancer (n = 25) Cancer (n = 5) No pathological results (n = 2) lows: N0, 6 patients; N2, 28 patients; N3, 2 patients. Nodal staging based on pathological examination could not be performed in the patient who refused surgical intervention. TBNA provided correct nodal staging in 30 patients (N0, 2 patients; N2, 26 patients; N3, 2 patients). TBNA samples were inadequate in 6 patients. In the remaining patient with a left upper lobe tumor, a TBNA sample obtained from left paratracheal area had abundant lymphocytes. This patient underwent mediastinoscopy and lung resection, with complete lymph node dissection. Pathological examination revealed malignant involvement of the subaortic lymph node; however, the left paratracheal lymph node did not have malignant involvement. This patient was correctly staged via PET/CT. The diagnostic accuracy of TBNA in nodal staging was 81%. PET/CT provided correct nodal staging in 29 patients (N0, 1 patient; N2, 27 patients; N3, 1 patient). Five patents with pathological staging of N0 had an up-stage on PET/CT (N1, 1 patient; N2, 2 patients; N3, 2 patients). Two patients were down-staged from N2 and N3 to N0 based on PET/CT. One patient without pathological nodal staging was excluded from the analysis. The diagnostic accuracy of PET/CT was 81% for nodal staging. Although the diagnostic accuracy of nodal staging increased to 92% when TBNA and PET/CT were combined, the resulting increase was not statistically significantly different from TBNA or PET/CT alone (McNemar test, p > 0.05). DISCUSSION Our results demonstrate that the combined use of TBNA and PET/CT is more effective for the identification of malignant involvement in the mediastinal lymph nodes of NSCLC patients. TBNA had a sensitivity of 78%, specificity of 100%, and accuracy of 80%. The corresponding figures for PET/CT were 88, 66, and 77%, respectively. When our results are interpreted in the context of mediastinal nodal staging, the combined use of TBNA and PET/CT had a diagnostic accuracy of 92%. FDG-PET is an imaging method providing biologi- MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 13 reasons for considering contamination unlikely during the TBNA process. First, the bronchial mucosa was normal at the site of needle puncture. The likelihood of contamination was low, as the lymph nodes are adjacent to the bronchial wall. Second, the TBNA procedure was performed as an initial step, prior to the observation of distal airways and the application of other conventional biopsy techniques. These factors make it unlikely that our TBNA results were false positives; nevertheless, the possibility cannot be excluded. The average NPV of TBNA for lymph nodes is reported to be 71% [7]. In our study, all inadequate and adequate-negative preparations that were not confirmed surgically were deemed false negatives, which may account for our low NPV for TBNA (29%). According to recent studies, PET/CT is superior to PET in the staging of NSCLC [12,22]. Yasufuku et al. [19] compared PET and EBUS-TBNA in the nodal staging of lung cancer. They reported 80% sensitivity, 70% specificity, and 73% diagnostic accuracy for PET, whereas the corresponding figures for EBUS-TBNA were 92, 100, and 98%, respectively. The present study found 88% sensitivity, 66% specificity, and 77% accuracy for PET/CT, with corresponding rates of 78, 100, and 80%, respectively, for TBNA. Gupta et al. [16] reported 13% false positive and 9% false negative rates for PET/PDG imaging in the identification of metastatic lymph nodes in lung cancer patients. For PET/CT, we obtained 25% false positive and 16% false negative rates. Abundant amounts of lymphocytes were observed in TBNA preparations obtained from the four lymph nodes that gave false positive results with PET/CT. These lymph nodes were confirmed to be true negatives via mediastinoscopy. Pathological examination of TBNA specimens from the three mediastinal lymph nodes that were negative for malignancy on PET/CT examination revealed the presence of NSCLC metastasis. The mean diameter of these three lymph nodes was 10 ± 0.1 mm, which may account for the observed false negative results via PET/CT. Our results suggest that the two procedures complement each other. In a study by Halpern et al. [6], when nodal staging was considered, PET/CT resulted in correct staging in 78% of cases, down-staging in 11%, and up-staging in 11%. In that study, false positive PET/CT results were due to granulomatous diseases and anthracosis, and the authors attributed false negative results to the small size of nodes (< 1 cm) [6]. Similarly, PET/CT resulted in correct nodal staging in 81% of cases, whereas down-staging and upstaging noted in 5 and 14%, respectively, of our cases. A major limitation of TBNA is that it does not provide access to some parts of the mediastinum. Although all mediastinal lymph nodes accessible via standard cervical mediastinoscopy can also be sampled by TBNA, the subaortic and paraesophageal lymph nodes (stations 5, 6, 8, and 9) BT Uskul, V Baysungur, F Aksoy, FE Turan, G Sevilgen, H Turker, S Halezeroglu TBNA and PET/CT for mediastinal staging of NSCLC - Stadiazione N mediastinica nel NSCLC cal information through the evaluation of tissue glucose metabolism, and is significantly superior to CT in the diagnosis of malignant involvement of mediastinal lymph nodes and distant metastases. Among the disadvantages of PET are its inability to demonstrate metastases in small lymph nodes, because of its poor spatial resolution, and its inability to differentiate lymph node involvement due to causes other than cancer from true tumor metastases [11]. Another disadvantage of PET is the low quality of the anatomical information it provides. Thus, for accurate localization of lesions, fusion software loading and overlapping PET images and radiological images on the same computer have been developed; however, these methods still provide limited accuracy. As a result, integrated PET/CT scanners have been developed [12]. Although PET has significant efficacy in the demonstration of extrathoracic metastases, varying results have been reported for its role in the demonstration of malignant lymph node involvement. Gupta et al. [13] reported 95% accuracy for PET in demonstrating malignant involvement of lymph nodes. However, subsequent studies did not confirm these findings. In the study of Gonzalez-Stawinski et al. [14], the sensitivity, specificity, PPV, and NPV of PET were 64, 77, 44, and 88%, respectively, in a sample of 202 patients. In a recent study, similar results were obtained: sensitivity 74%, specificity 73%, false positivity 26%, false negativity 25%, and diagnostic accuracy 74% [15]. Although PET/CT is a successful imaging modality for the demonstration of malignant nodal involvement and distant metastases in NSCLC patients, inflammatory changes at the lymph nodes may cause FDG accumulation, leading to false positive results. Thus, FDG uptake is not tumor-specific and is frequently observed in inflammatory lesions and benign conditions. False positive FDG uptake is common in granulomatous inflammation, silicosis, tuberculosis, histoplasmosis, and certain fungal inflammations [16-18]. Thus, false positive results from mediastinal examinations are frequent and histological confirmation should be performed before rejecting any surgical procedure [4,16,19]. Conventional TBNA is a minimally invasive technique that can be performed during diagnostic bronchoscopy and it may eliminate the need for more invasive mediastinal staging procedures [9]. Conventional TBNA can access all mediastinal lymph nodes accessible via endobronchial ultrasound-guided (EBUS)-TBNA. Additionally, conventional TBNA is a blind procedure, with varying yield rates [20]. Herth et al. [21] compared EBUS-TBNA and conventional TBNA, and found higher yield rates with EBUS-TBNA. There is always a possibility of getting false positive results from airway biopsies. Nevertheless, when cytological and/or histological preparations are positive for malignancy, it is reliable to accept this as a “true positive” [19]. False positive results are usually due to contamination occurring during the TBNA procedure. In our study, there were several MRM 13 Multidisciplinary Respiratory Medicine 2009; 4(1): 8-14 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 14 cannot be reached by this method. If PET/CT demonstrates positive uptake at subaortic and paraesophageal lymph nodes, endoscopic ultrasound-fine needle aspiration (EUS-FNA) or thoracoscopic examination of these nodes is recommended [23]. In the present study, the diagnoses of two inoperable patients were established by TBNA (N3, metastasis at the contralateral lymph node), eliminating the need for further diagnostic procedures. Our findings are noteworthy as they demonstrate the feasibility of the combined use of PET/CT (a non-invasive procedure) and conventional TBNA (a minimally invasive procedure that can be performed during routine bronchoscopy) for the nodal staging of NSCLC. Bernasconi et al. [24] demonstrated increased diagnostic accuracy with the combined use DICHIARAZIONE DI CONFLITTO DI INTERESSI: None of the authors has any conflict of interest to declare in relation to the subject matter of this manuscript. References 1. Patelli M, Agli LL, Poletti V, Trisolini R, Cancellieri A, Lacava N, Falcone F, Boaron M. Role of fiberscopic transbronchial needle aspiration in the staging of N2 disease due to nonsmall cell lung cancer. Ann Thorac Surg 2002;73:407-411. 2. Elias AD, Skarin AT, Leong T, Mentzer S, Strauss G, Lynch T, Shulman L, Jacobs C, Abner A, Baldini EH, Frei E 3rd, Sugarbaker DJ. Neoadjuvant therapy for surgically staged IIIA N2 non-small cell lung cancer (NSCLC). Lung Cancer 1997;17:147-161. 3. Toloza EM, Harpole L, McCrory DC. Noninvasive staging of non-small cell lung cancer: a review of the current evidence. Chest 2003;123:137S-146S. 4. Antoch G, Stattaus J, Nemat AT, Marnitz S, Beyer T, Kuehl H, Bockisch A, Debatin JF, Freudenberg LS. Non-small cell lung cancer: dual-modality PET/CT in preoperative staging. Radiology 2003;229:526-533. 5. Piet AH, Lagerwaard FJ, Kunst PW, van Sörnsen de Koste JR, Slotman BJ, Senan S. Can mediastinal nodal mobility explain the low yield rates for transbronchial needle aspiration without real-time imaging? Chest 2007;131:1783-1787. 6. Halpern BS, Schiepers C, Weber WA, Crawford TL, Fueger BJ, Phelps ME, Czernin J. Presurgical staging of non-small cell lung cancer: positron emission tomography, integrated positron emission tomography/CT, and software image fusion. Chest 2005;128:2289-2297. 7. Toloza EM, Harpole L, Detterbeck F, McCrory DC. Invasive staging of non-small cell lung cancer: a review of the current evidence. Chest 2003;123(Suppl.1):157S-166S. 8. Holty JE, Kuschner WG, Gould MK. Accuracy of transbronchial needle aspiration for mediastinal staging of nonsmall cell lung cancer: a meta-analysis. Thorax 2005;60:949-955. 9. Pretreatment evaluation of non-small-cell lung cancer. The American Thoracic Society and The European Respiratory Society. Am J Respir Crit Care Med 1997;156:320-332. 10. Wang KP. Staging of bronchogenic carcinoma by bronchoscopy. Chest 1994;106:588-593. 11. De Leyn P, Lardinois D, Van Schil PE, Rami-Porta R, Passlick B, Zielinski M, Waller DA, Lerut T, Weder W. ESTS guidelines for preoperative lymph node staging for non-small cell lung cancer. Eur J Cardiothorac Surg 2007;32:1-8. 12. Lardinois D, Weder W, Hany TF, Kamel EM, Korom S, Seifert B, von Schulthess GK, Steinert HC. Staging of non-smallcell lung cancer with integrated positron-emission tomography and computed tomography. N Engl J Med 2003; 348:2500-2507. 13. Gupta NC, Graeber GM, Bishop HA. Comparative efficacy 14 MRM of TBNA and PET imaging in the mediastinal staging of NSCLC. In the same study, patients with negative PET and TBNA results for enlarged mediastinal lymph nodes were confirmed to be operable. In conclusion, the combined use of TBNA and PET/CT in the nodal staging of NSCLC provides the following benefits to clinicians. First, identifying N3 lymph nodes during diagnostic bronchoscopy may decrease the need for a mediastinoscopy. Second, TBNA may give positive results in enlarged lymph nodes that give false negative results by PET/CT. Finally, the combined use of TBNA and PET/CT can provide 92% accuracy for nodal staging. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. of positron emission tomography with fluorodeoxyglucose in evaluation of small (< 1 cm), intermediate (1 to 3 cm), and large (> 3 cm) lymph node lesions. Chest 2000; 117:773-778. Gonzalez-Stawinski GV, Lemaire A, Merchant F, O'Halloran E, Coleman RE, Harpole DH, D'Amico TA. A comparative analysis of positron emission tomography and mediastinoscopy in staging non-small cell lung cancer. J Thorac Cardiovasc Surg 2003;126:1900-1905. Melek H, Gunluoglu MZ, Demir A, Akin H, Olcmen A, Dincer SI. Role of positron emission tomography in mediastinal lymphatic staging of non-small cell lung cancer. Eur J Cardiothorac Surg 2008;33:294-299. Gupta NC, Tamim WJ, Graeber GG, Bishop HA, Hobbs GR. Mediastinal lymph node sampling following positron emission tomography with fluorodeoxyglucose imaging in lung cancer staging. Chest 2001;120:521-527. Valk PE, Pounds TR, Hopkins DM, Haseman MK, Hofer GA, Greiss HB, Myers RW, Lutrin CL. Staging non-small cell lung cancer by whole-body positron emission tomographic imaging. Ann Thorac Surg 1995;60:1573-1581. Dewan NA, Gupta NC, Redepenning LS, Phalen JJ, Frick MP. Diagnostic efficacy of PET-FDG imaging in solitary pulmonary nodules. Potential role in evaluation and management. Chest 1993;104:997-1002. Yasufuku K, Nakajima T, Motoori K, Sekine Y, Shibuya K, Hiroshima K, Fujisawa T. Comparison of endobronchial ultrasound, positron emission tomography, and CT for lymph node staging of lung cancer. Chest 2006;130:710-718. Bilaceroglu S, Chhajed P. Transbronchial needle aspiration: a diagnostic tool in routine bronchoscopy. J Assoc Physicians India 2005;53:797-802. Herth F, Becker HD, Ernst A. Conventional vs endobronchial ultrasound-guided transbronchial needle aspiration: a randomized trial. Chest 2004;125:322-325. Hsu LH, Ko JS, You DL, Chu NM. Transbronchial needle aspiration guided by integrated positron emission tomography and computed tomography: a preliminary report. J Bronchol 2005;12:76-80. Herth FJ, Lunn W, Eberhardt R, Becker HD, Ernst A. Transbronchial versus transesophageal ultrasound-guided aspiration of enlarged mediastinal lymph nodes. Am J Respir Crit Care Med 2005;171:1164-1167. Bernasconi M, Chhajed PN, Gambazzi F, Bubendorf L, Rasch H, Kneifel S, Tamm M. Combined transbronchial needle aspiration and positron emission tomography for mediastinal staging of NSCLC. Eur Respir J 2006;27:889-894. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 15 Documento ufficiale / Official statement La cessazione del fumo in pazienti con malattie respiratorie: alta priorità, componente integrante della terapia Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy Laura Carrozzi1, Carlo Lazzaro2, Stefano Nardini3, Francesco Pistelli3, Patrizia Silvi4, Giovanni Viegi4 1 Dipartimento Cardiotoracico, Azienda Ospedaliero-Universitaria Pisana, Pisa Consulente di Economia Sanitaria, Milano 3 UO di Pneumotisiologia, Ospedale di Vittorio Veneto, TV, ULSS 7 Sinistra Piave, Regione Veneto 4 Istituto di Fisiologia Clinica CNR, Pisa. 2 Traduzione del documento prodotto dalla ERS Task Force on Smoking Cessation: “Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy. P Tønnesen, L Carrozzi, KO Fagerström, C Gratziou, C Jimenez-Ruiz, S Nardini, G Viegi, C Lazzaro, IA Campbell, E Dagli, R West. Eur Respir J 2007;29:390-417.” Il testo tradotto è stato messo a disposizione per la diffusione attraverso il sito dell'Istituto Superiore di Sanità. RIASSUNTO La cessazione del fumo è uno dei mezzi più importanti per migliorare la prognosi dei pazienti con malattie respiratorie. La Task Force sulle linee guida per la cessazione del fumo nei pazienti con malattie respiratorie è stata costituita per fornire raccomandazioni basate sull'evidenza per gli interventi di cessazione del fumo in pazienti respiratori. Basandosi sulle evidenze scientifiche attualmente disponibili e sul consenso di un panel di esperti, sono state fornite le seguenti raccomandazioni: 1) i pazienti con malattie respiratorie hanno una maggiore e più urgente necessità di smettere di fumare rispetto alla media dei fumatori, quindi gli spe- cialisti in malattie dell'apparato respiratorio devono avere un ruolo attivo e continuativo per tutti i fumatori, nel motivarli a smettere e nel fornire loro trattamenti che li aiutino a cessare il fumo; 2) il trattamento per la cessazione del fumo dovrebbe essere parte integrante della gestione dei pazienti con malattie respiratorie; 3) le terapie dovrebbero includere trattamenti farmacologici (es. terapia con sostituti alla nicotina, bupropione o vareniclina) in combinazione con un supporto comportamentale; 4) i medici pneumologi dovrebbero ricevere adeguata formazione per assicurarsi di avere la conoscenza, l'attitudine e gli strumenti necessari per dispensare questi interventi o per indirizzare i pazienti ad un adeguato + Laura Carrozzi Dipartimento Cardio-Toracico, Azienda Ospedaliero-Universitaria Pisana Via Roma 67, 56126 Pisa, Italia email: [email protected] Nota: Testo tradotto e messo a disposizione per la diffusione attraverso il sito dell'Istituto Superiore di Sanità, come da permesso ottenuto dalla European Respiratory Society Journals Ltd in data 7/11/2007 (ref. PMM016-2007). “This Italian translation has been reproduced with the permission of the European Respiratory Society. The translation has not been reviewed by the ERS prior to publication, therefore the ERS may not be responsible for any errors, omissions or inaccuracies, or any consequences arising there from, in the Italian content / “La presente traduzione in italiano è stata riprodotta con l'autorizzazione di European Respiratory Society. La traduzione non è stata rivista dall'ERS prima della pubblicazione, quindi l'ERS non può essere responsabile per qualsiasi errore, omissione o inaccuratezza, oppure per qualsiasi conseguenza che ne possa derivare, nel contenuto in italiano. Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 15 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 16 specialista in materia; 5) benché il costo della messa in opera di queste raccomandazioni sia in parte compensato dalla riduzione nella comparsa di riacutizzazioni, etc., un budget dovrebbe essere destinato a permetterne l'implementazione. Ulteriori ricerche sono necessarie per stabilire le strategie ottimali di trattamento specificamente rivolti a pazienti respiratori. Parole chiave: Broncopneumopatia cronica ostruttiva, linee guida, pazienti respiratori, cessazione del fumo. ABSTRACT Smoking cessation is one of the most important ways to improve the prognosis of patients with respiratory disease. The Task Force on guidelines for smoking cessation in patients with respiratory diseases was convened to provide evidence-based recommendations on smoking cessation interventions in respiratory patients. Based on the currently available evidence and the consensus of an expert panel, the following key recommendations were made: 1) patients with respiratory disease have a greater and more urgent need to stop smoking than the average smoker, so respiratory physicians must take a proactive and continuing role with all smokers in motivating them to stop and in providing treatment to aid smoking cessation; 2) smoking cessation treatment should be integrated into the management of the patient's respiratory condition; 3) therapies should include pharmacological treatment (i.e. nicotine replacement therapy, bupropion or varenicline) combined with behavioural support; 4) respiratory physicians should receive training to ensure that they have the knowledge, attitudes and skills necessary to deliver these interventions or to refer to an appropriate specialist; 5) although the cost of implementing these recommendations will partly be offset by a reduction in attendance for exacerbations, etc., a budget should be established to enable implementation. Research is needed to establish optimum treatment strategies specifically for respiratory patients. Keywords: Chronic obstructive pulmonary disease, guidelines, respiratory patients, smoking cessation. INDICE Introduzione 17 Punti chiave delle raccomandazioni 17 Dipendenza da tabacco / tossicodipendenza da nicotina 18 Fumo di tabacco Dipendenza da tabacco Definizione della dipendenza da tabacco Epidemiologia delle malattie respiratorie fumo-correlate 19 Fumo di tabacco: la dimensione del problema Tumore polmonare BPCO Fumo e sintomi respiratori Fumo e funzione respiratoria Fumo ed altre malattie respiratorie Valutazione 22 Abitudine al fumo Motivazione a smettere Dipendenza Precedenti esperienze di cessazione del fumo Monossido di carbonio 16 MRM Spirometria e cessazione del fumo Comorbosità Caratteristiche dei pazienti respiratori 24 che fumano Perché i pazienti respiratori sono un target difficile Auto-medicazione per le comorbosità Dipendenza Pattern di inalazione del fumo Controllo del peso Interventi psicologici e comportamentali 26 Programmi di auto-aiuto Consiglio breve Counselling Terapia comportamentale Procedure per interventi psicologici e comportamentali nella cessazione del fumo Interventi psicologici e comportamentali in pazienti con malattie respiratorie che fumano Trattamenti farmacologici per la cessazione del fumo 29 Trattamenti di prima linea Trattamenti di seconda linea Nuovi farmaci Punti chiave: farmacoterapia e disassuefazione dal fumo Altri interventi 35 Agopuntura e laser terapia Ipnosi La riduzione del fumo 35 Definizione Studi di popolazione Studi randomizzati controllati di riduzione assistita del fumo Riduzione del danno Implementazione della riduzione del fumo Struttura organizzativa e formazione 37 Identificazione sistematica dei fumatori Attrezzatura ed organico Formazione Strutture sanitarie libere dal fumo Costi del tabagismo ed aspetti economici degli interventi finalizzati alla disassuefazione dal fumo di sigaretta 38 Costo delle patologie fumo-correlate Analisi costo-efficacia degli interventi di disassuefazione dal tabagismo Cessazione del fumo e condizione socio-economica del paziente Cessazione del fumo ed “elasticità al prezzo” dei fumatori di sigarette Punti chiave Prospettive di ricerca 40 Ringraziamenti 41 Bibliografia 41 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 17 Il fumo di tabacco è un importante determinante per le malattie polmonari; esso rappresenta il maggior fattore etiologico per lo sviluppo di Bronco Pneumopatia Cronica Ostruttiva (BPCO) e tumore polmonare, e peggiora il controllo dell'asma [1]. Queste malattie costituiscono una parte consistente dell'impatto sulla mortalità e sulla morbosità attribuibili a patologie respiratorie in Europa, ma il fumo di tabacco è strettamente correlato anche ad altre malattie respiratorie, quali la polmonite e la tubercolosi (TB). Il fumo, infine, contribuisce alla progressione di alcune malattie respiratorie più rare, quali il deficit di alfa1-antitripsina e l'istiocitosi X. La cessazione del fumo è il più importante intervento sulla BPCO ed uno degli obiettivi fondamentali di questa Task Force della Società Europea Respiratoria (ERS) sulle linee guida per la cessazione del fumo nei pazienti con malattie respiratorie è garantire che i medici pneumologi agiscano per assicurare che i pazienti con BPCO ed altre malattie respiratorie smettano di fumare. Incoraggiare e supportare la cessazione del fumo sembra rivestire una bassa priorità per i medici pneumologi, anche se questo intervento possiede un alto rapporto costo-efficacia ed è il solo intervento in grado di ridurre il rischio di sviluppare BPCO e di rallentarne la progressione [2-4]. La cessazione del fumo dovrebbe essere parte integrante di ogni servizio di pneumologia ed ogni medico pneumologo dovrebbe avere un appropriato livello di conoscenza sulle tematiche della cessazione del fumo. La cessazione del fumo dovrebbe essere componente integrante dei programmi di riabilitazione per i pazienti con BPCO. Uno studio di riferimento, il Lung Health Study, ha arruolato 5887 fumatori con BPCO di grado lieve ed ha effettuato ripetuti interventi di cessazione del fumo per un periodo di 5 anni [5]. Il tasso di cessazione dopo 5 anni era di circa il 35%, dato che rappresenta un incoraggiante risultato. Altri studi hanno riportato valori di cessazione nei pazienti con BPCO più bassi rispetto a quelli ottenuti nei fumatori “sani”, sottolineando la presenza di maggiori ostacoli alla cessazione del fumo nei pazienti con BPCO e la necessità di maggiori sforzi per indurre questi pazienti a smettere di fumare [6-8]. Numerose linee guida per la cessazione del fumo sono state pubblicate negli anni recenti. Probabilmente le più conosciute e più largamente usate sono quelle redatte dall'Agenzia per le Politiche Sanitarie e la Ricerca Clinica Statunitense (US Agency for Health Care Policy and Reasearch's Clinical Practice Guidelines for Treating Tabacco Use and Dependence), pubblicate nel 1996 [9] e aggiornate nel 2000 [10,11]. Queste linee guida sono basate principalmente su metanalisi di 6000 studi, che includono molti studi clinici controllati volti al trattamento del tabagismo in fumatori sani, così come in popolazioni particolari, quali le donne in gravidanza, i fumatori ricoverati, i ragaz- zi, gli adolescenti ed i fumatori anziani. In accordo a queste linee guida, l'American College of Chest Physicians ha pubblicato nel 2002 un position paper [12], che evidenzia le strategie chiave e le raccomandazioni per gli pneumologi. L'ERS ha pubblicato un position paper sulla cessazione del fumo nel 1995 [13]. L'American Psychiatric Association (APA) ha pubblicato linee guida nel 1996 [14], basate su metanalisi e rivolte principalmente agli psichiatri; comunque, queste linee guida possono essere utili per tutti i medici che trattano i pazienti con dipendenza da nicotina. Poiché le linee guida esistenti per la cessazione del fumo hanno un carattere generalista, le presenti raccomandazioni sono rivolte in particolare ai pazienti con malattie respiratorie, al fine di definire comportamenti standardizzati in questo settore e di aumentare l'implementazione della cessazione del fumo in questa specifica popolazione. A causa della mancanza di evidenze scientifiche in merito alla cessazione del fumo nei pazienti respiratori, numerose raccomandazioni individuate da questa Task Force non sono basate sui risultati di studi clinici controllati, ma piuttosto sull'opinione di esperti derivante dalla pratica clinica di molti anni di lavoro nel campo della cessazione del fumo sia su fumatori sani sia su pazienti con malattie respiratorie. Le raccomandazioni sono classificate in base alla forza dell'evidenza scientifica, secondo la seguente graduazione: A) molti studi clinici randomizzati (RCT), ben disegnati; B) alcune evidenze da RCT, ma non ottimali, per esempio a causa di differenti popolazioni in studio; C) non esistenza di RCT, ma evidenza basata su dati pubblicati o sull'opinione degli esperti. I più importanti obiettivi di questa Task Force ERS sono: 1) presentare raccomandazioni per la cessazione del fumo indirizzate ai pazienti con malattie respiratorie; 2) incrementare l'implementazione dei servizi di cessazione del fumo nelle unità operative di pneumologia; e 3) stimolare la ricerca in quest'area. Per limitare la lunghezza di questo documento non sono stati considerati gli effetti del fumo passivo. È stata anche omessa la trattazione delle strategie di prevenzione, che giocano un ruolo integrante per la riduzione degli effetti avversi sulla salute derivanti dalla pandemia del fumo di tabacco. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement INTRODUZIONE PUNTI CHIAVE DELLE RACCOMANDAZIONI I punti chiave di questo documento sono: 1. I pazienti con malattie respiratorie hanno un più grande e più urgente bisogno di smettere di fumare rispetto alla media dei fumatori. Essi dovrebbero essere incoraggiati a smettere, ma molto spesso questo è per loro più difficile (livello di evidenza B). 2. I medici pneumologi devono avere un ruolo proattivo e continuo nei confronti di ogni fumatore nel motivarlo a smettere, fornire il trattamento MRM 17 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 18 per raggiungere la cessazione, indipendentemente dalla sua durata, e affrontare le ricadute quando queste accadano. Il trattamento per la cessazione del fumo deve essere considerato parte integrante della gestione di pazienti con malattie respiratorie. Lo schema di approccio comprende i seguenti punti: a) valutazione regolare dello stato di fumatore usando metodi che possano misurare obiettivamente il fumo, quali il test per il monossido di carbonio (CO) nell'espirato, (livello di evidenza C); b) trattamento farmacologico della dipendenza da nicotina, che comprende il bupropione e/o, quando necessario, alti dosaggi e/o l'uso prolungato di terapia sostitutiva nicotinica (NRT). Ciò può comprendere anche la combinazione di differenti forme di NRT (livello di evidenza A). La vareniclina è un farmaco promettente di seconda linea (livello di evidenza B); c) il supporto comportamentale, che dovrebbe essere intensivo, comprensivo di ripetute sedute, e fornito da personale opportunamente formato (livello di evidenza B) 3. Al fine di attuare con efficacia questo percorso, i medici pneumologi dovrebbero avere adeguate conoscenze e appropriate attitudini e capacità; questo richiede studio e formazione medica continua, che dovrebbe essere fornita secondo standard professionali e dovrebbe essere accreditata (livello di evidenza C). 4. Il costo di tale strategia sarà in parte compensato da una riduzione della presenza di riacutizzazioni etc., ma si dovranno comunque destinare finanziamenti per sostenere l'implementazione di protocolli di trattamento e per fornire farmaci e supporto comportamentale (livello di evidenza A). 5. È importante misurare regolarmente la funzione respiratoria al fine di monitorare l'evoluzione della malattia ed utilizzare tale valutazione come strumento motivazionale (livello di evidenza C). 6. Ai fumatori non motivati a smettere dovrebbe essere offerta NRT per ridurre la quantità di tabacco fumata e come tappa intermedia verso la cessazione (livello di evidenza B). 7. I fumatori non interessati a smettere o a ridurre dovrebbero essere avvertiti che il medico affronterà nuovamente la questione in una visita successiva. DIPENDENZA DA TABACCO / TOSSICODIPENDENZA DA NICOTINA Il fumo di tabacco contiene > 4000 differenti costituenti, che includono sostanze tossiche quali cancerogeni (N-nitrosamine, idrocarburi aromatici), ammoniaca, ossido di azoto, acido cianidrico, CO e nicotina [1]. La temperatura nella parte bruciante di una sigaretta è di circa 900°C, con una fase gassosa ed una fase particolata costituita da particelle di circa 0,2 µ (range 0,1-1,0 µ). I contenuti di CO e di catrame delle sigarette sono stati ridotti durante gli ultimi 10 anni, ma la determinazione della loro 18 MRM quantità effettuata utilizzando le macchine del fumo sottostima ampiamente i livelli di CO e catrame inalati dai fumatori [15]. Dipendenza da tabacco La dipendenza da tabacco è un comportamento complesso, con influenze ambientali e genetiche [16]. Il principale componente delle sigarette che determina dipendenza è la nicotina, benché anche fattori psicologici e abitudinari giochino un ruolo. La nicotina agisce su specifici recettori acetilcolinici ubicati nel cervello, stimolando il rilascio di dopamina che si ritiene associata agli effetti di rinforzo acuto della nicotina [17]. Il fumo cronico conduce ad una up regulation dei recettori nicotinici. Definizione della dipendenza da tabacco Nel 1988, il ministro della sanità americano (US Surgeon General) elaborò un rapporto intitolato “Tossicodipendenza da nicotina” [18]. Le principali conclusioni furono che le sigarette creano tossicodipendenza, che la nicotina è la componente del tabacco che causa tossicodipendenza e che la tossicodipendenza da tabacco è simile a quella da altre droghe come l'eroina e la cocaina [18]. La decima Classificazione Internazionale delle Malattie (ICD-10) dell'Organizzazione Mondiale della Sanità (OMS) classifica il fumo di tabacco all'interno del gruppo “Disordini mentali e comportamentali” come F17, Disordini mentali e comportamentali dovuti all'uso del tabacco [19]. Le sottodivisioni sono: F17.0, Intossicazione acuta; F17.1, Uso dannoso; F17.2, Sindrome da dipendenza; F17.3, Condizione di astinenza; F17.8, Altri disordini mentali e comportamentali; F17.9, Disordini mentali e comportamentali non specificati, e Z72.0, Uso del tabacco (che include F17.2, Dipendenza da tabacco). La categoria F17.2, Dipendenza da tabacco, può essere definita “come un insieme di fenomeni comportamentali, cognitivi e fisiologici che si sviluppano in seguito all'uso ripetuto e che tipicamente includono un forte desiderio di fumare, la difficoltà a controllarne l'uso, la persistenza nell'uso nonostante le conseguenze dannose, un'aumentata tolleranza alla nicotina, e una condizione (fisica) di astinenza. L'APA definisce la dipendenza da fumo di tabacco come tossicodipendenza da nicotina [20]. Approssimativamente, dopo 4-12 ore dalla cessazione del fumo, i sintomi di astinenza insorgono in grado variabile. Essi includono irritabilità, ansia, nervosismo, agitazione continua, disforia (o depressione), difficoltà a concentrarsi, “desiderio impellente” di fumare, aumento dell'appetito e disturbi del sonno. I sintomi, spesso, raggiungono il loro picco durante la prima settimana, quindi si riducono nell'arco di alcune settimane o mesi [21,22]. Il peso può aumentare di 2-3 Kg durante i primi tre mesi dalla cessazione. Le modalità di ricaduta dopo la cessazione del fumo sono comparabili a quelle della cessazione dell'uso di alcool o di eroina: la possibilità di rica- MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 19 EPIDEMIOLOGIA DELLE MALATTIE FUMO-CORRELATE Fumo di tabacco: la dimensione del problema Secondo la World Bank, nel 1995 si registravano nel mondo 1,1 miliardi di fumatori di età ≥ ai 15 anni (il 29% di tutta la popolazione; il 47% dei maschi, il 12% delle femmine) [23]. Si stima che questo numero sia destinato a salire ad 1,6 miliardi nel 2025 [23]. Durante il 2002-2003, la prevalenza media del fumo di sigaretta nell'Unione Europea (EU) è stata valutata del 29% (35% dei maschi e 22% delle femmine; Tabella I) [24,25]. Il fumo di sigaretta è la causa principale di molte malattie respiratorie ed uno dei fattori di rischio delle malattie cardiovascolari, tumori di vari organi e molte altre patologie [26,27]. Il peso delle malattie fumo correlate sulla società è enorme. È stato valutato che nel ventesimo secolo circa 100 milioni di persone sono state uccise dal fumo di tabacco e che il numero salirà ad un miliardo nel ventunesimo secolo [28]. In particolare dati recenti hanno dimostrato che nell'anno 2000 circa 4,83 milioni di morti nel mondo (il 12% della mortalità totale nel mondo stimata tra gli adulti di età ≥ 30 anni), erano attribuibili al fumo di tabacco e circa 2,43 milioni di questi in Paesi industrializzati (19% della mortalità totale di adulti) [29]. Le cause principali di morte da fumo di tabacco erano le malattie cardiovascolari (1,69 milioni di morti), BPCO (0,97 milioni), e cancro del polmone (0,85 milioni) [29]. Tra i 50 milioni di fumatori maschi nell'Unione Europea, ogni anno si registrano 500.000 morti attribuibili al fumo. Allo stesso tempo, tra i 35 milioni di fumatori femmine, si registrano annualmente circa 105.000 morti attribuibili all'abitudine al fumo [30]. Analizzando il follow up cinquantennale dei medici maschi inglesi, Doll e coll. [31] hanno concluso che i fumatori muoiono ad un'età di 10 anni più giovane rispetto a quella dei non fumatori. La cessazione a 60, 50, 40, o 30 anni permette di guadagnare rispettivamente circa 3, 6, 9, o 10 anni di aspettativa di vita [31]. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement duta è più alta durante le prime 3-6 settimane e quindi gradualmente si riduce [18]. Quindi, la dipendenza da tabacco / la tossicodipendenza da nicotina può essere considerata come una malattia o un disordine cronico recidivante, con un tasso di cessazione atteso dopo trattamento di 1535% dopo un anno, simile ad altri disturbi da dipendenza. Molti tentativi falliti di cessazione possono essere intrapresi prima di raggiungere l'astinenza definitiva. Comunque, anche se un fumatore riesce a smettere, la tossicodipendenza da nicotina rimane presente per molti anni come dimostrato dalle ricadute negli ex-fumatori che provano anche una sola sigaretta dopo alcuni anni dalla cessazione. Semplificando molto, la maggior parte dei fumatori che fumano più di 10 (o 15) sigarette al giorno e fumano la loro prima sigaretta entro un'ora dal risveglio sono significativamente dipendenti dal tabacco, cioè dalla nicotina. Tumore polmonare Diversi studi epidemiologici hanno dimostrato che il fumo di sigaretta è il fattore primario nel causare il tumore al polmone ed il conseguente decesso [31]. Nell'Unione Europea l'incidenza del tumore al polmone varia dall'8 al 62 per 100.000 persone, mentre la prevalenza varia dal 26 al 242 per 100.000 TABELLA I: PREVALENZA DELL'ABITUDINE AL FUMO NELL'UNIONE EUROPEA NEL PERIODO 2002-2003 (ECCETTO DOVE ESPRESSAMENTE INDICATO) Paese Fumatori totali % Fumatori % Fumatrici % Austria 29 32* 26* Belgio 27,5 33 22 Repubblica Ceca 30,5 38 23 Danimarca 27 30 24 Finlandia 22,5 26 19 Francia 30,5 36 25 Germania 32,5 37 28 Grecia 45 51§ 39§ Irlanda 27 28 26 Italia 26,2° 30° 22,5° Paesi Bassi 30 33 27 Polonia 31 39 23 Spagna 32 39 25 Svezia 25 26 24 Regno Unito 25 26 24 Media Unione Europea 29 35 22 Legenda:*, durante l'anno 2000; §, durante l'anno 2001; °, durante l'anno 2004 MRM 19 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 20 persone [32]. In Europa, l'indice di mortalità per tumore al polmone è aumentato del 58% tra il 1960 ed il 1988, ma è diminuito del 14% nel 1998, questo è dovuto principalmente al decrescere dell'incidenza e della mortalità nei maschi [33]. Al momento, il tumore al polmone è il più importante tumore killer in Europa che incide per circa il 20% su tutte le morti da tumore [33]. Comunque, Doll e coll. [31] hanno riscontrato che smettere di fumare a 50 anni dimezza il rischio di morte per tumore polmonare e molte altre patologie mentre smettere all'età di 30 elimina quasi del tutto il rischio [31]. È scientificamente dimostrato che la relazione esistente tra il fumo attivo ed il tumore polmonare è considerevole [27,34]. Sul rischio di sviluppare il tumore al polmone sembra influisca la durata nel tempo dell'abitudine al fumo attivo ed il numero di sigarette (o sigari, o pipe) fumate giornalmente [34]. Il rapporto dei rischi relativi di insorgenza del tumore polmonare tra i fumatori ed i non fumatori è di circa 15 complessivamente e circa 25 per i forti fumatori [31]. Comunque, molto recentemente, lo Studio di Prevenzione per il Tumore negli USA ha dimostrato che il numero degli anni di abitudine al fumo di tabacco influisce sul rischio di tumore molto più del numero di sigarette fumate giornalmente [35]. L'età in cui si inizia a fumare è un'altra caratteristica che influisce sull'aumento del rischio di tumore polmonare [34]. Il numero di pacchetti-anno (un indice illimitato definito come numero di sigarette fumate giornalmente per gli anni di fumo attivo/20), che prende in considerazione la durata ed il quantitativo di fumo attivo, è probabilmente la variabile più accurata per la valutazione della relazione tra il fumo attivo ed il tumore al polmone. In molti studi epidemiologici europei si è vista una tendenza all'aumento del rischio di tumore polmonare con l'aumento del numero di pacchetti-anno [36]. Smettere di fumare riduce il rischio di sviluppare il tumore al polmone rispetto a continuare a fumare: il rischio diminuisce sempre di più tanto più aumenta il periodo di astinenza dal fumo attivo. Comunque anche dopo lunghi periodi di astinenza per gli ex fumatori rimane più alto il rischio rispetto a quelli che non hanno mai fumato [27,32]. Fino dagli anni '80 è stato riscontrato nei fumatori un certo grado di suscettibilità genetica alla malattia [34]. Studi recenti sembrano indicare che, per lo sviluppo di tumore polmonare, le femmine sono più sensibili dei maschi ai cancerogeni contenuti nel fumo di tabacco [34]. BPCO Secondo l'OMS nel Global Burden of Disease study, la BPCO, che nel 1990 era la sesta causa principale di morte nel mondo, è previsto si collochi al terzo posto nel 2020 [37]. Nell'Unione Europea l'indice di mortalità dovuto alla BPCO è stimato due o tre volte superiore nei maschi che nelle femmine [38]. 20 MRM Nell'Unione Europea, i tassi di prevalenza di BPCO clinicamente rilevante, differiscono ampiamente tra i Paesi [38]. Indagini condotte in Europa hanno indicato che = 4-6% della popolazione adulta soffre di BPCO clinicamente rilevante, e la prevalenza aumenta nettamente con l'età [39]. Il fumo di sigaretta è il fattore di rischio più importante per la BPCO e può anche favorire l'inizio delle riacutizzazioni [40]. Da dati raccolti nei Paesi Europei è emerso che diagnosi autoriferite di bronchite cronica / enfisema [41] o segni spirometrici di ostruzione al flusso aereo [42] sono più frequenti nei fumatori che nei non fumatori. Il rischio di sviluppare BPCO può essere aumentato non solo dalla media di sigarette fumate giornalmente ma soprattutto dai pacchetti-anno accumulati [43]. Inoltre uno studio spagnolo ha dimostrato che i fumatori con BPCO consumano una quantità maggiore di tabacco, hanno livelli di CO più alti nell'aria espirata ed una dipendenza da nicotina maggiore dei fumatori sani [44]. Negli ultimi anni, molti studi hanno suggerito che le femmine potrebbero essere più suscettibili agli effetti nocivi del fumo di tabacco nello sviluppare BPCO [45]. Nel Copenhagen City Heart Study, la stima dell'eccesso di declino del volume espiratorio forzato nel primo secondo (FEV1) per pacchettoanno era di 7,4 mL nelle fumatrici e 6,3 mL nei fumatori. Le fumatrici avevano anche un rischio maggiore di ospedalizzazione per BPCO. Simili risultati sono stati notati quando l'outcome era il numero di morti da BPCO. Questo fenomeno è stato spiegato con il rilievo di iperreattività delle vie aeree, più frequente e grave nelle fumatrici [45]. Inoltre, fattori genetici come mancanza di α1-antitripsina, possono facilitare lo sviluppo di BPCO. Il fumo aumenta significativamente il rischio della malattia in soggetti caratterizzati da questo pattern genetico mendeliano [46]. La cessazione dell'abitudine al fumo è il mezzo più sicuro per prevenire o diminuire l'avanzamento della BPCO [47,48]. Sembra probabile che i programmi per la cessazione del fumo determinino una riduzione significativa della mortalità dei pazienti con BPCO [49]. Fumo e sintomi respiratori Dati raccolti da campioni di popolazione generale hanno confermato che i sintomi respiratori compaiono più frequentemente nei fumatori che nei non fumatori, sia nei maschi sia nelle femmine [41,50]. È stato dimostrato che una storia familiare positiva per BPCO è un fattore di rischio aggiuntivo per la presenza di sintomi di bronchite [51]. La cessazione del fumo attivo riduce significativamente la presenza di sintomi respiratori [52]. Fumo e funzione respiratoria Studi longitudinali e trasversali hanno dimostrato che il fumo attivo nuoce alla funzione respiratoria [53]. Fumare riduce il tasso di accrescimento del FEV1 durante l'adolescenza, riducendo così il valore massimo ottenibile di FEV1 [54]. Fumare anti- MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 21 Fumo ed altre malattie respiratorie Ci sono relativamente pochi dati riguardanti la relazione esistente tra il fumo attivo e le patologie respiratorie, a parte la BPCO ed il tumore del polmone. Comunque secondo evidenze scientifiche emergenti il fumo attivo può giocare un ruolo importante nel favorirne l'inizio o nell'aggravarne il corso naturale. Il fumo attivo è stato associato all'aumento dell'iperreattività bronchiale e del livello totale di immunoglobuline (IgE) [64]. È ben noto che i soggetti asmatici hanno un declino del FEV1 maggiore dei non asmatici; questo declino sembra essere maggiore in quelli che fumano [65,66]. Benché il ruolo del fumo attivo come fattore di rischio per l'asma resti da essere spiegato, i sintomi sono più gravi e le riacutizzazioni più frequenti e gravi tra gli asmatici fumatori rispetto agli asmatici non fumatori [64,67]. Il fumo attivo può alterare la risposta ai corticosteroidi riducendo così gli effetti benefici terapeutici di questi farmaci [67]. Il fumo attivo aumenta anche i rischi di ospedalizzazioni connesse con l'asma e di decesso per asma [65,68]. Negli asmatici la cessazione dell'abitudine al fumo, confrontata con l'abitudine al fumo invariata, ha migliorato la reattività dell'istamina delle vie aeree ed i sintomi respiratori dopo 4 mesi [69]. Molti studi hanno dimostrato che il fumo di sigaretta è per gli adulti un importante fattore di rischio per le polmoniti acquisite in comunità (CAP) [70]. Dati spagnoli hanno stimato il rischio attribuibile di popolazione (PAR) del fumo di tabacco per lo sviluppo di CAP al 32,4% (intervallo di confidenza al 95% (95% CI): 14,8-50,1). È stato trovato un rischio aumentato di CAP per l'incremento nella durata dell'abitudine al fumo, per un numero di sigarette fumate al giorno superiore alla media e per un maggiore consumo cumulativo di sigarette [71]. In aggiunta, la mortalità da CAP è correlata al numero di sigarette consumate in maniera dose-risposta [68]. Il fumo di sigaretta corrente è il fattore di rischio più importante per la malattia invasiva da pneumococco tra gli adulti sani, con un PAR del 51%. È stata individuata una relazione dose-risposta tra questa malattia ed il numero di sigarette fumate al giorno e pacchettianno [72,73]. È stato provato che il fumo attivo favorisce i sintomi iniziali della TB polmonare principalmente nei Paesi in via di sviluppo [73,74], ed aumenta anche il rischio di morte da TB [68]. Uno studio caso-controllo multicentrico ha dimostrato che i fumatori attuali (odds ratio (OR): 1,9; 95% CI: 1,3-2.9) ed ex (2,3; 1,3-3,8) presentano un rischio maggiore di sviluppare fibrosi polmonare idiopatica [75]. Gli studi epidemiologici non hanno ancora chiarito l'influenza dell'abitudine al fumo sulla storia naturale della malattia. Comunque un'anamnesi positiva per abitudine al fumo insieme con stadio patologico avanzato, sesso maschile ed età avanzata, è stata riscontrata essere un importante fattore di rischio per la mortalità a lungo termine da patologia interstiziale del polmone [76]. Con riferimento alla comparsa del pneumotorace, la letteratura scientifica ha dimostrato che il rischio di sviluppare questa malattia negli uomini fumatori sani è del 12%. Nei maschi non fumatori il rischio è 0,1%. Questa tendenza è presente nelle donne fumatrici “sane” ma in misura inferiore [77]. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement cipa l'inizio di declino del FEV1 nei giovani adulti accorciando così la fase plateau durante la quale la funzione respiratoria rimane quasi costante [55]. Inoltre, fumare accelera il declino del FEV1 nella tarda età adulta e nella vecchiaia [3,53,56]. Questo declino sembra essere più rapido nelle donne piuttosto che negli uomini una volta che la BPCO si è insediata [57]. Nello studio sulla salute del polmone (Lung Health Study) la media annuale di perdita del FEV1 era di circa 60 mL/anno tra coloro che continuavano a fumare al momento del follow up di 11 anni [58]. Molti studi hanno riportato una relazione dose-risposta tra il fumo e declino accelerato del FEV1 [3]. Studi longitudinali hanno dimostrato che smettere di fumare riduce il tasso del declino del FEV1 ad un valore vicino a quello dei non fumatori [3,59]. Il FEV1 può aumentare di poco dopo la cessazione dell'abitudine al fumo, ma non raggiungerà mai il livello atteso per un non fumatore [55]. C'è un'evidenza contrastante per coloro che sono fumatori intermittenti cioè che smettono di fumare e poi ricominciano (cosiddetti “ restarters”). Si è constatato che i restarters hanno un declino più rapido nel FEV1 rispetto a coloro che continuano ed agli ex fumatori [60]. Comunque i dati dal Lung Health Study dimostrano che coloro che avevano fatto diversi tentativi per smettere di fumare avevano una ridotta perdita di funzione respiratoria, ad analoghe dosi cumulative di sigarette, rispetto a quelli che continuavano a fumare [61]. La riduzione del fumo, cioè dimezzando il consumo delle sigarette giornaliere per un periodo di 2 anni, e facendo nel frattempo uso di un inalatore di nicotina, non ha avuto alcun effetto sul FEV1 [62]. Il fumo attivo influisce anche su altri indici di funzione respiratoria, oltre al FEV1. È stata osservata un'associazione tra la diminuzione della capacità di diffusione del polmone per il monossido di carbonio (DL,CO) ed il consumo cumulativo di sigarette, anche in soggetti sani [63] e il DL,CO può migliorare nei soggetti che smettono di fumare [64]. Il fumo attivo provoca un grado maggiore di iperreattività delle vie aeree. In soggetti senza sintomi respiratori cronici o BPCO la cessazione del fumo riduce la reattività delle vie aeree che viene valutata con un test di stimolazione alla metacolina. Nei pazienti con BPCO la cessazione del fumo riduce la reattività delle vie aeree alla metacolina ma non la riporta ai livelli normali [48]. VALUTAZIONE La valutazione del fumatore è importante per definire quale tipo di trattamento sia necessario. A tal MRM 21 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 22 fine è importante capire la motivazione che spinge il paziente a smettere di fumare, il suo grado di dipendenza da nicotina e qualsiasi altra condizione di comorbosità che possa interagire con la cessazione del fumo. La misura immediata del CO nell'aria espirata è un'altra determinazione che può aiutare molto per aumentare la motivazione e per testare i miglioramenti durante il percorso. Abitudine al fumo Di solito è sufficiente una domanda diretta. Se il paziente dichiara di essere un non fumatore, ma il sanitario è incerto, il CO espirato, la cotinina salivare, urinaria o plasmatica e l'esame delle dita e del respiro del paziente possono fornire informazioni oggettivamente valutabili. L'abitudine al fumo dovrebbe essere annotata con evidenza nella cartella del paziente, incluso il tipo di tabacco usato (sigarette, sigari o pipa) e la quantità fumata comprensiva di pacchetti-anno. Motivazione a smettere La determinazione o la forte motivazione a smettere sembrano essere cruciali per il successo nella cessazione del fumo. Non ci sono misure efficaci e validate per valutare il grado di motivazione. Comunque un semplice strumento per stabilire la volontà del paziente a smettere può essere chiedergli di dare una stima graduata, su una scala a 10 punti, in base alla domanda “Quanto importante è per lei smettere di fumare?”. Il medico può aiutare il paziente mostrandogli un modello di scala con il punteggio di 10 che rappresenta “estremamente importante” e di 0 che rappresenta “nessuna importanza”. Nella realtà clinica è utile anche avere un'idea della percezione di auto-efficacia. Può essere informativo chiedere: “Se dovesse decidere di smettere di fumare, quanto è sicuro che riuscirebbe a farlo?”, valendo 10 punti la risposta “Sicuramente certo che potrei riuscire” e 0 “Sicuramente certo che fallirei” [78]. Se il paziente è pronto a smettere dovrebbe riportare punteggi elevati in entrambe le variabili. Se la motivazione è alta, ma l'autostima è bassa, il trattamento ed il supporto sono critici per il successo. Se l'autostima è alta, ma la volontà a provare è bassa, è cruciale un intervento di tipo educazionale. Se entrambi i punteggi sono alti, può essere fissata immediatamente una data di cessazione. Se entrambi i punteggi sono bassi, allora la motivazione e l'autostima devono essere stimolate. La maggior parte dei medici pneumologi ha troppo poco tempo da dedicare ai propri pazienti, spesso solo pochi minuti per ognuno di loro. Al fine di massimizzare il limitato tempo disponibile, il medico sente la necessità di usare questo tempo per comunicare informazioni importanti per il paziente, spesso in modo autoritario, ed unidirezionale. Questo stile è generalmente anche il modo più efficace per trasferire informazioni quando il tempo è limitato. Ma qual è il sistema migliore se l'obiettivo è di cambiare attitudini? In questo caso (aumentare la determinazione e la motivazione a cambiare l'a- 22 MRM bitudine al fumo), questa strategia potrebbe non essere ideale. L'atteggiamento verso il fumo può essere più difficile da cambiare che, per esempio, l'imparare ad evitare allergeni. Così è necessaria una strategia diversa, in particolare perché i pazienti respiratori non si rivolgono di solito al medico per chiedere, in prima istanza, un aiuto per smettere di fumare. Sfortunatamente, una situazione frequente è che al paziente sia già stato consigliato di smettere molte volte da parte del medico stesso, o da altri colleghi, e che abbia ripetutamente fallito nei suoi tentativi. Questi ripetuti fallimenti possono aver indebolito l'auto-stima e la fiducia in se stesso tanto che, per ottenere un favorevole bilanciamento tra attitudine e comportamento, essi arrivino a dire che non hanno più intenzione di smettere. Questo può essere visto come un adeguamento alla realtà: “Perché provare ancora se fallisco sempre?”. Al fine di aiutare questi fumatori, il medico deve stabilire una buona relazione con essi. Normalmente, il paziente si aspetta che gli venga detto di smettere in modo diretto e chiaro, ma questa modalità può imbarazzarlo, e talvolta tacitamente, se non apertamente, renderlo aggressivo e sulle difensive. Pertanto, si richiede un approccio secondo il quale il fumo possa essere discusso in modo non minaccioso, rispettoso ed empatico. Dipendenza La larga maggioranza di fumatori fuma per gli effetti della nicotina e la maggior parte sono dipendenti dalla nicotina rilasciata dalle sigarette. Il livello di dipendenza è molto variabile. In passato, il numero di sigarette fumate al giorno è servito come unica misura di dipendenza. Tuttavia, la ricerca scientifica ha dimostrato che il numero di sigarette da solo non è una misura ottimale della dipendenza da nicotina [79]. Misure biochimiche come i livelli di nicotina e del suo principale metabolita, la cotonina, sono stati più recentemente usati come indicatori di dipendenza. Tuttavia, poiché la nicotina ha una breve emivita, di circa 2 ore, le sue concentrazioni sono dipendenti dal momento del giorno e da quando è stata fumata l'ultima sigaretta. È più spesso consigliato l'uso della cotinina, che possiede una emivita di 15-20 ore. Entrambe possono essere misurate nel plasma, nella saliva e nelle urine. Una concentrazione di cotinina plasmatica < 15 γ•mL -1 è considerata il livello del non fumatore, ma la maggioranza dei fumatori non esposti al fumo passivo ha concentrazioni da non determinabile a 10 γ•mL -1. Il livello medio dei fumatori è intorno a 200 γ•mL 1 , ma può raggiungere 1.000 γ•mL -1 [80]. Numerosi laboratori possono misurare la cotinina plasmatica la cui determinazione potrebbe facilmente essere approntata in molti ospedali. Un'indicazione del grado di dipendenza può essere ottenuta anche usando questionari. Il Test di Fagerström per la Dipendenza da Nicotina (Fagerström Test for Nicotine Dependance - FTND) è un breve questionario (6 domande) largamente MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 23 Precedenti esperienze di cessazione del fumo Può essere molto utile indagare sui precedenti tentativi di cessazione; per esempio, indagando sul più lungo periodo senza fumo, sulle difficoltà incontrate e sui sintomi di astinenza, sui metodi utilizzati come aiuto, quale è stato l'evento che ha stimolato la ricaduta e se e quali benefici si sono sperimentati durante l'astinenza. Tutto ciò può dare un'idea delle difficoltà che intercorreranno e fornire l'opportunità per gestirle meglio. Monossido di carbonio Il fumo di sigaretta comporta l'assorbimento di molte sostanze tossiche. Il CO è una di queste e può essere facilmente monitorato. La determinazione del CO può essere vista come un indicatore del consumo di fumo complessivo. La concentrazione di CO può essere facilmente ottenuta chiedendo al fumatore di espirare dentro un analizzatore di CO. L'unità di misura è il CO in ppm, che può essere facilmente convertito nel livello di carbossiemoglobina (COHb) corrispondente. In assenza di un analizzatore di CO espirato, la COHb può essere misurata dall'analisi di un campione di sangue. Dimostrare “l'effetto CO” nei fumatori è di grande valore motivazionale. La procedura raccomandata è che l'operatore per primo espiri nello strumento, mostrando la concentrazione normale di 1-3 ppm. Successivamente il fumatore soffierà a sua volta nello strumento nel quale immediatamente e inevitabilmente leggerà valori molto più alti di 10-20 ppm (2-5% di COHb). In condizioni ambientali normali, il valore di un non fumatore non dovrebbe eccedere 4 ppm. L'emivita del CO è di circa 4 ore, ma esso è in parte esercizio-dipendente. Le letture effettuate al mattino sono quindi più basse di quelle pomeridiane [86]. Entro 1-2 giorni dall'ultima sigaretta, il livello di CO ritorna nella norma. Vedere questa rapida normalizzazione è molto incoraggiante per il soggetto. Dopo la normalizzazione il livello di CO può essere usato per monitorare il progresso durante il follow up. Un valore anomalo di CO può essere usato per informare il fumatore sui meccanismi con L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement usato e validato [81]. FTND può essere compilato tramite intervistatore così come può essere autosomministrato (Tabella II). Il punteggio ottenuto è compreso tra 0 e 10 e il suo valore medio in campioni rappresentativi di fumatori è abitualmente di 3-4 punti. Le due domande più importanti sono l'ora della prima sigaretta del mattino e il numero di sigarette fumate al giorno. Queste due domande forniscono quasi tutte le informazioni derivabili dall'intero questionario. Se il tempo a disposizione è molte limitato, l'ora della prima sigaretta può essere usata come proxi [79]. Un altro forte indicatore di dipendenza, anche se relativamente infrequente, è il fumo notturno. Questi fumatori hanno, in genere, punteggi molto alti di FTND. Più alto è il punteggio, più forte è la dipendenza ed è più difficile smettere. Il punteggio di FTND predice anche la gravità dei sintomi di astinenza e la necessità di un trattamento farmacologico [82,83] ed è correlato alla determinazione genetica di specifici recettori nicotinici [84]. Nella Tabella II i fumatori sono caratterizzati approssimativamente in rapporto alla gravità della dipendenza. Nella ICD-10 [19], sette criteri (il desiderio impellente di fumare, la difficoltà a controllare la quantità di fumo, l'uso continuativo nonostante le dannose conseguenze per la salute, la priorità rispetto alle altre attività, l'aumentata tolleranza, l'astinenza fisica) sono utilizzati per diagnosticare la dipendenza da tabacco. Sono necessari tre dei sette criteri per porre la diagnosi. Con questo sistema, la dipendenza da tabacco può essere definita solo qualitativamente. Alcuni studi sono stati condotti nel tentativo di utilizzare la presenza dei sintomi di astinenza secondo una scala quantitativa [85], ma non esistono criteri standardizzati a questo scopo. TABELLA II: IL TEST DI FAGERSTRÖM PER VALUTARE LA DIPENDENZA ALLA NICOTINA (FTND) Domanda Risposta Punteggio entro 5 minuti tra 6 e 30 minuti tra 31 e 60 minuti dopo 60 minuti 3 2 1 0 sì no 1 0 la prima del mattino qualsiasi altra 1 0 10 o meno tra 11 e 20 tra 21 e 30 31 o più 0 1 2 3 5) Fuma più frequentemente durante le prime ore del mattino dopo il risveglio che durante il resto della giornata? sì no 1 0 6) Fuma anche quando è così malato da dover trascorrere a letto la maggior parte della giornata? sì no 1 0 1) Quanto tempo dopo essersi svegliato/a fuma la prima sigaretta? 2) Trova difficile astenersi dal fumo dove è proibito fumare? 3) Quale sigaretta Le dispiacerebbe maggiormente non fumare? 4) Quante sigarette fuma al giorno? MRM 23 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 24 cui il fumo, ed in particolare il CO, contribuiscono allo sviluppo delle malattie cardiovascolari. Se l'obiettivo è la riduzione del fumo, piuttosto che la cessazione, il monitoraggio del CO è essenziale. Il numero di sigarette fumate può essere ridotto, ma spesso il fumatore compensa la potenziale riduzione nell'assunzione di nicotina inalando più profondamente dalle sigarette residue, riducendo il possibile beneficio derivato dal fumare un numero minore di sigarette. La misura del CO, preferibilmente effettuata nel pomeriggio, è anch'essa un indicatore di dipendenza. Poiché c'è una relativamente piccola variazione nella emissione di CO dalle differenti marche di sigarette (diversamente da quanto è stampato sui pacchetti) le differenze ottenute possono essere in gran parte attribuibili alla diversa “ricerca” di nicotina ed alla dipendenza. I pazienti BPCO hanno valori più elevati di CO espirato. Non è chiaro se questo sia il risultato di differenze nell'emivita del CO, della produzione di CO conseguente all'infiammazione, di altri fattori intrinseci o semplicemente dell'intensità del fumo, ma l'intensità del fumo e i differenti pattern respiratori appaiono essere le più probabili spiegazioni dei più alti valori di CO nei pazienti con BPCO [87]. Spirometria e cessazione del fumo Le prove di funzionalità respiratoria sono fortemente raccomandate nel corso della valutazione basale dei fumatori provenienti dalla popolazione generale. L'obiettivo è di individuare malattie respiratorie nei fumatori suscettibili [88-91] e di aumentare il tasso di cessazione, come conseguenza di un rinforzo della motivazione a smettere causata dalla dimostrazione oggettiva di un danno polmonare [92]. I pazienti respiratori probabilmente minimizzano la loro percezione del rischio di malattia e le prove di funzionalità respiratoria possono essere per il sanitario un mezzo per dimostrare oggettivamente gli effetti del fumo, a livello individuale. È stata fatta una revisione dell'evidenza che la misurazione di un rischio biologico possa avere un effetto sul fumo futuro [93]. Poiché sono stati usati solo otto studi, che hanno fornito dati insufficienti, non è stato possibile trarre alcuna conclusione certa. Usare la misurazione del CO, testare la funzione polmonare, il rischio genetico di cancro al polmone o la ultrasonografia delle arterie carotidi e femorali, sia separatamente che in combinazione, non sembrerebbe avere effetto sul tasso di astinenza. Tuttavia, la spirometria è consigliata durante la valutazione basale dei fumatori provenienti dalla popolazione generale, al fine di identificare la presenza di malattie polmonari in fumatori suscettibili. Comorbosità Fumare può essere visto come un modo per affrontare lo stress giornaliero e situazioni di disagio. È stato osservato che nei forti fumatori esiste un'aggregazione di problemi clinici e subclinici come schizofrenia, deficit di attenzione, disordini da ipe- 24 MRM rattività, dipendenza ed abuso di altre droghe. Comunque, il più studiato e rilevante disordine psichiatrico associato al fumo è la depressione [94]. Una storia di depressione e fumo spesso vanno insieme e possono condividere meccanismi genetici [95] e se un fumatore presenta anche una storia di depressione sarà per lui più difficile smettere di fumare [96]. Depressione e ansia sono molto comuni in pazienti con malattie respiratorie, particolarmente quelli affetti da BPCO [97]. Al fine di capire meglio e trattare pazienti depressi si raccomanda al medico di porre queste due domande: 1) durante gli ultimi mesi si è sentito preoccupato, depresso, o senza speranza?; 2) durante gli ultimi mesi è stato spesso preoccupato di avere scarso interesse o scarso piacere nel fare le cose? Rispondere “sì” ad entrambe le domande è segno di forte depressione [98]. Per valutare la depressione può essere usata anche una sola domanda (“si è spesso sentito giù durante le ultime due settimane?”), che si è dimostrata essere valida (99]. Circa il 25% delle ricadute nell'abitudine al fumo è causato dalla depressione [84]. Questi pazienti che hanno una precedente storia di depressione, o hanno avuto depressione in altri tentativi di smettere di fumare, hanno più probabilità di soffrirne nuovamente ad un nuovo tentativo. È più comune soffrire di malumore che di reale depressione. Queste situazioni si presentano generalmente tra la quarta e la settima settimana di astinenza, ma consigli e incoraggiamento sono di solito sufficienti a risolverle. Talvolta sono però necessari l'uso di un adeguato trattamento e l'intervento di uno specialista [79,84]. CARATTERISTICHE DEI PAZIENTI RESPIRATORI CHE FUMANO Le persone fumano per molti differenti motivi. Alcuni fumano per conformarsi ad un comportamento predominante mentre altri sono i soli a fumare nel loro ambiente sociale. Alcuni possono fumare per lo stesso motivo per cui si beve alcool, per trarne un effetto positivo, mentre altri sono intrappolati nel loro comportamento e presentano sintomi d'astinenza se cercano di smettere. In questa sezione saranno considerati i pazienti con problemi respiratori, in modo particolare quelli affetti da BPCO, che può influenzare il loro comportamento. Perché i pazienti respiratori sono un target difficile La più comune e forte motivazione per smettere di fumare è la salute. Quando i fumatori invecchiano, la motivazione per smettere cresce o almeno si manifesta in diversi tentativi [100]. I fumatori con malattie respiratorie sembrano più motivati a smettere di fumare rispetto agli altri [8], in modo particolare se credono che il fumo sia la causa dei loro sintomi respiratori [101]. Alcuni fumatori hanno successo nello smettere di fumare e questi escono dalla popolazione dei fumatori, ma la maggior parte fallisce. Quando i sintomi peggiorano, questi MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 25 Auto-medicazione per le comorbosità Un altro fattore che può contribuire alle difficoltà nell'affrontare pazienti respiratori che fumano è la relativamente alta prevalenza di depressione o cattivo umore [102,103]. La depressione è indipendentemente associata al fumare e al fallimento nello smettere [104,105]. La depressione è anche uno dei pochi sintomi di astinenza che predicono la ricaduta al fumo [106,107]. Ci sono alcune prove che dimostrano che il livello di ansia, che spesso è parte della depressione, è più alto in fumatori affetti da BPCO [108]. È stato anche suggerito che questi pazienti soffrono di alessitimia o mancanza di emozioni [109]. Essi sono caratterizzati, sorprendentemente, come viventi in una camicia di forza emozionale ed è stato proposto che i pazienti con BPCO più grave non possono più essere arrabbiati, depressi o scontenti, perché ogni cambiamento importante di umore può indurre a sintomi di stress e qualche volta ad uno scompenso fisiologico [110]. In questa situazione fumare può aiutare come una sorta di auto-medicazione che controlla l'ansia e le emozioni: ricadere dopo un tentativo di smettere di fumare può essere un modo per sfuggire ad uno stato di depressione e ansia. In un interessante studio, Wagena e coll. [97] hanno studiato l'associazione tra depressione e BPCO/asma. È stato condotto uno studio prospettico su lavoratori nel quale la BPCO/asma e la depressione sono stati autovalutati da un questionario. È stato trovato che il 10% dei lavoratori non fumatori con BPCO/asma sono depressi, mentre il 29% dei fumatori si autodefinisce depresso. Nel gruppo BPCO/asma la presenza di depressione è il doppio rispetto al gruppo di controllo di fumatori con altri disturbi cronici (malattie di cuore e reumatiche) ed il quadruplo rispetto ai fumatori sani. Dipendenza Ci sono sufficienti evidenze che il grado di dipendenza misurato dal FTND [81] predica il risultato dei tentativi di smettere di fumare, particolarmente in assenza di trattamento farmacologico [82]. Con un appropriato trattamento farmacologico, il peso eccessivo dell'alta dipendenza può essere parzialmente alleviato. L'evidenza che i pazienti respiratori fumatori, e particolarmente quelli affetti da BPCO, abbiano più alta dipendenza al tabacco è relativamente forte e consistente. I fumatori con BPCO hanno un alto punteggio nell'FTND rispetto alla media dei fumatori [111,112]. Lo stesso è stato trovato nei pazienti con cancro al polmone [113,114]. In Spagna è stato studiato un campione rappresentativo della popolazione che ha mostrato che i fumatori con BPCO erano più dipendenti alla nicotina rispetto ai fumatori sani (punteggi FTND 4,7 vs 3,2, rispettivamente; p < 0,001). Lo stesso studio ha trovato che solo il 10% dei fumatori sani aveva alta dipendenza, mentre il 28% dei fumatori con BPCO era altamente dipendente. Inoltre, quasi il 60% dei fumatori sani aveva bassa dipendenza, rispetto a solo un terzo dei fumatori con BPCO [87]. Ogni punto addizionale nel FTND è stato significativamente associato ad un aumento dell'11% in più di sviluppare BPCO [115). È abbastanza plausibile che coloro che hanno un'alta dipendenza, come indicato da un più elevato consumo di sigarette e/o da più elevate concentrazione di cotinina e di CO, abbiano una maggiore probabilità di ammalarsi a causa del fumo. Nello studio spagnolo [87] i fumatori con BPCO avevano una più alta concentrazione di CO nell'aria respirata rispetto ai fumatori sani (19,7 vs 15,4, rispettivamente; p < 0,0001). Questa alta dipendenza contribuisce all'aumento del rischio di malattie respiratorie e rende anche più difficile smettere selezionando ulteriormente un “nocciolo duro” di fumatori altamente dipendenti. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement provano a smettere di nuovo. Coloro che falliscono sono quelli che avranno più difficoltà a smettere, per varie ragioni di cui parleremo dopo. È probabile che, in alcuni momenti, durante lo sviluppo dei sintomi respiratori, sia stato dato un consiglio a smettere da parte del Medico di Medicina Generale (MMG), forse ripetutamente, e che quindi il processo di selezione continui con molti più fumatori recalcitranti che rimangono nella popolazione. È anche possibile che alcuni pazienti respiratori ad un certo punto si dimostrino insofferenti al consiglio di smettere, soprattutto se le stesse procedure e trattamenti sono suggeriti ripetutamente. Da questa ipotesi di selezione deriva che più grave è la malattia polmonare, più difficile è smettere di fumare. Per esempio, in uno stadio avanzato della BPCO la qualità della vita è bassa ed i pazienti fumatori considerano le sigarette una delle poche cose che possano migliorare la qualità della vita. Pattern di inalazione del fumo I fumatori con BPCO tendono ad inalare più profondamente e rapidamente rispetto ai fumatori sani [111,116]. Mentre i fumatori in genere tendono a inalare fumo in 2 “stadi”, prima aspirando il fumo in bocca e nelle vie respiratorie superiori quindi inalandolo nei polmoni, i fumatori con BPCO sembrano inalare il fumo direttamente nei polmoni. Questo metodo espone i polmoni al fumo con più alta temperatura. È anche possibile che un aumento nella deposizione delle particelle possa derivare da alterazioni fisiologiche caratteristiche della BPCO [117]. Il rimodellamento delle piccole vie aeree che conduce all'ostruzione e ad un incremento nelle resistenze delle vie aeree è la principale componente della limitazione al flusso aereo. Questo significa che lo svuotamento è incompleto durante la respirazione a volume corrente ed il volume polmonare non ritorna al suo naturale punto di equilibrio, conseguentemente si verifica l'intrappolamento d'aria. Si può ipotizzare che con l'aumento della severità dell'ostruzione al flusso aereo, la deposizione delle particelle del fumo può aumentare ulteriormente e accelerare il declino della limitazione al flusso espiratorio. Controllo del peso Controllare il peso corporeo è un importante eleMRM 25 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 26 mento per i pazienti respiratori [118,119]. Un basso indice di massa corporea (BMI) è un problema per molti pazienti all'ultimo stadio di BPCO ed è associato con una peggiore prognosi. Per questo gruppo di pazienti, l'incremento di peso di 4-5 kg, tipicamente osservato durante il primo anno dopo aver smesso di fumare, potrebbe essere un vantaggio. Teoricamente, questo può anche essere un beneficio nei pazienti con cancro al polmone che hanno perdita di appetito. Sebbene molte donne abbiano paura di prendere peso dopo aver smesso, la prevenzione dell'incremento di peso post-cessazione non aumenta il tasso di successo. Per pazienti con BPCO con alto BMI, il vantaggio dello smettere di fumare per il mantenimento della funzione polmonare è più importante degli effetti avversi dati dall'assunzione di peso. Poiché approssimativamente un terzo dell'aumento di peso post-cessazione è dovuto ad una riduzione del metabolismo basale e due terzi ad un aumento dell'importo calorico [120], le restrizioni alimentari possono essere applicate 2-3 mesi dopo la data di stop del fumo, evitando quindi ulteriori difficoltà durante la prima fase del processo di cessazione. Il consiglio di aumentare l'esercizio fisico è anche importante per prevenire l'aumento di peso dopo aver smesso. INTERVENTI PSICOLOGICI E COMPORTAMENTALI Questa parte si concentra sugli interventi psicologici e comportamentali e sulla loro relativa efficacia per la cessazione del fumo. Si conclude discutendo l'applicazione di questi interventi per i fumatori con BPCO. Tre interventi possono essere considerati come strategie psicologiche e comportamentali per facilitare la cessazione del fumo di tabacco: interventi di auto-aiuto, breve consiglio e counselling. I tassi di astinenza o di successo sono riportati come: 1) tassi di cessazione totale (prolungata), es. non fumare (nemmeno una sola sigaretta) di solito dalla data di cessazione (con un periodo di tolleranza di 1 o 2 settimane) fino al termine di 6 mesi o un anno; e 2) i tassi di prevalenza puntuale di cessazione es. soggetti che non hanno fumato durante le ultime 24 ore o una settimana come stabilito. I tassi di prevalenza puntuale sono di solito un po' più alti di quelli dell'astinenza continuativa, ma questi ultimi riflettono più accuratamente il tasso di astinenza a lungo termine. Programmi di auto-aiuto L'auto-aiuto si definisce quel programma strutturato per i fumatori che cercano di interrompere completamente l'abitudine al fumo senza una terapia intensiva. Una revisione della letteratura sull'efficacia del materiale relativo all'auto-aiuto per la cessazione del fumo rivela l'efficacia dei materiali individualizzati [121-124]. Secondo questi dati, i materiali personalizzati per l'auto-aiuto possono essere consigliati per la cessazione del fumo (livello di evidenza A). 26 MRM Consiglio breve Il consiglio breve dato da medici o infermieri può essere definito come un mezzo di routine per procurare ai fumatori alcune informazioni che possano aiutarli a smettere di fumare ed aumentare le motivazioni per tentare la cessazione. Le revisioni di efficacia del consiglio breve dato da medici o infermieri [125,126] suggeriscono che questo se è dato dal medico ha un effetto significativo, benché piccolo. È stato dimostrato un piccolo ma significativo incremento nella probabilità di cessazione (OR: 1,69; 95% CI: 1,45-1,98) [125]. Questo equivale ad una differenza assoluta nel tasso di cessazione di circa 2,5% nei fumatori che hanno ricevuto il consiglio medico rispetto a coloro che non lo hanno ricevuto. Pertanto, se viene dato il consiglio breve a 50 pazienti, ci sarà un ex fumatore aggiuntivo dopo 6-12 mesi. Un confronto degli studi sulla cessazione del fumo effettuato dalla British Thoracic Society (BTS) ha dimostrato che il consiglio breve agisce efficacemente nei fumatori con BPCO [127]. L'aumento del numero delle sedute di consiglio breve non incrementa significativamente l'efficacia [128]. Il consiglio di smettere di fumare dato dagli infermieri migliora la cessazione del 1% paragonandola ai gruppi di controllo [126]. Secondo questi dati può essere raccomandato che siano i medici a dare ai fumatori il consiglio breve sulla cessazione del fumo, anche ai pazienti respiratori. Gli infermieri dovrebbero fare la stessa cosa (livello di evidenza A). Tuttavia, per la maggioranza dei pazienti polmonari non è sufficiente il consiglio breve ed è richiesto un intervento molto più intensivo. Comunque, sono principalmente i fumatori leggeri a rispondere al consiglio breve. Counselling Ci sono tre tipi di counselling (individuale, di gruppo e telefonico) che variano secondo il modo di procurare la terapia ed il tempo impiegato. Counselling individuale Il counselling individuale è definito un incontro faccia a faccia tra un paziente ed un consulente esperto nella cessazione dell'abitudine al fumo. Secondo la più recente revisione c'è sufficiente evidenza per supportare il counselling individuale nella cessazione dell'abitudine al fumo: sono necessari 25 pazienti da sottoporre a couselling individuale per ottenere un ex fumatore aggiuntivo [128]. C'è una forte relazione dose-risposta tra la lunghezza della sessione del contatto personale ed il successo del trattamento. Interventi intensivi sono più efficaci di interventi meno intensivi (livello di evidenza A). L'evidenza suggerisce anche una relazione dose-risposta tra il numero delle sessioni e l'efficacia del trattamento, cioè i trattamenti che durano più di 8 sessioni sono significativamente più efficaci degli interventi che durano fino a tre sessioni. In conclusione il counselling individuale è efficace nell'aiutare i pazienti ad interrompere l'abitudine al fumo (livello di evidenza A). MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 27 Counselling telefonico Il counselling telefonico può potenzialmente integrare gli interventi faccia a faccia o sostituire il contatto faccia a faccia come un'aggiunta agli interventi di auto-aiuto. Può anche essere scelto al momento giusto per portare al massimo il livello di aiuto in vicinanza della data di cessazione pianificata ed anche programmato in risposta alle necessità del ricevente. Il counselling telefonico può essere pro-attivo o reattivo [130]. Nell'approccio pro-attivo, il terapista inizia le telefonate dando al fumatore supporto per fare un tentativo di cessazione (OR: 1,41; 95% CI: 1,271,57). Il counselling reattivo avviene attraverso linee telefoniche dedicate che rispondono alle chiamate dei fumatori (1,33; 1,21-1,47) [131]. L'analisi dell'ultima revisione sistematica ed altri trial hanno evidenziato che il counselling telefonico pro-attivo aveva una maggiore efficacia rispetto ai materiali standard di auto-aiuto. Tuttavia il counselling telefonico in aggiunta alla farmacoterapia o in aggiunta all'intervento faccia a faccia senza farmacoterapia, non migliora il risultato di tali interventi nei fumatori sani. [131-133]. Le conclusioni suggeriscono che il counselling telefonico pro-attivo è efficace se confrontato con altri interventi minimali (livello di evidenza A). Terapia comportamentale Un trattamento completo dovrebbe rivolgersi anche a quella parte comportamentale e psicologica della dipendenza da tabacco. Qualche aspetto della terapia comportamentale, qualche volta riferito anche come counselling, è quindi importante in un approccio ottimale del trattamento. Terapia aversiva La terapia aversiva unisce qualche stimolo spiacevole allo stimolo di piacere che si ottiene fumando una sigaretta. Il procedimento più frequentemente esaminato è stato quello di fumare velocemente, il che ha come conseguenza la nausea. Benché l'ultima revisione sistematica di Cochrane abbia provato che fumare velocemente potrebbe essere efficace, l'unico studio che risponda ai criteri correnti per l'adeguatezza metodologica ha prodotto un trend non significativo [134]. I risultati suggeriscono che non c'è evidenza sufficiente per supportare l'uso del fumo aversivo per riuscire a smettere di fumare. Terapia dell'esercizio fisico Gli argomenti per l'utilizzo dello sforzo nella cessazione del fumo sono supportati dall'evidenza che dimostra che l'esercizio fisico ha un effetto moderante su molte delle variabili negativamente affette dalla sospensione dell'assunzione di nicotina. È evidente anche che l'esercizio fisico può avere un effetto positivo sui fattori che possono proteggere contro la ripresa dell'abitudine al fumo [135-138]. Comunque la più recente revisione sistematica suggerisce che non c'è sufficiente evidenza per supportare l'esercizio fisico per la cessazione del fumo [139]. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement Counselling di gruppo La terapia di gruppo offre agli individui l'opportunità di imparare le tecniche comportamentali per la cessazione dell'abitudine al fumo e provvedere a sostenersi reciprocamente. Questo tipo di sostegno permette a più persone di essere trattate da un terapista e può avere un migliore rapporto costo-efficacia rispetto al counselling individuale. Per aiutare le persone che vogliono interrompere l'abitudine al fumo, la terapia di gruppo è migliore del non avere alcun intervento di aiuto (OR: 2,17; 95% CI: 1,37-3,45) e meglio della terapia di autoaiuto (OR: 2,04; 95% CI: 1,60-2,60). C'è un evidenza insufficiente sul fatto che la terapia di gruppo sia più efficace, o abbia un miglior rapporto costo-efficacia rispetto al counselling individuale intensivo [129]. Comunque diversi studi placebo-controllati con terapia di gruppo e NRT mostrano tassi di cessazione relativamente alti (circa 30%) mantenuti per un anno utilizzando NRT combinato con la terapia di gruppo [129]. Non c'è evidenza sull'efficacia della terapia di gruppo nei pazienti con problemi respiratori. Si può trarre la seguente conclusione: il counselling di gruppo è efficace per la cessazione dell'abitudine al fumo (livello di evidenza A). Non è chiaro se il counselling di gruppo sia più o meno efficace del counselling individuale (livello di evidenza A). Procedure per interventi psicologici e comportamentali nella cessazione del fumo Una parte cruciale del programma per aiutare i fumatori a smettere è quello di stabilire visite programmate dopo la data della cessazione. Ci sono diversi tipi di piani. I medici devono riconoscere che l'aumento del numero delle visite fino a 8 può aumentare la percentuale di successo. Il seguente programma di visite può essere raccomandato: settimane 1, 2, 4, 8 e 12, e 6 e 12 mesi dopo la data di cessazione. Dovrebbero essere tenute di conto alcune considerazioni allo scopo di procurare al fumatore il migliore aiuto durante il periodo di follow up. A volte, gli ex-fumatori sentono la necessità di fumare di nuovo anche oltre i primi giorni dopo la cessazione. Questa sensazione turba molto il fumatore e può condurre alla ripresa dell'abitudine al fumo. I fumatori dovrebbero essere informati che tali sensazioni sono comuni e dovrebbero essere incoraggiati a riflettere sulla loro motivazione a smettere di fumare. Mettere in pratica attività gratificanti durante questa fase può essere molto utile per alleviare questa sensazione [9]. Qualche volta i fumatori in astinenza possono soffrire di sintomi di astinenza per lunghi periodi. I terapisti dovrebbero capire che è cruciale spiegare ai pazienti l'evoluzione dei diversi sintomi. I fumatori devono capire i sintomi, la durata, l'intensità e l'evoluzione, poiché questa conoscenza li aiuta a mantenere l'astinenza. Inoltre, i medici dovrebbero considerare di estendere l'uso di farmacoterapia oltre il periodo di trattamento raccomandato o usare una combinazione di diversi tipi di trattamento farmacologico. Alternativamente, dovrebbero MRM 27 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 28 essere prese in considerazione dosi più elevate di NRT per alleviare la sindrome da astinenza. Non c'è prova che queste procedure aumentino i rischi per la salute [140,141]. In situazioni speciali (occasioni sociali, mangiare e bere, incontrare amici, ecc.), i fumatori si possono sentire talmente sicuri di sé da provare a fumare solo una sigaretta. Spesso questa “sigaretta innocente” può immediatamente portare a riprendere di nuovo l'abitudine al fumo. I medici devono spiegare chiaramente al paziente che iniziare a fumare, anche una sola tirata, aumenterà il bisogno di fumare, renderà la cessazione più difficile e metterà il paziente ad alto rischio di ricaduta [9]. I fumatori dovrebbero sapere che anche una debolezza isolata conduce di solito ad una ricaduta. Deve essere considerato un insuccesso del programma di cessazione se il fumatore continua a fumare giornalmente per 2-3 settimane dopo aver ricevuto un trattamento adeguato per la dipendenza. L'approccio al trattamento di questi pazienti potrebbe essere il seguente: 1) il medico dovrebbe congratularsi con il fumatore per aver fatto un serio tentativo di cessazione dell'abitudine al fumo. Dovrebbe spiegare al fumatore che, nonostante abbia fallito, egli/ella ha imparato le astuzie che possono essere usate in altri tentativi. Maggiori i tentativi fatti, più alta la possibilità di successo. I medici devono incoraggiare i fumatori che hanno fallito a prendere un altro appuntamento entro 2/3 mesi allo scopo di fare un ulteriore serio tentativo; 2) in alcuni casi può essere considerata la possibilità di iniziare un approccio di riduzione del danno. Interventi psicologici e comportamentali in pazienti con malattie respiratorie che fumano Tre studi hanno valutato l'efficacia dell'intervento comportamentale per la cessazione dell'abitudine al fumo in pazienti con BPCO [142-144]. Il primo, un piccolo studio pilota, ha valutato se l'uso delle parole “i polmoni del fumatore” invece della terminologia tradizionale parlando con i fumatori con BPCO, avesse avuto influenza sul loro modo di fumare [142]. Malgrado l'uso del termine “polmoni del fumatore” abbia aumentato l'astinenza, l'effetto non è stato significativo. In effetti, gli autori di questo documento non sono d'accordo sull'uso del termine “polmoni del fumatore” perché è utilizzato spesso per biasimare il fumatore con BPCO e addossare la colpa al paziente. Un altro studio ha paragonato l'efficacia di diversi programmi di rinforzo comportamentale [142]. L'incentivo rappresentato da biglietti della lotteria dati dopo la dimostrazione di una riduzione del CO espirato non produceva differenza nei tassi di astinenza prolungata rispetto allo stesso incentivo dato in seguito alla semplice dichiarazione di aver ridotto il fumo. Inoltre, l'incentivo rappresentato da biglietti della lotteria dati dopo la dimostrazione di una riduzione del CO espirato non produceva differenza nei tassi di astinenza prolungata rispetto al rimborsare i pazienti che si presentavano alle visite programmate. Il terzo studio ha dimostrato che il counselling individuale adattato ai bisogni ed alle 28 MRM domande del paziente, insieme all'uso di un manuale di auto-aiuto per la cessazione del fumo, non era significativamente più efficace rispetto al consiglio del medico di smettere di fumare [143]. Tre precedenti ampi studi su pazienti ambulatoriali che testavano l'effetto di diversi interventi sulla cessazione dell'abitudine al fumo su pneumopatici, senza riferire dati sulla funzione respiratoria, sono stati pubblicati dalla BTS nel 1983 e 1990 [127,145]. Il primo trial consisteva in 1.618 pazienti che frequentavano un ambulatorio pneumologico. Sono stati valutati quattro metodi: solo il consiglio del medico, il consiglio più un opuscolo, il consiglio più l'opuscolo più un chewing-gum placebo, e tutti e tre più il chewing-gum con 2 mg di nicotina e 4 visite di follow up. Il tasso totale del risultato di un anno è stato di 9,7% (95% CI: 8,311,3%), senza alcuna differenza significativa tra i 4 gruppi di trattamento [127]. Comunque, Fagerström [79] ha suggerito che ci potrebbero essere stati diversi errori metodologici in questo studio. Il secondo e terzo studio BTS sulla cessazione dell'abitudine al fumo sono stati trial multicentrici su 2.854 pazienti esterni (87% soffrivano di disturbi respiratori) che frequentavano ospedali o ambulatori pneumologici [145]. Lo studio A ha paragonato l'effetto del consiglio del medico di smettere di fumare con lo stesso consiglio integrato da un impegno firmato a cessare di fumare in una data particolare e da due visite con un operatore sanitario ed alcune lettere di incoraggiamento inviate dal medico al paziente. Si è riscontrato che questi due interventi hanno ottenuto lo stesso risultato. Lo studio B ha paragonato 4 gruppi: il consiglio del medico versus il consiglio più l'intenzione firmata versus il consiglio più le lettere versus il consiglio più le lettere più l'intenzione firmata. L'intenzione firmata non ha influito sull'esito, mentre le lettere hanno aumentato il risultato dal 5,1 all'8,7%. Una successiva stratificazione ed un'analisi combinata dei due studi hanno riscontrato che il 5% smetterebbe con il solo consiglio del medico e che l'incoraggiamento postale incrementerebbe il tasso di successo di oltre la metà. Anche le visite ambulatoriali sembravano aumentare il tasso di successo (Tabella III). L'implementazione della cessazione di routine dell'abitudine al fumo in una clinica cardiotoracica è stata riferita in uno studio danese [146] che ha coinvolto 197 fumatori leggeri (< 10 sigarette al giorno) e 310 fumatori (> 10 sigarette al giorno) che non erano interessati a partecipare ad un formale programma di cessazione dell'abitudine al fumo. Le infermiere dell'ambulatorio pneumologico applicavano un intervento minimale consistente in: consiglio dell'infermiere a smettere di fumare (durata: 5 minuti), valutazione del CO, un opuscolo ed una lettera di incoraggiamento dopo 4-6 settimane. Al gruppo di controllo sono state fatte alcune domande sul fumo ed è stato valutato il loro CO, senza averne risposta. La prevalenza puntuale di astinenza a un anno è stata dell'8,7 versus 3,6% (p = 0,025), mentre il tasso di successo continuativo è stato 3,1 versus 1,2% (non significativo) [146]. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 29 Visite ambulatoriali Consiglio del medico Intervento (lettere) Nessuna 5 9 Una o più 9 13 I dati sono presentati come tassi percentuali di cessazione in seguito alla stratificazione secondaria di due studi (n = 2.854) per stimare gli effetti dell'intervento e delle visite ambulatoriali. Tratto da [144]. In conclusione si è riscontrato che il consiglio del medico e dell'infermiere supportato da lettere di incoraggiamento è più efficace del solo consiglio in pazienti ambulatoriali con malattie respiratorie, con un tasso di astinenza ad un anno di circa il 10%. TRATTAMENTI FARMACOLOGICI PER LA CESSAZIONE DEL FUMO Trattamenti di prima linea La terapia farmacologica è un'importante pilastro del trattamento della dipendenza da tabacco. La NRT e/o il bupropione a rilascio controllato (SR), utilizzati insieme ad interventi comportamentali, sono raccomandati come farmacoterapia di primo impiego dalle attuali linee guida per la disassuefazione dal fumo [10,147-150]. Eccetto che in presenza di controindicazioni, questi farmaci dovrebbero essere usati in quasi tutti i pazienti che tentano di smettere di fumare. I fumatori di almeno dieci sigarette al giorno che sono pronti a smettere dovrebbero essere incoraggiati ad utilizzare NRT o bupropione per aiutare la disassuefazione. Il personale sanitario che fornisce interventi di disassuefazione dal fumo dovrebbe dare ai pazienti fumatori informazioni accurate e consigli su questi prodotti. Terapia sostitutiva con nicotina (NRT) La dipendenza da nicotina è un elemento significativo della dipendenza da tabacco, per cui l'approccio standard alla cessazione farmacologica dell'abi- tudine al fumo è stata l'uso di NRT. Questo trattamento ha lo scopo di rimpiazzare la nicotina ottenuta dalle sigarette, riducendo in questo modo i sintomi da astinenza dovuti alla cessazione. Tutte le forme di NRT (gomme da masticare, cerotti transdermici, inalatori orali, spray nasali, compresse sublinguali e pastiglie) sono ugualmente efficaci e ben tollerati (Tabella IV) [140,151-154] Una metanalisi Cochrane ha dimostrato che la NRT aiuta i fumatori a smettere (Tabella V) [140]. Un totale di 105 studi randomizzati controllati con placebo hanno mostrato un OR 1,8 (95% CI tra 1,7 e 1,9) a favore della NRT contro il placebo. In termini assoluti, questo significa un incremento del 7% nel tasso di astinenza a 6 e 12 mesi usando la NRT per 3 mesi; aggiungendo un supporto comportamentale alla NRT il tasso di astinenza aumenta di un ulteriore 7-8%. Nella metanalisi Cochrane, il tasso di astinenza a un anno è stato del 17% per la NRT e del 10% per il gruppo di controllo. La recidiva precoce è abbastanza comune negli studi con NRT ed è un predittore di fallimento della disassuefazione. I dosaggi raccomandati di NRT variano in relazione al grado di dipendenza. L'uso dovrebbe essere limitato alla durata autorizzata nella prescrizione, tuttavia può essere continuato ben oltre i tre mesi in caso di perdurante dipendenza da nicotina. La NRT dovrebbe essere sospesa se il fumatore inizia nuovamente a fumare [151,152,154]. C'è scarsa evidenza diretta sul fatto che alcune formulazioni di NRT siano più efficaci di altre, pertanto la decisione sul prodotto da utilizzare dovrebbe L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement TABELLA III: RISULTATI AD UN ANNO DI: CONSIGLIO DEL MEDICO, LETTERE, VISITE TABELLA IV: FORMULAZIONI DI TERAPIA SOSTITUTIVA NICOTINICA DISPONIBILI SUL MERCATO Formulazioni Prodotti commerciali Cerotti transdermici alla nicotina 5 mg, 10 mg, 15 mg/16 h (Nicorette®, Pfizer) 7 mg, 14 mg, 21 mg/24 h (Nicotinell® TTS 10, TTS 20, TTS 30, Novartis) 7 mg, 14 mg, 21 mg/24 h (NiQuitin® CQ, GSK) Gomme da masticare alla nicotina 2 mg, 4mg (Nicorette®, Pfizer; Nicotinell®, Novartis Formulazioni orali alla nicotina 2 mg compresse sublinguali (Nicorette® Microtab®, Pfizer) 1 mg pastiglie (Nicotinell®, Novartis) 2 mg e 4 mg pastiglie (Niquitin® CQ, GSK) Inalatori alla nicotina 10 mg cartucce da inalare più bocchino (Nicorette® Inhaler, Pfizer) Spray nasale alla nicotina 0,5 mg per spruzzo in ciascuna narice (Nicorette® Spray nasale, Pfizer) Definizione delle abbreviazioni: GSK, GlaxoSmithKline; TTS, sistema terapeutico transdermico. MRM 29 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 30 TABELLA V: METANALISI COCHRANE DEGLI EFFETTI DELLE DIFFERENTI FORMULAZIONI DI TERAPIA SOSTITUTIVA CON NICOTINA (NRT) Terapia per smettere di fumare NRT vs Placebo Controlli 10 Tutte le formulazioni di NRT 1,77 (1,7-1,9) 17 Gomme da masticare alla nicotina 1,66 (1,5-1,8) 17 Cerotti alla nicotina 1,81 (1,6-2,0) 14 Inalatori alla nicotina 2,14 (1,4-3,2) 17 Spray nasale alla nicotina 2,35 (1,6-3,4) 24 Compresse sublinguali/pastiglie alla nicotina 2,05 (1,9-3,3) 17 Gomme da 4 mg vs gomme da 2 mg 2,20 (1,5-3,3) Gomme a dosaggio fisso vs gomme ad libitum 1,29 (0,90-1,9) Combinazione di due formulazioni di NRT vs singola formulazione 1,42 (1,1-1,8) Bupropione SR* 2,06 (1,8-2,4) I dati sono presentati come Odds ratio (intervallo di confidenza 95%) oppure in %. Numero totale di soggetti analizzati: 39.503. SR = rilascio controllato. I dati sono stati raccolti da [140], eccetto * tratto da [141]. essere guidata dalle preferenze individuali. Sono stati riportati migliori tassi di cessazione in fumatori molto dipendenti che utilizzavano una gomma da 4 mg di nicotina rispetto alla gomma da 2 mg. In alcuni fumatori molto dipendenti, può essere di beneficio combinare due formulazioni diverse di NRT. È stato dimostrato che questa terapia combinata migliora i risultati a breve termine, mentre i risultati a lungo termine sono contrastanti. Non ci sono dimostrazioni di risultati diversi nell'utilizzo dei cerotti da 16 o da 24 ore né che il prolungamento del trattamento oltre i tre mesi migliori il tasso di astinenza, mentre cerotti a maggiore contenuto di nicotina hanno ottenuto risultati migliori ma in misura modesta. Utilizzare cerotti a dosaggio decrescente non è risultato più efficace che smettere improvvisamente il loro uso. Controindicazioni relative all'uso di NRT sono le malattie cardiovascolari, l'ipertiroidismo, il diabete mellito, l'ulcera peptica e stati di grave insufficienza renale o epatica. Tuttavia è stato dimostrato che la NRT può essere data in tutta sicurezza in caso di coronaropatie; inoltre dovrebbe essere prescritta in tutti i casi nei quali smettere di fumare è uno dei più importanti fattori in grado di influenzare la prognosi. Nel caso di donne in gravidanza o allattamento si dovrebbe sempre fare un bilancio rischi-benefici dell'uso di NRT, tenendo presente il fatto che continuare a fumare fornisce alla donna più nicotina della NRT. La sostituzione di nicotina è in genere ben tollerata. Gli effetti avversi più comuni sono irritazioni locali dovute appunto alla nicotina, come ad esempio irritazione cutanea con i cerotti, o irritazioni della mucosa orale o faringea con le formulazioni orali, irritazioni che generalmente si riducono o scompaiono in pochi giorni in seguito allo sviluppo di tolleranza locale. Nei paesi europei, la NRT è disponibile sia su prescrizione, sia come farmaco da banco, sia in libera vendita. 30 MRM Tassi di cessazione NRT Efficacia della NRT nei fumatori affetti da malattie respiratorie Sebbene la disassuefazione dal fumo sia considerata il più importante provvedimento terapeutico nei pazienti affetti da BPCO, pochi studi hanno esaminato l'efficacia dei differenti trattamenti per la cessazione su queste popolazioni di pazienti. Gli studi su pazienti con BPCO e altre patologie respiratorie sono riassunti in tabella VI [155-163]. Uno studio randomizzato in aperto ha indagato quattro differenti regimi di NRT in pazienti con BPCO in un ambulatorio specialistico di medicina respiratoria [146]. I 446 soggetti erano stati indirizzati all'ambulatorio specialistico dai propri medici di medicina generale per una radiografia del torace di routine, prove di funzione respiratoria ed una valutazione diagnostica per la BPCO. I fumatori (di più di 10 sigarette al giorno) erano stati avviati ad un programma di disassuefazione dal fumo condotto da infermiere, con visite di follow up a 2 e 6 settimane e a 3, 6, 9 e 12 mesi. I tassi di astinenza a un anno erano 1,8% per il gruppo trattato con cerotto alla nicotina da 5 mg (definito come “placebo”) dell'8,7% nel gruppo trattato con cerotto alla nicotina da 15 mg, 5,1% per il gruppo trattato con l'inalatore di nicotina e 3,5% per il trattamento combinato con inalatore e cerotto da 15 mg [146]; il tasso medio di astinenza per i tre trattamenti attivi era del 5,6% (p < 0,01). In un altro studio randomizzato a doppio cieco, controllato con placebo, sette ambulatori di medicina respiratoria arruolarono 370 pazienti con BPCO che fumavano una media di 19,6 sigarette al giorno (con una media di 42,7 pacchetti-anno) e con un FEV1 medio del 56% del teorico [161]. I soggetti erano trattati con compresse sublinguali di nicotina da 2 mg o placebo per 12 settimane, combinati con un supporto a bassa intensità (quattro visite e sei telefonate) oppure con un supporto ad alta intensità (sette visite più cinque telefonate) forniti da infermiere. I tassi di astinenza MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 31 Primo autore/Società (biblio.) n pazienti Tasso di cessazione continuativa Intervento p Controlli/Terapia usuale Pazienti ospedalizzati CAMPBELL [156] 111 20 (+NRT/placebo) 20 NS CAMPBELL [157] 234 21 (+NRT/placebo) 14 NS MILLER [158] 1402* 1482* 14 (+NRT) 19 (+NRT) 13 13 NS < 0,01 LEWIS [159] 185 † 6,5 (+placebo) 9,7 (+NRT) 4,9 4,9 NS NS British Thoracic Society [127] 1550 9,8 (+NRT/placebo) 8,9 NS MURRAY [61] 5887 28 (+NRT) 7 < 0,001 TØNNESEN [160] 446 TASHKIN [8] 404 † HAND [6] TØNNESEN [161] Pazienti ambulatoriali 5,6 (+NRT/placebo‡) 1,8 < 0,01 23 (bupropione/placebo) 16 < 0,01 245 15 (+NRT) 14 NS 370 17 (+NRT/placebo) 10 < 0,001 L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement TABELLA VI: TASSI DI CESSAZIONE A UN ANNO DA STUDI CLINICI DI CESSAZIONE IN PAZIENTI FUMATORI AFFETTI DA MALATTIE RESPIRATORIE Definizione delle abbreviazioni: NRT, terapia sostitutiva con nicotina; NS, non significativo; *, interventi intensivi e non intensivi nello stesso studio; † , tasso di successo a 6 mesi; ‡, come placebo è stato utilizzato il cerotto da 5 mg. Tratto da [155] mod, con il permesso dell'editore. espressi in prevalenza puntuale furono superiori in misura statisticamente significativa con le compresse sublinguali rispetto al placebo sia a 6 mesi (23% contro 10%) sia a un anno (17% contro 10%). Non c'era differenza significativa tra il supporto ad alta e quello a bassa intensità. Il punteggio del St. George Respiratory Questionnaire (SGRQ) migliorava significativamente negli astinenti rispetto ai non astinenti; le variazioni dei punteggi medi dopo un anno erano di -10,9 contro -2,9 per il punteggio totale e -28,6% contro -2,3% per il punteggio dei sintomi. Questo studio ha dimostrato l'efficacia a lungo termine della NRT per la disassuefazione della popolazione generale di fumatori con BPCO, indipendentemente dal consumo giornaliero di sigarette, dato che erano stati inclusi anche fumatori di meno di dieci sigarette al giorno. I tassi di disassuefazione erano compresi nello stesso range di quelli dei fumatori sani e l'astinenza migliorava il punteggio del SGRQ [161]. Il Lung Health Study [152] è stato uno studio multicentrico randomizzato controllato messo a punto per investigare un programma comprendente un intervento di disassuefazione dal fumo e uso continuato di un broncodilatatore inalatorio in 5.887 fumatori con BPCO da lieve a moderata, con un FEV1 medio di 2,700 ± 0,6 L (75% del teorico). I soggetti avevano un'età media di 48 anni e un'anamnesi di fumo di 40 pacchetti-anno. Inizialmente è stato fornito un programma intensivo di disassuefazione da fumo articolato in 12 sessioni, con gomme alla nicotina in aggiunta a trattamento comportamentale, che è stato seguito da un programma di prevenzione delle recidive ogni 4 mesi per 5 anni. All'ingresso nello studio, veniva fornito dal medico un deciso consiglio di smettere e veniva fis- sata una data precisa per l'inizio del tentativo. La gomma alla nicotina veniva usata in modo aggressivo. Il tasso continuativo di cessazione fu alto nel gruppo oggetto di intervento e si ridusse poi, come il solito, durante il periodo dello studio e cioè dal 35% dopo un anno al 22% dopo 5 anni, contro il 10 e 5% rispettivamente nel gruppo di controllo (cioè trattato come usualmente). Il tasso di cessazione trasversale aumentava significativamente durante i 5 anni fino al 39% nel gruppo di intervento e al 22% nel gruppo di controllo (Figura 1). L'altra importante scoperta era che la disassuefazione dal fumo riduceva significativamente sia il declino del FEV1 dovuto all'età sia la mortalità. Tuttavia dato che la gomma alla nicotina non era somministrata in modo randomizzato, non era possibile analizzarne l'efficacia in questo studio. Complessivamente, questo approccio a lungo termine ha dimostrato che programmi di disassuefazione aggressivi, intensivi e ripetuti possono ottenere tassi di cessazione elevati nel lungo periodo in fumatori con lieve ostruzione delle vie aeree. Bupropione SR Il cloridrato di bupropione è un farmaco antidepressivo (un aminochetone) che si è dimostrato efficace nel promuovere la disassuefazione nei fumatori che fumano più di 10 sigarette al giorno e che sono motivati a smettere. Il bupropione inibisce il riassorbimento della noradrenalina e della dopamina da parte delle cellule neuronali, con effetto minimo sul riassorbimento della serotonina e nessun effetto inibitore sulle mono-amino-ossidasi. È stato dimostrato che il farmaco riduce l'attività di questi neuroni che rilasciano dopamina e conseguentemente può disattivare i circuiti della ricomMRM 31 FIGURA 1: PREVALENZA PUNTUALE DI CESSAZIONE DAL FUMO NEL “LUNG HEALT STUDY” (N = 5.587) 40 popolazione trattata popolazione di controllo 35 30 Tasso di cessazione (%) Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 32 25 20 15 10 5 0 1 2 3 4 5 Tempo dall’inzio dello studio (anni) Popolazione trattata = gruppo trattato con intervento terapeutico; popolazione di controllo = terapia usuale. Tratto da [152], con il permesso dell’editore. pensa e ridurre il bisogno di fumare. Recenti studi in vitro indicano che il bupropione, oltre ad inibire il riassorbimento della noradrenalina e della dopamina, può essere un inibitore funzionale non competitivo dei recettori nicotinici per la acetilcolina. Il bupropione SR è considerato un'opzione utile per i fumatori che tentano di smettere di fumare per la prima volta, specialmente coloro che non possono tollerare la NRT, o che preferiscono un trattamento non nicotinico o che sono reduci da un fallimento di un tentativo per smettere attuato con NRT (26,16-19]. Per la disassuefazione dal fumo la dose raccomandata di bupropione SR è di 150 mg al giorno per la prima settimana, successivamente aumentato a 300 mg al giorno (150 mg per due al di). Ai fumatori che utilizzano il bupropione SR viene raccomandato di continuare a fumare fino al giorno fissato per smettere, di solito una settimana dopo l'inizio del trattamento. Una dose di mantenimento ridotta (150 mg al giorno) è raccomandata per i fumatori più anziani, o per coloro affetti da insufficienza renale o epatica o per quelli che pesano meno di 45 chili. La durata raccomandata del trattamento per la disassuefazione dal fumo è compresa fra 7 e 12 settimane. Il trattamento dovrebbe essere accompagnato da un programma di supporto motivazionale, che metta in luce informazioni aggiuntive sulla cessazione e sulla prevenzione delle ricadute. Il bupropione SR è un farmaco che richiede la prescrizione medica. I più comuni effetti collaterali sono disturbi del sonno e secchezza delle fauci. Un effetto grave ma raro (inferiore a uno su mille) è costituito dalle convulsioni [141]. Il farmaco è controindicato nei pazienti che siano o 32 MRM siano stati affetti da epilessia, e dovrebbe essere utilizzato con estrema cautela nei fumatori che soffrono di patologie che abbassano la soglia convulsivante, come ad esempio anamnesi di trauma cranico o di abuso alcolico. Il bupropione interagisce con un certo numero di farmaci comunemente utilizzati compresi alcuni anti depressivi, gli antiaritmici di tipo 1c e gli anti-psicotici; cautela è anche richiesta nel prescrivere la dose a pazienti sofferenti di diabete trattato con farmaci ipoglicemizzanti orali o insulina, e in pazienti che fanno uso di farmaci che abbassano la soglia convulsivante (ad esempio antipsicotici, antidepressivi, teofillina e steroidi sistemici). Inoltre, il bupropione è controindicato in pazienti con anamnesi di anoressia nervosa e bulimia, grave necrosi epatica, o disordini bipolari. Si dovrebbe evitare di somministrare il bupropione insieme a un inibitore della monoamino ossidasi e almeno due settimane dovrebbero passare tra la fine del trattamento con tale farmaco e l'inizio di quello con bupropione [9,140,164-167]. Efficacia del bupropione SR nei pazienti fumatori affetti da BPCO L'efficacia clinica del bupropione SR nella popolazione generale di fumatori è stata verificata in numerosi studi ben controllati [8,162,163,168170]. Una metanalisi di 19 studi ha verificato un OR di 2,06 (95% CI: 1,8-2,4) a favore del bupropione SR contro placebo [163]. Oltre agli studi clinici randomizzati, l'efficacia del bupropione SR è stata dimostrata negli ambulatori ospedalieri ed extra ospedalieri. Un periodo di trattamento da 7 a 12 settimane con bupropione SR sembra la durata adeguata per la disassuefazione dal fumo, sebbene trattamenti più prolungati allunghino i tempi della recidiva. Un riciclo (cioè un trattamento ripetuto con bupropione in fumatori che sono stati trattati precedentemente con questo farmaco) dovrà essere tentato dal momento che è stato dimostrato aumentare le possibilità di successo finale [171]. Il trattamento con bupropione SR dovrebbe essere accompagnato da un programma di supporto motivazionale che fornisca informazioni supplementari sulla disassuefazione e sulla prevenzione delle ricadute [9-12,147,162]. Sono molto pochi gli studi che hanno utilizzato il bupropione SR per la disassuefazione dal fumo nei pazienti con malattie croniche come ad esempio la BPCO o le malattie cardiovascolari. Uno studio multicentrico, controllato con placebo, condotto da Tashkin e coll. [8] ha esaminato l'efficacia del bupropione SR per 12 settimane accompagnato a visite settimanali per la disassuefazione dal fumo su 404 pazienti affetti da BPCO lieve o moderata che fumavano una media di 28 sigarette al giorno. Questi soggetti erano dipendenti in misura relativamente elevata, con un punteggio medio di FTND di 7. I tassi di astinenza continuativa nelle settimane dalla IV alla VII erano significativamente più alti nei soggetti che ricevevano bupropione SR rispetto a quelli che ricevano il placebo (28 contro 16%, p = 0,003). I tassi di astinenza continuativa dalla IV alla MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 33 Trattamenti di seconda linea La nortriptilina, un antidepressivo triciclico, è l'unico altro antidepressivo che si sia dimostrato efficace per la disassuefazione dal fumo. La dose di nortriptilina per la disassuefazione dal fumo è 75-150 mg al giorno. Una metanalisi di quattro studi clinici ha evidenziato un OR 2,8 (95% CI: 1,7-4,6) per il tasso di cessazione a un anno per la nortriptilina contro placebo [141]. Tuttavia ci sono molte controindicazioni all'utilizzo della nortriptilina, compresi i frequenti effetti collaterali anticolinergici e particolarmente i disturbi della conduzione cardiaca e l'ipotensione ortostatica. Numerosi altri antidepressivi, compresi gli inibitori selettivi del riassorbimento della serotonina (cioè doxepina, fluoxetina, sertralina, moclobemide, e venlafaxina) non si sono dimostrati efficaci nella disassuefazione dal fumo. La clonidina, un'imidazolina usata nel trattamento della ipertensione, ha un'efficacia limitata come terapia per la cessazione del fumo [174,175]. È stata raccomandata come terapia di seconda linea dalle linee guida statunitensi per la disassuefazione [10]. Tuttavia gli effetti collaterali associati alla terapia con clonidina, come sonnolenza, astenia e secchezza delle fauci, può limitarne l'uso [174] e gli autori di questo documento la ritengono obsoleta. Nuovi farmaci La vareniclina è stata approvata nella Unione Europea, è commercializzata negli Stati Uniti e sarà commercializzata tra la fine del 2006 e l'inizio del 2007 nella maggior parte dei Paesi europei (attualmente è commercializzata nella maggior parte dei Paesi Europei, ndr). Il rimonabant è un farmaco disponibile sia negli Stati Uniti sia in Europa, ma è stato approvato come medicamento per il calo ponderale piuttosto che come farmaco per la disassuefazione dal fumo. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement XII settimana (18 contro 10%) e dalla IV alla XXVI settimana (16 contro 9%) erano anche più elevati nel gruppo trattato con bupropione SR (p < 0,05). I tassi di cessazione espressi come prevalenza puntuale a 6 mesi erano più elevati in quelli trattati con bupropione SR che in quelli che ricevevano il placebo (23 contro 16%), ma al dodicesimo mese i tassi di astinenza continuativa non differivano in misura statisticamente significativa. Approssimativamente un terzo della popolazione studiata che inizialmente non desiderava o non era capace di smettere di fumare fu in grado di ridurre il fumo di più del 50% durante la terapia con bupropione SR; il 14% di questa popolazione riuscì a raggiungere l'astinenza. I tassi di astinenza riportati sono molto più bassi di quelli osservati in studi similari nei quali il bupropione SR era stato impiegato in soggetti sani, e ciò suggerisce che i pazienti con BPCO possano essere fumatori relativamente più recalcitranti a smettere. Considerata l'urgente necessità per i pazienti con BPCO di smettere di fumare, sembra opportuno impiegare programmi più intensivi che possano ottenere risultati maggiori in termini di disassuefazione in questa popolazione ad alto rischio. Il bupropione SR è stato tollerato bene in questi studi clinici e sembra avere un buon profilo di sicurezza nei pazienti affetti da BPCO. È importante che sia stata osservata l'assenza di effetti clinici significativi sulla pressione arteriosa media dei fumatori, compresi quelli affetti da ipertensione arteriosa, e che sia stata dimostrata un'attenuazione dell'incremento di peso dopo disassuefazione dal fumo, particolarmente nelle donne. Pochi studi hanno confrontato il bupropione SR con NRT nei confronti della cessazione o investigato gli effetti del trattamento combinato. Tuttavia, la combinazione di bupropione SR e NRT sembra sicura ed è usata da molti clinici per i fumatori più dipendenti [172,173], sebbene manchino degli studi completi. La scelta del trattamento combinato dovrebbe essere basato sulle preferenze del paziente e sulla considerazione degli effetti collaterali e di eventuali comorbosità. La scelta del trattamento può anche essere influenzata dalla disponibilità sul mercato e dal costo di acquisto di questi farmaci. La Vareniclina La vareniclina è un agonista parziale del sottotipo di recettori neuronali nicotinici composti dalle subunità alfa4 e beta2. Recenti ricerche suggeriscono un ruolo primario per questi recettori nicotinici nella dipendenza nicotinica e nel bisogno di fumare. Gli studi preclinici suggeriscono che la vareniclina inizialmente stimola i recettori alfa4 beta2 che mediano gli effetti dell'agonista nicotinico sul rilascio di dopamina nel nucleus accumbens (funzione agonista). Se la nicotina viene aggiunta al trattamento con vareniclina, non viene registrato alcun incremento della risposta dopaminica (funzione antagonista). Dato che la vareniclina combina sia la funzione agonista sia quella antagonista, può ridurre la dipendenza nicotinica e può anche ridurre gli effetti dovuti alla astinenza da nicotina [176,177]. La vareniclina è ben assorbita e viene escreta prevalentemente immodificata (92%) nelle urine. Ha un'emivita di 17 ore e richiede 4,3 ore per raggiungere la massima concentrazione [176,177]. Ai fumatori si raccomanda di raggiungere gradatamente in una settimana la dose terapeutica di vareniclina di 1 mg per due volte al dì, smettere di fumare all'ottavo giorno e continuare poi il trattamento per 12 settimane. Sono stati pubblicati i risultati di tre studi clinici di fase tre sulla vareniclina. Due studi, che hanno impiegato protocolli identici, hanno confrontato la vareniclina con placebo e con bupropione SR (Tabella VII). I risultati di fase tre sono simili a quelli ottenuti con gli studi clinici di fase due. I più comuni effetti avversi riportati rispettivamente per vareniclina, bupropione SR e placebo sono stati: nausea (28, 10 e 9%), cefalea (14, 11 e 12%), incubi (12, 6 e 4%). Sebbene la nausea, in particolare, fosse l'effetto più frequentemente riportato con vareniclina, la percentuale di drop-out dovuti agli effetti collaterali non è stata più elevata per vareniclina (10%), rispetto a bupropione (14%) ed al placebo (8%) [176-177]. In un terzo MRM 33 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 34 TABELLA VII: TASSI DI CESSAZIONE CONTINUATIVA DALLA SETTIMANA 9 ALLA 52 IN DUE STUDI CLINICI DI FASE TRE CON VARENICLINA PER LA DISASSUEFAZIONE DAL FUMO Primo autore (biblio.) Tasso di cessazione (%) p Placebo Vareniclina 2 mg al dì Bupropione SR 300 mg al dì GONZALEZ [176] 8,4 21,9 16,1 Vareniclina vs placebo p < 0,001 Vareniclina vs bupropione SR p < 0,057 Bupropione SR vs vareniclina p < 0,001 JORENBY [177] 10,3 23,0 15,0 Vareniclina vs bupropione SR p < 0,001 Bupropione SR vs placebo p < 0,001 Vareniclina vs placebo p < 0,001 lavoro è stata studiata la durata del trattamento con vareniclina, 12 settimane contro 24; un piccolo ma significativo effetto è stato osservato a favore del periodo di 24 settimane [177]. La vareniclina impiega un nuovo interessante meccanismo di azione per il trattamento della dipendenza da tabacco. In uno studio di mantenimento, 1.927 fumatori sono stati trattati in aperto con vareniclina per 3 mesi, con un tasso di prevalenza puntuale di cessazione a tre mesi del 64,1%. I fumatori che avevano raggiunto l'astinenza continuarono l'assunzione del farmaco per altri tre mesi in doppio cieco con un tasso di cessazione dalla 13a alla 52a settimana di 43,6% contro il 36,9% (p = 0,02), suggerendo che alcuni fumatori possono beneficiare di un ciclo di terapia con vareniclina per 6 mesi per mantenere l'astinenza [178]. I risultati degli studi di fase tre suggeriscono che la vareniclina può rappresentare un miglioramento dell'attuale trattamento per la disassuefazione dal fumo. Poiché sono stati pubblicati solo pochi studi sulla vareniclina e poiché mancano sia studi al di fuori degli ambulatori specialistici per smettere di fumare, sia studi condotti in ambiente di medicina generale con supporto minimale, sia di studi su pazienti BPCO e sia di studi post-marketing, gli autori di queste linee guida considerano la vareniclina come farmaco di seconda linea per la disassuefazione. Ci si attende che in seguito a ulteriore documentazione ed esperienza la vareniclina divenga un farmaco di primo impiego per la disassuefazione dal fumo. Il Rimonabant Un altro approccio alla farmacoterapia per la disassuefazione dal fumo è l'impiego di farmaci non nicotinici al fine di influenzare gli effetti della nicotina sulle vie nervose dell'encefalo che sono implicate nella dipendenza da nicotina/tabacco. In animali da esperimento è stato dimostrato che il blocco dei recettori cannabinoidi CB1 con il rimonabant riduce la ricerca di cibo e diminuisce l'autosomministrazione di nicotina e il turnover della dopamina dovuto a stimolazione da nicotina nel nucleus accumbens [179]. In più, il rimonabant attenua il ripristino del comportamento di ricerca della nicotina, evocato da esposizione non contingente ad uno stimolo condizionato, dopo cessazione dell'autosomministrazio34 MRM ne di nicotina [179]. Pertanto, gli scienziati hanno recentemente ipotizzato che la stimolazione dei recettori CB1 da parte degli endocannabinoidi nell'encefalo possa avere un ruolo importante nello sviluppo e nel mantenimento della dipendenza da nicotina e fumo, e che il rimonabant esplichi i suoi effetti nei soggetti dipendenti inibendo questo ruolo del sistema degli endocannabinoidi [179]. Sono disponibili i risultati di due grandi studi multicentrici di fase 3 (Studies with rimonabant and tobacco use (STRATUS) USA and Europe) [180,181] condotti con protocolli simili. Il rimonabant è stato provato ai dosaggi di 5 mg e 20 mg al giorno contro placebo e il trattamento attivo è durato per dieci settimane. Nello studio condotto negli Stati Uniti, i tassi di cessazione alla decima settimana erano il 28% per il rimonabant 20 mg, il 16% per il rimonabant da 5 mg e il 16% per il placebo [180]. La differenza fra la dose da 20 mg e il placebo era altamente significativa (p < 0,005). Nello studio europeo i tassi di astinenza alla decima settimana erano 25, 24 e 20% rispettivamente (non significativi dal punto di vista statistico). Alla decima settimana, tra i soggetti astinenti, gli incrementi di peso erano stati rispettivamente di 0,7 nel gruppo a 20 mg, 2 in quello a 5 mg e 3 kg nel gruppo placebo. I più frequenti effetti collaterali riportati con il rimonabant erano nausea, diarrea, vomito, infezioni del tratto urinario, ansia e infezioni delle vie aeree superiori. Sebbene il rimonabant abbia dimostrato una qualche efficacia nel breve periodo, i suoi effetti non sembrano essere significativamente migliori di quelli dei trattamenti per la disassuefazione attualmente disponibili. Tuttavia, data la sua documentata miglior efficacia nel trattamento dell'obesità [181], si può supporre che il rimonabant possa essere utile nei fumatori sovrappeso, per i quali un incremento ponderale può essere una barriera insormontabile alla cessazione. Punti chiave: farmacoterapia e disassuefazione dal fumo 1. La NRT e il bupropione SR sono trattamenti di prima linea per la disassuefazione dal fumo (livello di evidenza A). I fumatori che tentano di smettere dovrebbero essere incoraggiati a usare questi farmaci per aiutare la cessazione, tranne i casi nei MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 35 ALTRI INTERVENTI Agopuntura e laser terapia Una revisione Cochrane di 20 studi clinici non ha trovato alcun beneficio nell'agopuntura confrontata con l'agopuntura-placebo [182]. È stato pubblicato un singolo studio sulla laser terapia in 320 adolescenti, ma non ha riportato alcun effetto della laser terapia [183]. Per questo l'agopuntura e la laser terapia non possono essere raccomandati come ausili per la cessazione del fumo. Ipnosi Una revisione Cochrane di nove piccoli studi clinici di ipnosi non li ha trovati maggiormente efficaci di altri trattamenti comportamentali [184]. L'ipnosi è difficile da valutare in assenza di una procedura placebo per controllarne gli effetti aspecifici e non c'è alcun evidenza per supporre che l'ipnosi da sola abbia alcun effetto nel trattamento per la disassuefazione dal fumo. Non c'è alcun evidenza che l'ipnosi, l'agopuntura o la laser terapia abbiano alcun effetto nella disassuefazione dal fumo. LA RIDUZIONE DEL FUMO Definizione Di solito si raccomanda ai fumatori di smettere completamente il giorno scelto per la cessazione dal momento che la maggior parte di fumatori che riducono lentamente e progressivamente hanno una elevata probabilità di recidiva. Questo è stato documentato in parecchi studi clinici di disassuefazione dal fumo, per esempio nello studio Collaborative European Anti-Smoking Evaluation (CEASE) [165]. La completa astinenza durante la prima settimana dalla cessazione era un fattore predittivo molto forte di completa astinenza ad un anno: il 25% nei fumatori che avevano smesso completamente in confronto al 4% per quelli che avevano fumato durante la prima settimana [165]. Tuttavia, molti fumatori preferirebbero ridurre il numero di sigarette fumate al giorno piuttosto che smettere completamente. Lo scopo della riduzione del fumo è ampliare l'accesso alla disassuefazione, arruolando fumatori che al momento sono incapaci di - o non desiderano - smettere di colpo, ma vorrebbero ridurre il fumo. Come si vedrà più oltre, il concetto di riduzione del fumo rende possibile reclutare un nuovo gruppo di fumatori, che non sono interessati alla cessazione immediata. Il processo di riduzione dovrebbe essere considerato un passaggio verso la disassuefazione totale. La definizione di riduzione del fumo è una diminuzione nel numero di sigarette (oppure nella quantità di tabacco) fumate al giorno. La soglia del 50% o più di riduzione del numero di sigarette quotidiane è stata scelta arbitrariamente nella maggior parte degli studi, confermandola con una diminuzione nei livelli di monossido di carbonio espirato [185,186]. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement quali sussistano controindicazioni (livello di evidenza A). 2. Differenti formulazioni di NRT (gomme, cerotti, inalatori, spray nasali, pastiglie e compresse sublinguali) sono ugualmente efficaci nei trattamenti per la disassuefazione dal fumo (livello di evidenza A). 3. La combinazione fra un cerotto alla nicotina ed un'altra formulazione farmaceutica di NRT autosomministrata può essere più efficace di una singola formulazione di NRT (livello di evidenza B). 4. La NRT dovrebbe essere usata per aiutare la cessazione in tutti i fumatori con BPCO, indipendentemente dalla gravità della malattia e dal numero di sigarette fumate (livello di evidenza B). 5. Il trattamento combinato con bupropione SR e NRT potrebbe essere più efficace nei forti fumatori (livello di evidenza C). 6. Sia NRT che il bupropione SR sono efficaci e ben tollerati nei fumatori con malattie cardiovascolari stabili e nei pazienti affetti da BPCO (livello di evidenza A). 7. La nortriptilina può essere usata come farmaco di seconda linea per trattare la dipendenza dal tabacco (livello di evidenza B). 8. Non vi sono attualmente evidenze che gli inibitori selettivi del riassorbimento della serotonina (SSRIs) abbiano un qualche effetto nella disassuefazione dal fumo. 9. La vareniclina può avere un effetto terapeutico addizionale nel trattamento per la disassuefazione dal fumo ed è considerata un farmaco di seconda linea fino a quando non saranno disponibili maggiore documentazione ed esperienza (livello di evidenza B). 10. Visite periodiche di follow up sono importanti e sono correlate ad un miglior tasso di successo nel lungo periodo (livello di evidenza B). Sulla base di queste conclusioni e raccomandazioni, è stato messo a punto l'algoritmo per la disassuefazione dal fumo che è mostrato nella figura 2. Studi di popolazione In uno studio di intervento di medicina di comunità in differenti città condotto negli Stati Uniti (Community Intervention Trial for Smoking Cessation; COMMIT) focalizzato sulla disassuefazione assistita, il 40% di fumatori ridusse il proprio fumo e mantenne questa riduzione per tre anni [187]. Un tasso di riduzione assai più basso a cinque anni è stato riportato da uno studio osservazionale di popolazione in Danimarca (il Copenhagen Population Study), che comprendeva 3.791 fumatori; non venivano offerti interventi di alcun genere per la cessazione o la riduzione [188]. Nei maschi venne osservata una riduzione del fumo del 13% a cinque anni, con una diminuzione (± DS) da una media di 31 ± 12 ad una di 16 ± 9 sigarette al giorno. Il tasso di cessazione dei maschi fu di circa 9%, mentre il 78% si dimostrò stabile riguardo all'abitudine al fumo. Nelle femmine il tasso di riduzione fu del 9% da 27±11 a 13 ± 7 sigarette al giorno. Il tasso di cessazione nelle femmine fu del 7%, l'84% non cambiò la propria abitudine al fumo. MRM 35 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 36 FIGURA 2: ILLUSTRAZIONE DELLE FASI RACCOMANDATE NELLA DISASSUEFAZIONE DAL FUMO E DEGLI INTERVENTI DI PRIMA LINEA APPROVATI SI NO Chiedere al/alla paziente se fuma Registrare lo stato di fumatore con regolarità Prevenire le recidive in quelli che hanno smesso da meno di 1 anno Non è richiesto alcun intervento Incoraggiare l’astinenza continuativa Raccomandare Offrire una assistenza personalizzata per smettere NO Valutare Determinare la motivazione a smettere Promuovere la motivazione a smettere SI Valutare Misurare il grado di motivazione e aiutare il paziente con un piano per smettere, fornire un trattamento appropriato Fissare una data per smettere Fornire un counselling pratico Raccomandare l’uso di farmacoterapia Raccomandare supporto comportamentale Specificare il trattamento farmacologico basandolo sulle indicazioni cliniche e sulle preferenze del paziente Raccomandare i trattamenti di prima linea, per esempio bupropione SR o NRT Considerare le controindicazioni per ciascun paziente Bupropione Considerare il supporto comportamentale Trattamento sostitutivo con nicotina cerotti/gomme/pastiglie/inalatori/spray nasali/compresse sublinguali Considerare il supporto comportamentale Considerare il trattamento combinato Organizzare il follow up Organizzare il controllo (follow up) Disassuefazione raggiunta Rinforzare il tentativo del paziente Fornire un feedback positivo Fornire consigli per prevenire le recidive Recidiva Tempistica Subito dopo la data di cessazione (prima settimana) il secondo controllo entro il primo mese Azioni Usare strategie motivazionali Discutere paure e problemi Lavorare su nuove strategie di gestione (coping strategies) Essere di supporto e aiutare il paziente a capire le ragioni per la recidiva Controllare l’aderenza alla terapia e identificare il problema Considerare un trattamento più intensivo Attendere tre mesi prima di un nuovo tentativo di cessazione 36 MRM Promuovere la motivazione MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 37 Riduzione del danno Un altro modo per ridurre il danno da fumo può essere ottenuto attraverso una modifica dei prodotti derivati dal tabacco [192,193]. Per i fumatori non motivati a smettere potrebbe essere di beneficio fumare una sigaretta meno pericolosa. Inoltre il tabacco non fumato (masticato oppure inalato attraverso il naso) potrebbe essere un'alternativa al fumo, con rischi per la salute ridotti rispetto al fumo stesso [194]. Implementazione della riduzione del fumo Il principio della riduzione del fumo dovrebbe essere proposto ai pazienti con malattie respiratorie che fumano e che non sono motivati a smettere. Ad essi si dovrebbe prescrivere NRT (gomme alla nicotina o inalatore) per 3 mesi, raccomandando loro di ridurre il numero di sigarette fumate al giorno di più del 50% durante le prime 1-2 settimane e poi tentare di ridurre ulteriormente. Se il fumatore non ha ridotto di almeno il 50% dopo 3 mesi, la NRT dovrebbe essere sospesa dal momento che le possibilità di una cessazione successiva sono basse. Nei fumatori che hanno ridotto di almeno il 50% al terzo mese, la NRT dovrebbe essere continuata fino al compimento di un anno, ma dopo sei mesi al paziente dovrebbe essere raccomandato di tentare di smettere completamente di fumare. Lo scopo è che il successo nella riduzione del fumo motiverà questo gruppo di fumatori recalcitranti a smettere in modo definitivo. Tuttavia ad oggi l'approccio di riduzione del fumo per la cessazione definitiva è stato testato soltanto in fumatori sani. In sintesi, la riduzione del fumo sembra avere un ruolo per i fumatori che non sono attualmente motivati o capaci di smettere da subito, come ponte verso la cessazione completa e definitiva. C'è una evidenza limitata che la riduzione del fumo da sola possa portare ad un guadagno di salute. STRUTTURA ORGANIZZATIVA E FORMAZIONE L'evidenza e le raccomandazioni sopra menzionate riconoscono decisamente la cessazione del fumo come un intervento importante ed essenziale nella maggior parte dei pazienti con malattie respiratorie. I servizi per la cessazione del fumo dovrebbero essere parte integrante di un'unità operativa di pneumologia come le prove di funzionalità respiratoria e la broncoscopia, offrendo consigli ed aiuto a tutti i fumatori con malattie respiratorie indipendentemente dalla motivazione del fumatore, ma concentrandosi principalmente su quelli che vogliono cercare di smettere di fumare. I fumatori che non riescono in questo intento dovrebbero essere aiutati a ridurre il numero delle sigarette. Come minimo le unità operative di pneumologia dovrebbero offrire supporto nella cessazione del fumo con terapia sostitutiva nicotinica e/o bupropione SR ed almeno 4 visite di controllo a tutti i fumatori. I protocolli operativi di ciascun servizio dipendono da fattori locali e differenze nazionali tenendo in considerazione che l'intervento di ogni singolo clinico fallisce in più di un terzo dei fumatori [9]. La cessazione del fumo può essere effettuata individualmente o in gruppo, ma è necessario prevedere forza lavoro e tempo dedicato nell'ambito del piano di attività dell'unità operativa di pneumologia, insieme ad un budget per la farmacoterapia. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement Studi randomizzati controllati di riduzione assistita del fumo Sono stati pubblicati parecchi studi randomizzati controllati di riduzione del fumo. In sei studi (2 che hanno utilizzato inalatori di nicotina e quattro che hanno utilizzato gomme da masticare alla nicotina da sei mesi a un anno) che hanno arruolato in totale 2.424 fumatori che non desideravano o non erano in grado di smettere di colpo, è stata riportata una riduzione nel numero di sigarette fumate al giorno (> 50%) nel 15,9% dei fumatori che utilizzavano la NRT contro il 6,7% di quelli che utilizzavano il placebo [189]. Dopo un anno i tassi di cessazione del fumo erano dell'8,4% fra coloro che avevano utilizzato NRT contro il 4,1% di coloro che avevano utilizzato il placebo. Una riduzione nel numero di sigarette fumate al giorno di oltre il 50% dopo 3-4 mesi aveva un forte valore predittivo per la cessazione a un anno. La partecipazione a studi clinici di riduzione aumentava la motivazione a smettere. Sebbene il numero di sigarette fumate al giorno dopo 18 mesi fosse sceso al 36% del basale, nel gruppo trattato attivamente con nicotina il livello di monossido di carbonio era sceso solo al 71% rispetto al basale, suggerendo un certo grado di compensazione ottenuta attraverso un fumo più efficace di ciascuna sigaretta (inalazioni più profonde, più prolungate e più frequenti per ogni sigaretta) [189]. Un'analisi di 19 studi clinici di NRT sulla riduzione del fumo ha evidenziato una riduzione nel numero di sigarette fumate al giorno compresa fra il 25% (riduzione assoluta di 8 sigarette al giorno) e il 55% (23 sigarette al giorno) nel gruppo trattato con NRT comparato con una riduzione compresa tra il 13% (3 sigarette al giorno) e il 26% (8 sigarette al giorno) dei gruppi trattati con placebo [190,191]. Identificazione sistematica dei fumatori Prendendo in considerazione gli ospedali (sia per i ricoverati sia per i pazienti ambulatoriali) ci dovrebbe essere un piano organizzativo per identificare i fumatori, documentando i dati sul fumo nella registrazione ed inviando una breve comunicazione con un invito a rivolgersi al servizio per la cessazione del fumo [9,195]. Le linee guida della US Agency for Health Care Policy [9] suggeriscono che ogni servizio sanitario dovrebbe attuare un sistema per l'identificazione dei fumatori. La metanalisi di nove studi ha dimostrato che il tasso di intervento stimato dai clinici sui loro pazienti fumatori saliva dal 39 al 66% (95% CI: 58-73%) quando era stato messo in atto un sistema di screening per identificare lo stadio del fumo. Per quanto riguarda il tasso di cessazione l'impatto della presenza di un sistema identificativo rispetto all'assenza (n = 3 studi) ha MRM 37 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 38 riportato i tassi di cessazione stimati del 6,4% (1,3 - 11,6%)) versus 3,1% (non significativo), benché si debba considerare che queste statistiche sono basate su di un piccolo numero di studi [9]. Attrezzatura ed organico Certe necessità e competenze dovrebbero essere accessibili in ogni unità clinica per effettuare la valutazione di cui sopra. Dovrebbe essere possibile valutare il livello del CO, la dipendenza da nicotina e la motivazione della cessazione [80,196,197]. Uno o due componenti dello staff dovrebbero essere responsabili del programma per la cessazione del fumo, la formazione del personale e la gestione degli aspetti pratici. Se l'unità operativa non può offrire i servizi per la cessazione del fumo dovrebbero essere realizzate delle flow-chart in modo che i pazienti sappiano dove rivolgersi. È importante impegnare nella cessazione del fumo anche i MMG, come è importante che molti pazienti affetti da BPCO consultino con frequenza il loro MMG. Formazione È stato difficile dimostrare che le linee guida modificano la pratica clinica [198]. La durata della formazione oltre pochi giorni sembra inefficacie ed i molteplici strumenti di attuazione sono più efficaci di uno solo. È stato dimostrato che i seguenti strumenti alterano il comportamento dei medici di famiglia [199]: formazione da parte di medici “opinion leader”; feedback computerizzato simultaneo alle decisioni cliniche; istruzione dettagliata (cioè formazione personalizzata spesso da parte di un farmacista); incentivi al medico, ma anche istruzione o informazione ed incentivi per il paziente. Le linee guida dovrebbero essere semplici, pragmatiche, utilizzabili, flessibili e focalizzate all'attuazione [198,200]. La cessazione del fumo dovrebbe essere parte del curriculum essenziale dell'istruzione pre e post laurea e del tirocinio dei medici. Secondo l'esperienza degli autori di questo documento, le conoscenze sulla dipendenza e cessazione dal fumo di sigaretta variano tra gli operatori sanitari. Sembra che tra i medici ci sia la necessità di un aggiornamento su questo argomento, in particolare sulla farmacoterapia utilizzabile per la cessazione del fumo. Poiché il fumo gioca un ruolo eziologico così ampio per la maggioranza dei disturbi polmonari, la conoscenza della cessazione del fumo da parte degli pneumologi deve essere ad un livello simile a quello della loro conoscenza sulle altre terapie respiratorie, es. broncodilatatori e steroidi inalati. Corsi formativi regolari sono necessari per istruire gli operatori sanitari sulla cessazione del fumo ed inoltre i corsi devono essere ripetuti per prendere in considerazione l'avvicendamento del personale. Sarebbe l'optimum se tutti gli pneumologi partecipassero alla formazione indicata sopra. Ci dovrebbero anche essere corsi post laurea sulla cessazione del fumo al congresso annuale dell'ERS. L'abitudine personale al fumo e l'attitudine verso di esso da parte degli pneumologi e degli operatori sanitari non sembra interferire con la loro capacità 38 MRM a gestire la cessazione del fumo, ma il consiglio a smettere di fumare potrebbe essere considerato meno credibile dal paziente [201]. Strutture sanitarie libere dal fumo Fumare dovrebbe essere vietato negli ospedali, sia per i ricoverati sia per i pazienti ambulatoriali sia per il personale. In tutti gli ospedali degli USA da dieci anni è vietato fumare senza grossi problemi. L'Europa è molto indietro. Il valore più importante di una struttura sanitaria libera dal fumo è il segnale che essa da ai pazienti, ai parenti ed all'intera comunità. Per il singolo fumatore l'unità operativa di pneumologia può apparire più degna di fiducia se c'è il “vietato fumare”. Lavorando in un ambiente libero dal fumo si evitano anche gli effetti negativi sulla salute dovuti al fumo passivo. Quando un fumatore con patologie respiratorie è ricoverato in un reparto dove non si fuma, questa è un'ulteriore opportunità per intervenire indipendentemente dalla motivazione del paziente a smettere di fumare. Il reparto dovrebbe sostenere il fumatore informandolo e fornendogli sostegno comportamentale attraverso un operatore specializzato per la cessazione del fumo, oltre a prescrivere la terapia di sostituzione nicotinica o bupropione SR. La Rete Europea degli Ospedali Liberi da Fumo consta di 16 paesi membri. Questa organizzazione ha creato linee guida sia per l'attuazione di ospedali liberi da fumo sia per la formazione ed il materiale per gli operatori sanitari [202]. Inoltre, alcune unità operative pneumologiche potrebbero offrire alla comunità locale competenze per la formazione, l'istruzione, la ricerca, il patrocinio e pressioni politiche come pure sviluppare e sperimentare nuove terapie. COSTI DEL TABAGISMO ED ASPETTI ECONOMICI DEGLI INTERVENTI FINALIZZATI ALLA DISASSUEFAZIONE DAL FUMO DI SIGARETTA Costo delle patologie fumo-correlate Un recente studio statunitense, condotto sull'intera popolazione nazionale, ha valutato in US$6 miliardi la differenza annuale in spese sanitarie tra le persone affette e quelle non affette da patologie fumocorrelate [203]. Il costo, riferito a tutta la vita, delle patologie fumo-correlate per la popolazione olandese, a valori 1997, è stato stimato in US$ 7,27 miliardi ed in US$ 9,47 miliardi per i maschi e le femmine, rispettivamente [204]. Gli importi summenzionati non considerano i costi attribuibili alla perdita di giornate lavorative od alla premorienza causate dalle patologie fumo-correlate. In Germania i costi di pertinenza del settore sanitario relativi alle patologie fumo-correlate, espressi a valori 1996, raggiungevano € 5,471 miliardi per la BPCO (frazione attribuibile al fumo: 73%), € 2,593 miliardi per le neoplasie polmonari (89%), € 996 milioni per le neoplasie del cavo orale e della laringe (65%), € 1,774 miliardi per l'ictus cerebrale (28%), € 4,963 miliardi per le coronaropatie (35%) MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 39 Analisi costo-efficacia degli interventi di disassuefazione dal tabagismo Gli interventi finalizzati alla disassuefazione dal tabagismo sono notevolmente costo-efficaci quando confrontati con altri programmi sanitari. Secondo uno dei più noti esempi di league tables - elenchi di programmi sanitari classificati in ordine crescente in termini di costo per anno di vita salvato incrementale [210] o, più frequentemente, in termini di anno di vita salvato incrementale corretto per la qualità (Quality-Adjusted Life Year - QALY) [211-213] - smettere di fumare su consiglio del MMG era considerato un buon investimento di risorse (costo per QALY incrementale guadagnato a prezzi 1990: € 400), classificato al terzo posto in una lista di programmi sanitari medici e chirurgici destinati alla prevenzione od alla terapia di diverse patologie [213]. Tra i programmi sanitari rivolti ai pazienti affetti da BPCO, quando espresso a valori 1990-1991, il costo per anno di vita incrementale guadagnato seguendo una terapia di disassuefazione al tabagi- smo risultava pari ad US$ 6.500 [214], laddove l'importo in questione raggiungeva US$ 24.300 ed US$ 50.000 per un programma di riabilitazione polmonare e per una terapia del deficit di α1-antitripsina, rispettivamente [215]. A valori 1997, i programmi di disassuefazione dal tabagismo si qualificano come maggiormente costo-efficaci (US$ 2.700 per anno di vita salvato incrementale) di interventi sanitari destinati ad altre patologie, quali screening mammografico (US$ 50.000 per anno di vita salvato incrementale) e terapia dell'ipercolesterolemia grave (US$ 100.000 per anno di vita salvato incrementale) [216,217]. Secondo i risultati di una delle più rilevanti analisi costo-efficacia sui programmi sanitari rivolti alla disassuefazione dal tabagismo effettuata in Gran Bretagna, il costo per anno di vita salvato incrementale varia da € 354 (breve consiglio del MMG sull'importanza di smettere di fumare) ad € 1.458 (consiglio del MMG sull'importanza di smettere di fumare+auto-aiuto+consiglio di utilizzare una Terapia Sostitutiva della Nicotina (NRT) all'interno di un programma di disassuefazione dal tabagismo gestito da specialisti), a valori 1998. Questo è un intervento molto economico, anche considerando che queste cifre sono state calcolate quando gli ambulatori specialistici antifumo non erano operativi (quindi il secondo costo potrebbe essere leggermente più elevato). Tutte queste cifre sono comprensive di costi di pertinenza del settore sanitario e di costi non sanitari [206,207]. Un modello di analisi costo-efficacia realizzato in Gran Bretagna seguendo la prospettiva del NHS, ha confrontato diversi interventi di disassuefazione dal tabagismo; i risultati indicano che il costo per anno di vita salvato incrementale varia tra € 1.500-3.500 per NRT; € 935-2.200 per bupropione SR; € 1.300-2.900 per NRT + bupropione SR [218]. Nell'ambito di una serie di linee-guida sulla disassuefazione dal tabagismo destinate al MMG italiano, è stata effettuata un'analisi costo-efficacia finalizzata a confrontare 2 ipotetici programmi di cessazione del fumo gestiti dal MMG: cure primarie (consiglio del MMG di smettere di fumare) e ambulatorio antifumo (consiglio del MMG di smettere di fumare + NRT) [219]. I costi di pertinenza del settore sanitario, espressi a valori 2000, sono risultati pari ad € 87,18 e ad € 266,89 per cure primarie e ambulatorio antifumo, rispettivamente. Sulla base di pregresse evidenze cliniche [207], l'efficacia di cure primarie e ambulatorio antifumo era riportata pari a 7% e 17%, rispettivamente. Ipotizzando l'esistenza dell'opzione “non fare nulla”, il rapporto costo-efficacia incrementale (vale a dire, il costo addizionale per ottenere un ex-fumatore addizionale rispetto ad un'alternativa meno costosa e meno efficace) è risultato pari ad € 1.245,43 e ad € 1.797,10 per cure primarie e ambulatorio antifumo, rispettivamente. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement ed € 761 milioni per le arteropatie obliteranti (28%). Complessivamente, i costi di pertinenza del settore sanitario causati dal tabagismo si attestavano su € 16,6 miliardi per la Germania nel 1996 [205]. I costi annuali delle patologie fumo-correlate negli adulti, che gravano sul Servizio Sanitario Nazionale della Gran Bretagna (UK NHS), raggiungevano € 2,3 miliardi a valori 1998 [206,207]. Nel 2000, il valore economico delle giornate lavorative perse a causa delle patologie fumo-correlate era stimato in € 130 miliardi. Il tumore polmonare è responsabile del 5,7% di tutti i costi correlati al tabagismo sostenuti da UK NHS; il 90% di tale cifra concerne l'ospedalizzazione [207]. Per l'Italia, i costi di pertinenza del settore sanitario attribuibili al tabagismo sono stati calcolati quale contributo allo sviluppo di un modello epidemiologico internazionale, deterministico, di popolazione Economic Consequences of Smoking (ECOS), sviluppato nel 1999 sotto l'egida dell'Organizzazione Mondiale della Sanità (OMS) in occasione dell'iniziativa denominata Action Plan for a Tobacco-Free Europe [208]. Nel 1998, il totale dei costi di pertinenza del settore sanitario in Italia derivanti dalle malattie fumo-correlate è stato stimato in € 4,31271 miliardi (malattie cardiovascolari € 2,46419 miliardi; BPCO € 451,53 milioni; tumore polmonare a piccole cellule € 58,06 milioni; tumore polmonare non a piccole cellule € 232,25 milioni; ictus cerebrale € 1,10667 miliardi) [209]. In Gran Bretagna, i costi non sanitari annui relativi ai danni incendiari causati dall'abitudine al fumo sono stati stimati in circa € 6 milioni (Scozia) ed € 218 milioni (Inghilterra e Galles) [207]. Un recente sondaggio effettuato in Scozia ha dimostrato che l'assenteismo è maggiore tra i fumatori che tra i non fumatori [210], con perdite economiche annue stimate in € 60 milioni; complessivamente, la mancata attività lavorativa attribuibile al tabagismo, comporta costi pari a circa € 660 milioni per anno [207]. Cessazione del fumo e condizione socio-economica del paziente Data la compresenza di alcune condizioni sociali (vivere in un ambiente salubre; raggiungere un MRM 39 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 40 40 MRM buon livello di istruzione; maturare la consapevolezza che l'abitudine al fumo è nociva per la salute), rispetto alle persone economicamente meno agiate, le persone di condizione economica più elevata presentano una minore probabilità di sviluppare la dipendenza dalla sigaretta e registrano una maggiore aderenza agli interventi di disassuefazione dal tabagismo. I risultati di una vasta indagine sulle disuguaglianze in tema di salute condotta in Gran Bretagna [217,220], indicano che la più rilevante riduzione nella prevalenza di fumatori si registra tra le persone economicamente più agiate, mentre alle condizioni economicamente meno favorevoli si correlano risultati più modesti [221]. Cessazione del fumo ed “elasticità al prezzo” dei fumatori di sigarette L'elasticità al prezzo (la riduzione attesa nel consumo di sigarette conseguente ad un aumento del prezzo di queste ultime) è inversamente correlata all'età del fumatore. I risultati di una ricerca su questo tema, condotta negli Stati Uniti d'America, riportano la più ridotta elasticità al prezzo (-0,095) per i fumatori di età compresa tra 27 e 29 anni; la più elevata elasticità al prezzo (-0,831) si registra, invece, nei fumatori di età compresa tra 15 e 17 anni [222]. La teoria della dipendenza razionale [223-225] - la quale sostiene che, analogamente a quanto, in genere, accade ad un investimento finanziario, la dipendenza dalla sigaretta aumenta con il trascorrere del tempo - può spiegare questi risultati. Pertanto, maggiore è la durata dell'abitudine al fumo, minore è la probabilità che il fumatore decida di smettere a seguito di un aumento del prezzo delle sigarette. Ancora una volta, deve essere adeguatamente sottolineata l'importante funzione svolta dal prezzo delle sigarette nell'impedire che fumatori sperimentali (da adolescenti) possano diventare fumatori abituali (da adulti) [226,227]; infatti, alla luce dei risultati sopra citati [222], ad un aumento dell'1% nel prezzo delle sigarette corrisponde una riduzione del consumo delle medesime pari a 0,83% negli adolescenti. Un recente studio basato su dati raccolti in numerosi Paesi Europei ha dimostrato che la totalità delle terapie di prima linea per la disassuefazione dal tabagismo è notevolmente costo-efficace in confronto ad altri programmi di prevenzione [228). Punti chiave In considerazione delle ampie differenze in termini di “elasticità al prezzo” e della teoria della dipendenza razionale, imposte e prezzi elevati hanno un ruolo rilevante nella riduzione della futura dipendenza dalla sigaretta negli adolescenti; tale prescrizione risulta meno valida per i fumatori adulti. Gli interventi finalizzati alla disassuefazione dal tabagismo presentano un limitato costo per QALY (o per anno di vita) salvato incrementale. Arruolare in programmi anti-fumo dedicati (effettuati, per esempio, presso il luogo di lavoro) fumatori a basso reddito, con bassi livelli di istruzione e/o scolarizzazione e dediti a lavori manuali, aumenterà, nel breve perio- do, il costo per QALY incrementale di tali interventi ma potrebbe comportare, a lungo termine, una maggiore riduzione nella prevalenza di fumatori. Tra gli interventi finalizzati alla disassuefazione dal tabagismo attualmente disponibili, il consiglio del MMG o dello specialista, NRT e bupropione SR sembrano essere un buon investimento di risorse. In quanto costo-efficace, in Gran Bretagna, dall'Aprile 2001, la NRT può essere prescritta dal MMG. PROSPETTIVE DI RICERCA 1) Valutare l'efficacia della terapia sostitutiva della nicotina e del bupropione a rilascio sostenuto in monoterapia ed in associazione nei pazienti con patologie respiratorie, in particolare broncopneumopatia cronica ostruttiva ed asma. Sono altresì necessari studi sulla cessazione del fumo nei pazienti affetti da numerose altre patologie di pertinenza pneumologica, quali tubercolosi, deficit di α1-antitripsina, istiocitosi X e nei candidati al trapianto polmonare. 2) Valutare l'efficacia di differenti interventi di ripresa del trattamento, così come di trattamenti di lungo periodo finalizzati alla cessazione del fumo in pazienti con patologie respiratorie. 3) Valutare l'efficacia dell'assunzione di tabacco in forma diversa dal fumo quale strumento di disassuefazione nei fumatori resistenti alle terapie. 4) Valutare l'efficacia dello screening della funzionalità polmonare combinato con diverse strategie di disassuefazione dal tabagismo, in fumatori asintomatici e sintomatici. 5) Indagare le caratteristiche della dipendenza da tabacco/nicotina, degli ostacoli e della motivazione a smettere di fumare in pazienti affetti da malattie respiratorie. 6) Valutare se una riduzione nel consumo di sigarette nei pazienti non intenzionati ad abbandonare la sigaretta può aumentare la fiducia e la motivazione a smettere di fumare. 7) Indagare la relazione tra broncopneumopatia cronica ostruttiva e depressione e valutare se la terapia antidepressiva può aiutare il paziente pneumologico fumatore ad abbandonare la sigaretta. 8) Valutare l'efficacia di nuovi farmaci per la cessazione del fumo in pazienti affetti da malattie respiratorie. 9) Valutare l'efficacia dei programmi di disassuefazione dal tabagismo nei trattamenti di riabilitazione. 10) Valutare l'efficacia dei programmi di disassuefazione veicolati attraverso Internet, linee telefoniche di supporto ai fumatori intenzionati ad abbandonare la sigaretta ed altri metodi di cessazione del fumo supportati dai mezzi di comunicazione. RINGRAZIAMENTI Gli autori desiderano ringraziare F. Pistelli, Dipartimento Cardiotoracico, Azienda Ospedaliera Universitaria di Pisa e A. Scognamiglio, Unità di Epidemiologia Ambientale Polmonare, Istituto di Fisiologia Clinica, CNR, Pisa, per il loro contributo a numerosi paragrafi del presente manoscritto. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 41 1. Postma DS, Siafakas NM, eds. Management of Chronic Obstructive Pulmonary Disease. Eur Respir Mon 1998;7. 2. Global Initiative for Chronic Obstructive Lung disease. NHLBI/WHO Workshop. US Dept of Health and Human Services, National Institutes of Health, National Heart, Lung and Blood Institute. NIH Publication No. 2701A. Bethesda, National Institutes of Health, 2001. 3. Fletcher C, Peto R. The natural history of chronic airflow obstruction. BMJ 1977;1:1645-1648. 4. Fletcher C, Peto R, Tinker C, Speizer FE, eds. The natural history of chronic bronchitis and emphysema. Oxford, Oxford University Press, 1976. 5. Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, Conway WA Jr, Enright PL, Kanner RE, O'Hara P, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA 1994;272:1497-1505. 6. Hand S, Edwards S, Campbell IA, Cannings R. Controlled trial of three weeks nicotine replacement in hospital patients also given advice and support. Thorax 2002;57:715-718. 7. Borson S, Claypoole K, McDonald GJ. Depression and chronic obstructive pulmonary disease: treatment trials. Semin Clin Neuropsychiatry 1998;3:115-130. 8. Tashkin DP, Kanner R, Bailey W, Buist S, Anderson P, Nides M, Gonzales D, Dozier G, Patel MK, Jamerson B. Smoking cessation in patients with chronic obstructive pulmonary disease: a doubleblind, placebo-controlled, randomised trial. Lancet 2001;357:15711575. 9. Fiore MC, Bailey WC, Cohen SJ, Dorfman, SF; Goldstein, HG; Gritz, ER, et al. Smoking cessation: clinical practice guidelines No. 18. Public Health Service, Agency for Health Care Policy and Research. AHCPR Publication No. 96-0692. Rockville, US Dept of Health and Human Services, 1996. 10. Fiore M, Bailey W, Cohen S, Dorfman, SF; Goldstein, HG; Gritz, ER, et al. Treating tobacco use and dependence: clinical practice guideline. Rockville, US Dept of Health and Human Services, 2000. 11. The Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff and Consortium Representatives. A clinical practice guideline for treating tobacco use and dependence: a US Public Health Service report. JAMA 2000;283:3244-3254. 12. Anderson JE, Jorenby DE, Scott WJ, Fiore MC. Treating tobacco use and dependence: an evidence-based clinical practice guideline for tobacco cessation. Chest 2002;121:932-941. 13. American College of Chest Physicians, American Thoracic Society, European Respiratory Society, Asian Pacific Society of Respirology, Canadian Thoracic Society, International Union Against Tuberculosis and Lung Disease. Smoking and health: the physician's responsibility. A statement by the Health and Smoking Committee. Pneumologie 1996;50:270-274. 14. Hughes JR, Fiester S, Goldstein MG, Resnick MP, Rock N, Ziedonis D. The American Psychiatric Association Practice Guidelines for the treatment of patients with nicotine dependence. Am J Psychiatry 1996;153(Suppl.10):S1-S31. 15. Haustein KO. Tobacco or Health? Berlin, Springer-Verlag, 2001;3443. 16. Batra V, Patkar AA, Berrettini WH, Weinstein SP, Leone FT. The genetic determinants of smoking. Chest 2003;123:1730-1739. 17. Watkins SS, Koob GF, Markou A. Neural mechanisms underlying nicotine addiction: acute positive reinforcement and withdrawal. Nicotine Tob Res 2000;2:19-37. 18. US Department of Health and Human Services. Nicotine addiction. A report of the Surgeon General. Rockville, US Dept of Health and Human Services, 1998. 19. World Health Organization. International Classification of Diseases, 10th Edn. Geneva, World Health Organization, 1992. 20. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th Edn. Washington, American Psychiatric Association, 1994. 21. Hughes JR, Gust SW, Skoog K, Keenan RM, Fenwick JW. Symptoms of tobacco withdrawal. A replication and extension. Arch Gen Psychiatry 1991;48:52-59. 22. Shiffman S, West RJ, Gilbert DG. SRNT Work Group on the Assessment of Craving and Withdrawal in Clinical trials. Nicotine Tob Res 2004;6:599-614. 23. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, The World Bank, 1999. Available at www1.worldbank.org/ tobacco/reports.asp. Date last accessed: March 15, 2005. Date last updated: 2001. 24. Tobacco Policy in the European Union: ASH Fact Sheet No. 20. www.ash.org.uk/html/factsheets/html/fact20. html. Date last accessed: November 28, 2005. Date last updated: May 2006. 25. Doxa. Indagine sul fumo in Italia 2004. www.doxa.it/ italiano/inchieste/fumo2004_ita.pdf. Date last accessed: March 15, 2005. Date last updated: April 2004. 26. Murin S, Bilello KS, Matthay R. Other smoking-affected pulmonary diseases. Clin Chest Med 2000;21:121-137. 27. US Department of Health and Human Services. The health consequences of smoking: a report of the Surgeon General, 2004. www.cdc.gov/tobacco/sgr/sgr_2004/ index.htm. Date last accessed: November 28, 2006. Date last updated: February 15, 2006. 28. Peto R, Lopez AD, Boreham J, Thun M, Heath C Jr., Doll R. Mortality from smoking worldwide. Br Med Bull 1996;52:12-21. 29. Ezzati M, Lopez AD. Estimates of global mortality attributable to smoking in 2000. Lancet 2003;362:847-852. 30. Rodu B, Cole P. The burden of mortality from smoking: comparing Sweden with other countries in the European Union. Eur J Epidemiol 2004;19:129-131. 31. Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years' observations on male British doctors. BMJ 2004;328:1529-1533. 32. Lung cancer. In: European Respiratory Society/European Lung Foundation. European Lung White Book. The First Comprehensive Survey on Respiratory Health in Europe. Sheffield, ERS Journals, 2003;44-54. 33. La Vecchia C, Franceschi S, Levi F. Epidemiological research on cancer with a focus on Europe. Eur J Cancer Prev 2003;12:5-14. 34. Alberg AJ, Samet JM. Epidemiology of lung cancer. Chest 2003;123(Suppl.1):21S-49S. 35. Flanders WD, Lally CA, Zhu BP, Henley SJ, Thun MJ. Lung cancer mortality in relation to age, duration of smoking, and daily cigarette consumption: results from Cancer Prevention Study II. Cancer Res 2003;63:6556-6562. 36. Simonato L, Agudo A, Ahrens W, Benhamou E, Benhamou S, Boffetta P, Brennan P, Darby SC, Forastiere F, Fortes C, Gaborieau V, Gerken M, Gonzales CA, Jöckel KH, Kreuzer M, Merletti F, Nyberg F, Pershagen G, Pohlabeln H, Rösch F, Whitley E, Wichmann HE, Zambon P. Lung cancer and cigarette smoking in Europe: an update of risk estimates and an assessment of inter-country heterogeneity. Int J Cancer 2001;91:876-887. 37. Murray CJL, Lopez AD. Alternative projections of mortality and disability by cause 1990- 2020: Global Burden of Disease Study. Lancet 1997;349:1498-1504. 38. Chronic obstructive pulmonary disease. In: European Respiratory Society/European Lung Foundation. European Lung White Book. The First Comprehensive Survey on Respiratory Health in Europe. Sheffield, ERS Journals, 2003;34-43. 39. Burney P, Suissa S, Soriano JB, Vollmer WM, Viegi G, Sullivan SD, Fabbri LM, Sin DD, Ernst P, Coultas D, Bourbeau J, Mapel DW, Weiss K, McLaughlin T, Price D, Sturkenboom MC, Taylor R, Hagan GW. The pharmacoepidemiology of COPD: recent advances and methodological discussion. Eur Respir J 2003; 22(Suppl.42):1s-44s. 40. Wedzicha JA, Donaldson GC. Exacerbations of chronic obstructive pulmonary disease. Respir Care 2003;48:1204-1213. 41. Viegi G, Pedreschi M, Baldacci S, Chiaffi L, Pistelli F, Modena P, Vellutini M, Di Pede F, Carrozzi L. Prevalence rates of respiratory symptoms and diseases in general population samples of North and Central Italy. Int J Tuberc Lung Dis 1999;3:1034-1042. 42. Lundbäck B, Lindberg A, Lindström M, Rönmark E, Jonsson AC, Jönsson E, Larsson LG, Andersson S, Sandström T, Larsson K; Obstructive Lung Disease in Northern Sweden Studies. Not 15 but 50% of smokers develop COPD? Report from the Obstructive Lung Disease in Northern Sweden Studies. Respir Med 2003;97:115-122. 43. de Marco R, Accordini S, Cerveri I, Corsico A, Sunyer J, Neukirch F, Künzli N, Leynaert B, Janson C, Gislason T, Vermeire P, Svanes C, Anto JM, Burney P; European Community Respiratory Health Survey Study Group. An international survey of chronic obstructive pulmonary disease in young adults according to GOLD stages. Thorax 2004;59:120-125. 44. Jimenez-Ruiz CA, Masa F, Miravittles M, Gabriel R, Viejo JL, Villasante C, Sobradillo V. Smoking characteristics: differences in attitudes and dependence between healthy smokers and smokers with COPD. Chest 2001;119:1365-1370. 45. Watson L., Boezen HM, Postma DS. Differences between males and females in the natural history of asthma and COPD. In: Buist S, Mapp CE, eds. Respiratory Diseases in Women. Eur Respir Mon 2003;25:50-73. 46. Viegi G, Scognamiglio A, Baldacci S, Pistelli F, Carrozzi L. Epidemiology of chronic obstructive pulmonary disease (COPD). Respiration 2001;68:4-19. 47. Calverley PMA, Walker P. Chronic obstructive pulmonary disease. Lancet 2003;362:1053-1061. 48. Willemse BWM, Postma DS, Timens W, ten Hacken NHT. The impact of smoking cessation on respiratory symptoms, lung function, airway hyperresponsiveness and inflammation. Eur Respir J 2004;23:464-476. 49. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement Bibliografia MRM 41 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 42 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 42 MRM Connett JE, for the Lung Health Study Research Group. The effects of a smoking cessation intervention on 14.5-year mortality. Ann Intern Med 2005;142:233-239. Cerveri I, Accordini S, Corsico A, Zoia MC, Carrozzi L, Cazzoletti L, Beccaria M, Marinoni A, Viegi G, de Marco R; ISAYA Study Group. Chronic cough and phlegm in young adults. Eur Respir J 2003;22:413-417. Carrozzi L, Rijcken B, Burney P, et al. Family history for chronic lung diseases and epidemiological determinants of COPD in three European countries. Eur Respir Rev 2001;11:49-54. Eagan TML, Gulsvik A, Eide GE, Bakke PS. Remission of respiratory symptoms by smoking and occupational exposure in a cohort study. Eur Respir J 2004;23:589-594. Kerstjens HAM, Rijcken B, Schouten JP, Postma DS. Decline of FEV1 by age and smoking status: facts, figures, and fallacies. Thorax 1997;52:820-827. Gold DR, Wang X, Wypij D, Speizer FE, Ware JH, Dockery DW. Effects of cigarette smoking on lung function in adolescent boys and girls. N Engl J Med 1996;335:931-937. Sherrill DL, Lebowitz MD, Knudson RJ, Burrows B. Smoking and symptom effects on the curves of lung function growth and decline. Am Rev Respir Dis 1991;144:17-22. Xu X, Weiss ST, Rijcken B, Schouten JP. Smoking, changes in smoking habits, and rate of decline in FEV1: new insight into gender differences. Eur Respir J 1994;7:1056-1061. Downs SH, Brandli O, Zellweger JP, Schindler C, Künzli N, Gerbase MW, Burdet L, Bettschart R, Zemp E, Frey M, Keller R, Tschopp JM, Leuenberger P, Ackermann-Liebrich U; SAPALDIA team. Accelerated decline in lung function in smoking women with airway obstruction: SAPALDIA 2 cohort study. Respir Res 2005;6:45. Anthonisen NR, Connett JE, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med 2002;166:675-679. Scanlon PD, Connett JE, Waller LA, Altose MD, Bailey WC, Buist AS. Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease. The Lung Health Study. Am J Respir Crit Care Med 2000;161:381-390. Sherrill DL, Enright P, Cline M, Burrows B, Lebowitz MD. Rates of decline in lung function among subjects who restart cigarette smoking. Chest 1996;109:1001-1005. Murray RP, Anthonisen NR, Connett JE, Wise RA, Lindgren PG, Greene PG, Nides MA. Effects of multiple attempts to quit smoking and relapses to smoking on pulmonary function. Lung Health Study Research Group. J Clin Epidemiol 1998;51:1317-1326. Bolliger CT, Zellweger JP, Danielsson T, van Biljon X, Robidou A, Westin A, Perruchoud AP, Säwe U. Influence of long-term smoking reduction on health risk markers and quality of life. Nicotine Tob Res 2002;4:433-439. Viegi G, Paoletti P, Carrozzi L, Baldacci S, Modena P, Pedreschi M, Di Pede F, Mammini U, Giuntini C. CO diffusing capacity in a general population sample: relationships with cigarette smoking and airflow obstruction. Respiration 1993;60:155-161. Viegi G, Sherrill DL, Carrozzi L, Di Pede F, Baldacci S, Pistelli F, Enright P. An 8-year follow up of carbon monoxide diffusing capacity in a general population sample of northern Italy. Chest 2001;120:74-80. Viegi G, Matteelli G, Annesi I. Epidemiology of asthma. In: Chung F, Fabbri LM, eds. Asthma. Eur Respir Mon 2003;23:1-25. Ulrik CS, Lange P. Cigarette smoking and asthma. Monaldi Arch Chest Dis 2001;56:349-353. Thomson NC, Chaudhuri R, Livingston E. Asthma and cigarette smoking. Eur Respir J 2004;24:822-833. Doll R. Risk from tobacco and potentials for health gain. Int J Tuberc Lung Dis 1999;3:90-99. Tønnesen P, Pisinger C, Hvidberg S, Wennike P, Bremann L, Westin A, Thomsen C, Nilsson F. Effects of smoking cessation and reduction in asthmatics. Nicotine Tob Res 2005;7:139-148. Farr BM, Bartlett CL, Wadsworth J, Miller DL. Risk factors for community-acquired pneumonia diagnosed upon hospital admission. British Thoracic Society Pneumonia Study Group. Respir Med 2000;94:954-963. Almirall J, Gonzalez CA, Balanzo X, Bolibar I. Proportion of community-acquired pneumonia cases attributable to tobacco smoking. Chest 1999;116:375-379. Nuorti JP, Butler JC, Farley MM, Harrison LH, McGeer A, Kolczak MS, Breiman RF. Cigarette smoking and invasive pneumococcal disease. Active Bacterial Core Surveillance Team. N Engl J Med 2000;342:681-689. Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med 2004;164:2206-2216. Gajalakshmi V, Peto R, Kanaka TS, Jha P. Smoking and mortality from tuberculosis and other diseases in India: retrospective study of 43 000 adult male deaths and 35000 controls. Lancet 2003;362:507515. Baumgartner KB, Samet JM, Stidley CA, Colby TV, Waldron JA, 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. 96. 97. 98. 99. 100. 101. Collaborating Centers. Cigarette smoking: a risk factor for idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1997;155:242248. Chiyo M, Sekine Y, Iwata T, Tatsumi K, Yasufuku K, Iyoda A, Otsuji M, Yoshida S, Shibuya K, Iizasa T, Saitoh Y, Fujisawa T. Impact of interstitial lung disease on surgical morbidity and mortality for lung cancer: analyses of short-term and long-term outcomes. J Thorac Cardiovasc Surg 2003;126:1141-1146. Henry M, Arnold T, Harvey J, on behalf of the BTS Pleural Disease Group, a subgroup of the BTS Standards of Care Committee. BTS guidelines for the management of spontaneous pneumothorax. Thorax 2003;58(Suppl.II):39-52. Rollnick S, Mason P, Butler C. Health behaviour change: a guide for practitioners. London, Churchill Livingstone, 1999. Fagerström KO. Time to first cigarette; the best single indicator of tobacco dependence. Monaldi Arch Chest Dis 2003;59:95-98. Etter JF, Duc TV, Perneger TV. Saliva cotinine levels in smokers and non-smokers. Am J Epidem 2000;151:251-258. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerstöm Tolerance Questionnaire. British Journal of Addiction 1991;86:1119-1127. Fagerström KO, Schneider N. Measuring nicotine dependence: A review of the Fagerström Tolerance Questionnaire. J Behav Med 1989;12:159-182. Breslau N, Johnson EO. Predicting smoking cessation and major depression in nicotine dependent smokers. Am J Pub Health 1999;90:1122-1127. Batra A, Gelfort G, Bartels M. The dopamine D2 receptor (DRD2) gene - a genetic risk factor in heavy smoking? Addict Biol 2000;5:431-438. Etter JF, LeHouezec J, Perneger TV. A self-administered questionnaire to measure addiction to cigarettes. The Cigarette Dependence Scale. Neuropsychopharmacology 2003;28:359-370. Javors MA, Hatch JP, Lamb R. Cut-off levels for breath carbon monoxide as a marker for cigarette smoking. Addiction 2005;100:159-167. Jimenez-Ruiz CA, Masa F, Miravitlles M, Gabriel R, Viejo JL, Villasante C, Sobradillo V. Smoking characteristics: differences in attitudes and dependence between healthy smokers and smokers with COPD. Chest 2001;119:1365-1370. Petty TL, Doherty DE. National Lung Health Education Program. The National Lung Health Education Program: roots, mission, future directions. Respir Care 2004;49:678-683. Enright PL, Kaminsky DA. Strategies for screening for chronic obstructive pulmonary disease. Respir Care 2003;48:1194-1201. Clotet J, Gomez-Arbones X, Ciria C, Aldalad JM. Spirometry is a good method for detecting and monitoring chronic obstructive pulmonary disease in high-risk smokers in primary care. Arch Bronconeumol 2004;40:155-159. Stratelis G, Jakobsson P, Molstad S, Zetterstrom O. Early detection of COPD in primary care: screening by invitation of smokers aged 40 to 55 years. Brit J Gen Pract 2004;54:201-206. Gorecka D, Bednarek M, Nowinski A, Puscinska E, Goljan-Geremek A, Zielinski J. Diagnosis of airflow limitation combined with smoking cessation advice increases stopsmoking rate. Chest 2003;123:1916-1923. Bize R, Burnand B, Mueller Y, Cornuz J. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev 2005;4:CD0004705. Hughes JR. Comorbidity and smoking. Nicotine Tob Res 1999; 1(Suppl.2):S149-S152. Dierker LC, Avenevoli S, Stolar M, Merikangas KR. Smoking and depression: an examination of mechanisms of comorbidity. Am J Psychiatry 2002;159:947-953. Glassman AH, Covey LS, Stetner F, Rivelli S. Smoking cessation and the source of major depression: a follow up study. Lancet 2001;357:1929-1932. Wagena E, Kant I, Huibers MJ, van Amelsvoort LG, Swaen GM, Wouters EF, van Schayck CP. Psychological distress and depressed mood in employees with asthma, chronic bronchitis or emphysema: a population-based observational study on prevalence and the relationship with smoking cigarettes. Eur J Epidemiol 2004;19:147-153. Arrol B, Khin N, Kerse N. Screening for depression in primary care with two verbally asked questions: cross sectional study. BMJ 2003;327:1144-1146. Watkins C, Daniels L, Jack C, Dickinson H, van der Broek M. Accuracy of a single question in screening for depression in a cohort of patients after stroke: comparative study. BMJ 2001;323:1159. Centers for Disease Control and Prevention. Smoking cessation during previous years among adults in United States 1990 and 1991. MMWR 1993;42:504-507. US Dept of Health and Human Services. The health consequences of smoking: Chronic obstructive lung disease. A report of the Surgeon General. Rockville, US Dept of Health and Human MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 43 129. Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev 2005;2:CD001007. 130. Lichtenstein E, Glasgow RE, Lando HA, Ossip-Klein DJ, Boles SM. Telephone counseling for smoking cessation: rationales and metaanalytic review of evidence. Health Educ Res 1996;11:243-257. 131. Stead LF, Lancaster T, Perera R. Telephone counselling for smoking cessation. Cochrane Database Syst Rev 2006;3:CD002850. 132. Borland R, Segan CJ, Livingston PM, Owen N. The effectiveness of callback counselling for smoking cessation: a randomised trial. Addiction 2001;96:881-889. 133. Macleod ZR, Charles MA, Arnaldi VC, Adams IM. Telephone counselling as an adjunct to nicotine patches in smoking cessation: a randomised controlled trial. Med J Aust 2003;179:349-352. 134. Hajek P, Stead LF. Aversive smoking for smoking cessation. Cochrane Database Syst Rev 2001;3:CD000546. 135. Ussher M, Nunciata P, Cropley M, West R. Effect of a short bout of exercise on tobacco withdrawal symptoms and desire to smoke. Psychopharmacology (Berl) 2001;158:66-72. 136. Bock BC, Marcus BH, King TK, Borrelli B, Roberts MR. Exercise effects on withdrawal and mood among women attempting smoking cessation. Addict Behav 1999;24:399-410. 137. Steptoe A, Edwards S, Moses J, Mathews A. The effects of exercise training on mood and perceived coping ability in anxious adults from the general population. J Psychosom Res 1989;33:537-547. 138. McAuley E, Mihalko SL, Bane SM. Exercise and self esteem in middle-aged adults: multidimensional relationships and physical fitness and self-efficacy influences. J Behav Med 1997;20:67-83. 139. Ussher M. Exercise interventions for smoking cessation. Cochrane Database Syst Rev 2005;1:CD002295. 140. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2004;3:CD000146. 141. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev 2004;4:CD000031. 142. Crowley TJ, Macdonald MJ, Walter MI. Behavioural antismoking trial in chronic obstructive pulmonary disease patients. Psychopharmacology 1995;119:193-204. 143. Pederson LL, Wanklin JM, Lefcoe NM. The effect of counselling on smoking cessation among patients hospitalised with chronic obstructive pulmonary disease: a randomised clinical trial. Int J Addiction 1991;26:107-119. 144. Wagena EJ, van der Meer RM, Ostelo RJ, Jacobs JE, van Schayck CP. The efficacy of smoking cessation strategies in people with chronic obstructive pulmonary disease: results from a systematic review. Respir Med 2004;98:805-815. 145. Research Committee of the British Thoracic Society. Smoking cessation in patients: two further studies by the British Thoracic Society. Thorax 1990;45:835-840. 146. Tønnesen P, Mikkelsen KL. Routine smoking cessation with four nicotine regiments in a lung clinic. Eur Respir J 2000;16:717-722. 147. West R, McNeill A, Raw M. Smoking cessation guidelines for health professionals: an update. Thorax 2000;55:987-999. 148. World Health Organisation. European partnership to reduce tobacco dependence: WHO evidence based recommendations on the treatment of tobacco dependence. Geneva, WHO, 2001. 149. National Institute for Health and Clinical Excellence. Smoking cessation - bupropion and nicotine replacement therapy. National Institute for Health and Clinical Excellence Technology appraisal TA39. www.nice. org.uk/page.aspx?o5TA39. Date last accessed: May 2006. Date last updated: March 2002. 150. Andersson JE, Jorenby DE, Scott WJ, Fiore MC. Treating tobacco use and dependence. Chest 2002;121:932-941. 151. Wagena E, Zeegers M, Van Schayck C, Wouters E. Benefits and risks of pharmacological smoking cessation therapies in chronic obstructive pulmonary disease. Drug Saf 2003;26:381-403. 152. Anthonisen NR, Connett JE, Kiley JP, ltose MD, Bailey WC, Buist AS, Conway WA Jr, Enright PL, Kanner RE, O'Hara P, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1: The Lung Health Study. JAMA 1994;272:1497-1505. 153. Sachs DPL, Benowitz NL, Silver KJ. Effective use of nicotine polacrilex (Nicorette) in patients with chronic obstructive pulmonary disease. In: Aoki M, Hisamichi S, Tominaga S, eds. Smoking and health. Amsterdam, Elsevier, 1987;793-795. 154. Glover ED, Glover PN, Abrons HL, et al. Smoking cessation among COPD and chronic bronchitis patients using the nicotine nasal spray. Am J Health Behav 1997;21:310-317. 155. Tønnesen P. Smoking cessation. In: Pauwels RA, Postma DS, Weiss ST, eds. Long-term intervention in chronic obstructive pulmonary disease. Lung Biology in Health and Disease, New York, Marcel Dekker, 2005;191:315-352. 156. Campbell IA, Prescott RJ, Tjeder-Burton SM. Smoking cessation in hospital patients given repeated advice plus nicotine or placebo chewing gum. Respir Med 1991;85:155-157. 157. Campbell IA, Prescott RJ, Tjeder-Burton SM. Transdermal nicotine L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement Services, 1984. 102. van Manen JG, Bindels PJ, Dekker FW. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax 2002;57:412-416. 103. Wagena EJ, Kant I, van Amelsvoort LG, Wouters EF, van Schaychk CP, Swaen GM. Risk of depression and anxiety in employees with chronic bronchitis: the modifying effect of cigarette smoking. Psychosom Med 2004;5:729-734. 104. Breslau N, Peterson EL, Schultz LR. Major depression and stages of smoking. A longitudinal investigation. Arch Gen Psychiatry 1998;55:161-166. 105. Covey LS, Glassaman AH, Stetner F. Cigarette smoking and major depression. J Addict Dis 1998;17:35-46. 106. West R, Hajek P, Belcher M. Severity of withdrawal symptoms as a predictor of outcome of an attempt to quit smoking. Psychol Med 1989;19:981-985. 107. Shiffman S, Hickcox M, Paty J, Gnys M, Kassel J, Richards T. Progression from a smoking lapse to relapse: prediction from abstinence violation effects, nicotine dependence, and lapse characteristics. J Consult Clin Psychol 1996;64:993-1002. 108. Kim HF, Kunik ME, Molinari VA. Functional impairment in COPD patients: the impact of anxiety and depression. Psychosomatics 2000;41:465-471. 109. de Voogd JN, Elzen HA. Psychological state and personality traits of patients in a pulmonary rehabilitation program. Eur Respir J 2001;18(Suppl.33):54s. 110. Dudley DL, Wermuth C, Hague W. Psychological aspects of care in the chronic obstructive pulmonary disease patient. Heart Lung 1973;2:339-345. 111. Gorecka D, Bednarek M, Nowinski A, Plywaczewski R, Zielinski J, Bielen P. Nicotine dependence in smokers at risk for COPD. Eur Respir J 2002;20(Suppl.38):134s. 112. Miloskovic V, Lazic Z. Lung function and level of the smoker's nicotine dependence. Eur Respir J 2001;18(Suppl.33):S115-S116. 113. Kunze U, Schoberberger R, Schmeiser-Rieder A, Fagerström K. Preventive oncology and nicotine addiction. In: Antypas G, ed. International Proceedings Division, 2nd International Congress on Lung Cancer. Bologna, Monduzzi Editore, 1996;551-554. 114. Mikami I, Akechi T, Kugaya A, Okuyama T, Nakano T, Okamura H, Yamawaki S, Uchitomi Y. Screening for nicotine dependence among smoking related cancer patients. Japan J Cancer Res 1999;90:10711075. 115. Jiménez-Ruiz CA, Miravitlles M, Sobradillo V, Gabriel R, Viejo JL, Masa JF, Fernández-Fau L, Villasante C. Can cumulative tobacco consumption, FTND score, and carbon monoxide concentrations in expired air be predictors of chronic obstructive pulmonary disease? Nicotine Tob Res 2004;6:649-653. 116. Medici TC, Unger S, Ruegger M. Smoking pattern of smokers with and without tobaccorelated lung diseases. Am Rev Resp Dis 1985;131:385-388. 117. Pauwels RA, Buist AS, Calverley PM. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med 2001;163:1256-1276. 118. Siafakas NM, Vermeire P, Pride NB, Paoletti P, Gibson J, Howard P, Yernault JC, Decramer M, Higenbottam T, Postma DS, et al. Optimal assessment and management of COPD. The European Respiratory Society Task Force. Eur Respir J 1995; 8:1398-1420. 119. Gray-Donald K, Gibbons L, Shapiro SH, Macklem PT, Martin JG. Nutritional status and mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1996;153:961-966. 120. Filozof C, Fernadez Pinilla MC, Fernadez-Cruz A. Smoking cessation and weight gain. Obes Rev 2004;5:95-103. 121. Lancaster T, Stead LF. Self-help interventions for smoking cessation. Cochrane Database Syst Rev 2005;3:CD001118. 122. Borland R, Balmford J, Hunt D. The effectiveness of personally tailored computer generated advice letters for smoking cessation. Addiction 2004;99:369-377. 123. Quist-Paulsen P, Gallefos F. Randomised controlled trial of smoking cessation intervention after admission for coronary heart disease. BMJ 2003;327:1254-1257. 124. Aveyard P, Griffin C, Lawrence T, Cheng KK. A controlled trial of an expert system and self help manual intervention based on the stages of change versus standard self-help materials in smoking cessation. Addiction 2003;98:345-354. 125. Lancaster T, Stead L. Physician advice for smoking cessation. Cochrane Database Syst Rev 2004;4:CD000165. 126. Rice V, Stead LF. Nursing interventions for smoking cessation. Cochrane Database Syst Rev 2004;1:CD001188. 127. British Thoracic Society. Comparison of four methods for smoking cessation in patients with smoking related disorders. BMJ 1983;286:595-597. 128. Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst Rev 2005;2:CD001292. MRM 43 Multidisciplinary Respiratory Medicine 2009; 4(1): 15-45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 44 158. 159. 160. 161. 162. 163. 164. 165. 166. 167. 168. 169. 170. 171. 172. 173. 174. 175. 176. 177. 178. 179. 44 MRM plus support in patients attending hospital with smoking-related diseases: a placebo-controlled study. Respir Med 1996;90:47-51. Miller NH, Smith PM, DeBusk RF, Sobel DS, Taylor CB. Smoking cessation in hospitalized patients: results of a randomized trial. Arch Intern Med 1997;157:409-415. Lewis SF, Piasecki TM, Anderson JE, Baker TB. Transdermal nicotine replacement for hospitalized patients: a randomized clinical trial. Prev Med 1998;27:296-303. Tønnesen P, Mikkelsen KL, Markholst C, Ibsen A, Bendixen M, Pedersen L, Fuursted R, Hansen LH, Stensgaard H, Schiøtz R, Petersen T, Breman L, Clementsen P, Evald T. Nurse-conducted smoking cessation with minimal intervention in a lung clinic: a randomized controlled study. Eur Respir J 1996;9:2351-2355. Tønnesen P, Mikkelsen K, Bremann L. Nurse-conducted smoking cessation in patients with COPD, using nicotine sublingual tablets and behavioral support. Chest 2006;130:314-316. Gratziou C, Francis K, Maragianni A, et al. Bupropion treatment and cognitive behavioral therapy in smoking cessation program. Eur Respir J 2001;18(Suppl.33):12s. Richmond R, Zwar N. Review of bupropion for smoking cessation. Drug and Alcohol Review 2003;22:203-220. Tønnesen P, Fryd V, Hansen M, Helsted J, Gunnersen AB, Forchammer H, Stockner M. Two and four mg nicotine chewing gum and group counseling in smoking cessation: an open, randomized, controlled trial with a 22 month follow-up. Addict Behav 1988;13:17-27. Tønnessen P, Paoletti P, Gustavsson G, Russell MA, Saracci R, Gulsvik A, Rijcken B, Sawe U. Higher dosage nicotine patches increase one-year smoking cessation rates: results from the European CEASE-trial. Collaborative European Anti-Smoking Evaluation. European Respiratory Society. Eur Respir J 1999;13:238246. Shiffman S, Dressler C, Hajek P, Gilburt S, Targett D, Strahs K. Efficacy of a nicotine lozenge for smoking cessation. Arch Intern Med 2002;162:1267-1276. Ferry LH, Burchette RJ. Efficacy of bupropion for smoking cessation in non-depressed smokers. J Addict Disord 1994;13:249. Dalsgareth O, Hansen N, Soes-Petersen U, Evald T, Høegholm A, Barber J, Vestbo J. A multicentre, randomised, double blind, placebo controlled, 6-month trial of bupropion hydrochloride sustained release tablets as an aid to smoking cessation in hospital employees. Nicotine Tob Res 2004;6:55-61. Garcia-Rio F, Serrano S, Mediano O, Alonso A, Vilamor J. Safety profile of bupropion for COPD. Lancet 2001;358:1009-1010. Tonstad S, Farsang D, Klaene G, Lewis K, Manolis A, Perruchoud AP, Silagy C, van Spiegel PI, Astbury C, Hider A, Sweet R. Bupropion SR for smoking cessation in smokers with cardiovascular disease: a multicentre, randomised study. Eur Heart J 2003;24:946-955. Hays JT, Hurt RD, Rigotti NA, Niaura R, Gonzales D, Durcan MJ, Sachs DP, Wolter TD, Buist AS, Johnston JA, White JD. Sustainedrelease bupropion for pharmacologic relapse prevention after smoking cessation: a randomized, controlled trial. Ann Intern Med 2001;135:423-433. Sampablo I, Lores L, Coll-Klein F, Jimenez C, Rebasa P. Predictive factors in smoking cessation with combined therapy with bupropion and nicotine patches. Monaldi Arch Chest Dis 2003;59:171-176. Jorenby DE, Leischow SJ, Nides MA, Rennard SI, Johnston JA, Hughes AR, Smith SS, Muramoto ML, Daughton DM, Doan K, Fiore MC, Baker TB. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med 1999;340:685-691. Glassman AH, Covey LS, Dalack GW, Stetner F, Rivelli SK, Fleiss J, Cooper TB. Smoking cessation, clonidine, and vulnerability to nicotine among dependent smokers. Clin Pharmacol Ther 1993;54:670679. Hilleman DE, Mohiuddin SM, Delcore MG, Lucas BD Jr. Randomized controlled trial of transdermal clonidine for smoking cessation. Ann Pharmacother 1993;27:1025-1028. Gonzales D, Rennard SI, Nides M, Oncken C, Azoulay S, Billing CB, Watsky EJ, Gong J, Williams KE, Reeves KR; Varenicline Phase 3 Study Group. Varenicline, an a4b2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation. JAMA 2006;296:47-55. Jorenby DE, Hays T, Rigotti NA, Azoulay S, Watsky EJ, Williams KE, Billing CB, Gong J, Reeves KR; Varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA 2006;296:56-63. Tonstad S, Tønnesen P, Hajek P, Williams KE, Billing CB, Reeves KR; Varenicline Phase 3 Study Group. Effect of maintenance therapy with varenicline on smoking cessation. JAMA 2006;296:64-71. Cohen C, Kodas E, Griebel G. CB1 receptor antagonists for the treatment of nicotine addiction. Pharmacol Biochem Behav 2005;81:387-395. 180. Anthenelli RM, Despres JP. Effects of rimonabant in the reduction of major cardiovascular risk factors. Results from the STRATUS-US Trial (smoking cessation in smokers motivated to quit). American College of Cardiology 53rd Annual Scientific Session. New Orleans, American College of Cardiology, 2004. 181. Van Gaal LF, Rissanen AM, Scheen AJ, Ziegler O, Rossner S. Effects of the cannabinoid-1 receptor blocker rimonabant on weight reduction and cardiovascular risk factors in overweight patients: 1-year experience from the RIO-Europe study. Lancet 2005;365:13891364. 182. White A, Resch K, Ernst E. A metanalysis of acupuncture techniques for smoking cessation. Tob Control 1999;8:393-397. 183. Yiming C, Changxin Z, Ung WS, Lei Z, Kean LS. Laser acupuncture for adolescent smokers - a randomised, double-blind controlled trial. Am J Chin Med 2000;28:443-449. 184. Abbot NC, Stead LF, White AR, Barnes J, Ernst E. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev 1998;2:CD001008. 185. Bolliger CT, Zellweger JP, Danielsson T, van Biljon X, Robidou A, Westin A, Perruchoud AP, Säwe U. Smoking reduction with oral nicotine inhalers: double blind, randomised clinical trial of efficacy and safety. BMJ 2000;321:329-333. 186. Wennike P, Danielsson T, Landfeldt T, Westin Å, Tønnesen P. Smoking reduction promotes smoking cessation: Results from a double blind, randomised, placebo-controlled trial of nicotine gum with 2-year follow-up. Addiction 2003;98:1395-1402. 187. Hughes JR, Cummings KM, Hyland A. Ability of smokers to reduce their smoking and its association with future smoking cessation. Addiction 1999;94:109-114. 188. Gotfredsen N, Prescott E, Osler M, Vestbo J. Predictors of smoking reduction and cessation in a cohort of Danish moderate and heavy smokers. Prev Med 2001;33:46-52. 189. Tønnesen P, Danielsson T. Cutting down smoking then stopping with nicotine replacement therapy: an innovative approach to smoking cessation. Thorax 2005;60(Suppl.II):ii36. 190. Hughes JR, Carpenter MJ. Can medications or behavioral treatment reduce smoking in smokers not trying to quit? A review. Proceedings of the Society for Research on Nicotine and Tobacco 2005:8. 191. Hughes JR. Smoking reduction: efficacy and implementation. Addiction 2000;95(Suppl.1):S3-S37. 192. Bates C, McNeill A, Jarvis M, Gray N. The future of tobacco product regulation and labelling in Europe: Implications for the forthcoming European Union directive. Tob Control 1999;8:225-235. 193. Fagerström KO, Hughes JR, Rasmussen T, Callas PW. Randomised trial investigating effect of a novel nicotine delivery device (Eclipse) and a nicotine oral inhaler on smoking behaviour, nicotine and carbon monoxide exposure, and motivation to quit. Tob Control 2000;9:327-333. 194. Gray N, Henningfield JE, Benowitz NL, Connolly GN, Dresler C, Fagerstrom K, Jarvis MJ, Boyle P. Toward a comprehensive long term nicotine policy. Tob Control 2005; 14:161-165. 195. Glynn TJ, Manley MW. How to help your patients to stop smoking: A National Cancer Institute Manual for Physicians. NIH Publication No. 93-3064. Bethesda, National Institutes of Health, 1993. 196. Prochaska JO, Goldstein MG. Process of smoking cessation. Implications for clinicians. Clin Chest Med 1991;12:727-735. 197. Jarvis MJ, Russell MA, Saloojee Y. Expired air carbon monoxide: a simple breath test of tobacco smoke intake. BMJ 1980;281:484-485. 198. Heffner JE. The overarching challenge. Chest 2000;118(Suppl.2): 1S-3S. 199. Smith WR. Evidence for the effectiveness of techniques to change physician behavior. Chest 2000;118(Suppl2):8S-17S. 200. Heffner JE, Alberts WM, Irwin R, Wunderink R. Translating guidelines into clinical practice. Recommendations to the American College of Chest Physicians. Chest 2000;118(Suppl.2):70S-73S. 201. Nardini S, Bertoletti R, Rastelli V, Donner CF. The influence of personal tobacco smoking on the clinical practice of Italian chest physicians. Eur Respir J 1998;12:1450-1453. 202. European Smoke-Free Hospital Network. http:// ensh.aphp.fr. Date last accessed: November 28, 2006. Date last modified: November 23, 2006. 203. Johnson E, Dominici F, Griswold M, Zeger SL. Disease cases and their medical costs attributable to smoking: an analysis of the national medical expenditure survey. J Econometrics 2003;112:135151. 204. Barendregt JJ, Bonneux L, van der Maas J. The health care costs of smoking. N Engl J Med 1997;337:1052-1057. 205. Ruff LK, Volmer T, Nowak D, Meyer A. The economic impact of smoking in Germany. Eur Respir J 2000;16:385-390. 206. Parrott S, Godfrey C, Raw M, West R, McNeill A. Guidance for commissioners on the cost effectiveness of smoking cessation interventions. Thorax 1998;53(Suppl.5):S1-S38. 207. Godfrey C. The economic and social costs of lung cancer and the economics of smoking prevention. Monaldi Arch Chest Dis 2001;56:458-461. 208. World Health Organization. Economic Consequences of Smoking MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 45 219. 220. 221. 222. 223. 224. 225. 226. 227. 228. nicotine replacement therapy (NRT) for smoking cessation. York, University of York, 2002. Invernizzi G, Nardini S, Bettoncelli G, Codifava A, Corti F, Fossati R, Guerra C, Lavecchia C, Lazzaro C, Sabato E, Zuccaro P. L'intervento del medico di medicina generale nel controllo del fumo. Rassegna di Patologia dell'Apparato Respiratorio 2002;17:55-70. Baker D, Illsley R. Inequalities in health. Studies in inequality in health need careful interpretation. BMJ 1998;317:1659. Whitfield L. Social policies ''must focus on inequalities''. Health Service Journal 1998;108:8. Harris JE, Chan SW. The continuum-of-addiction: cigarette smoking in relation to price among Americans aged 15-29. Health Econ 1999;8:81-86. Becker GS, Murphy KM. A theory of rational addiction. Journal of Political Economy 1988;96:675-700. Becker GS, Grossman M, Murphy KM. An empirical analysis of cigarette addiction. American Econ Rev 1994;84:396-418. Chaloupka FJ, Tauras J, Grossman M. Economic models of addiction and applications to cigarette smoking and other substance abuse. Chicago, University of Illinois 1999;1-27. Chaloupka FJ. Tobacco taxation. www.impacteen.org/ generalarea_PDFs/NCSLSEATTLE111601.pdf. Date last accessed: September 22, 2006. Chaloupka FJ. Price, tobacco control policies and youth and young adult tobacco use. www.impacteen.org/generalarea_PDFs /TUPTI082401.pdf. Date last accessed: September 22, 2006. Cornuz J, Gilbert A, Pinget C, et al. Cost-effectiveness of pharmacotherapies for nicotine dependence in primary care settings: a multinational comparison. Tobacco Control 2006;15:152-159. L Carrozzi, C Lazzaro, S Nardini, F Pistelli, P Silvi, G Viegi Documento ufficiale - Official statement (ECOS) model. WHO European Partnership Project to Reduce Tobacco Dependence. Copenhagen-Geneva, World Health Organization, 1999. 209. Lazzaro C. Health and Economic Consequences of Smoking (ECOS) model. WHO European Partnership Project to Reduce Tobacco Dependence. Appendix 1. Copenhagen-Geneva, World Health Organization, 1999. 210. Parrott S, Godfrey C, Raw M. Costs of employee smoking in the workplace in Scotland. Tob Control 2000;9:187-192. 211. Drummond MF, O'Brien BJ, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes, 2nd edn. Oxford, Oxford University Press, 1997;109-112. 212. Gold MR, Siegel JE, Russel LB, Weinstein MC. Cost-effectiveness in health and medicine. New York, Oxford University Press, 1996. 213. Maynard A. Developing the health care market. Econ J 1991;101:1277-1286. 214. Schulmann KA, Lorna AL, Glick HA, Eisenberg J. Cost effectiveness of low-dose zidovudine therapy for asymptomatic patients with human immunodeficiency virus (HIV) infection. Ann Int Med 1991;114:798-802. 215. Mölken MP, Van Doorslaer EK, Rutten FF. Economic appraisal of asthma and COPD care: a literature review 1980-1981. Soc Sci Med 1992;35:161-175. 216. Cromwell J, Bartosch WJ, Fiore MC, Hasselblad V, Baker T. Costeffectiveness of the clinical practice recommendations in the AHCPR guideline for smoking cessation. Agency for Health Care Policy and Research. JAMA 1997;278:1759-1766. 217. Department of Health. Independent inquiry into inequalities in health. London, Stationery Office, 1998. 218. NHS Centre for Reviews & Dissemination. A rapid and systematic review of the clinical and cost effectiveness of bupropion SR and MRM 45 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 46 Background statements / Basi razionali, AIMAR Top Seminars 2009 “Inflammation and infection in the upper and lower respiratory tract”, Expert Opinion Consensus/Dissensus Seminar, Stresa, Italy, April 1-4, 2009 AIMAR Top Seminars 2009 “Inflammation and infection in the upper and lower respiratory tract”, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 1-4, 2009: background statements AIMAR Top Seminars 2009 “Infiammazione e infezione nelle vie respiratorie superiori e inferiori”, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, 1-4 aprile 2009: le basi razionali Claudio F. Donner Mondo Medico, Centro diagnostico, terapeutico e riabilitativo multidisciplinare, Borgomanero (NO) INTRODUCTION Diseases of the upper airway (from nose down to vocal cords) and lower airway (below the vocal cords) have historically been considered as separate anatomical and histological entities (the pathophysiology of rhinitis was different from that of asthma) and coming under two different specialties as regards the treatment (otolaryngology for the upper airway, pulmonology for the lower airway). We now know that, notwithstanding different facets of clinical management of these two regions, there is one united airway, i.e. diseases that affect one part of the airway often impact on other parts. The united airway disease (UAD) hypothesis, in fact, proposes that upper and lower airway disease are both manifestations of a single inflammatory process within the respiratory tract, drawing support from increasing evidence of a systemic link between the upper and lower airways [1]. The UAD hypothesis argues that any disease process that affects the upper airway is likely to affect the lower airway, and vice versa, by both direct and indirect means. Hence, rhinitis and asthma represent the manifestations of one syndrome in two parts of the respiratory tract, the upper and lower airways, respectively. At the low end of the severity spectrum, rhinitis may occur alone; in the middle range, rhinitis and airway hyperresponsiveness (AHR) may be present; at the high end of the spectrum, rhinitis and asthma may both be present, with the severity of each condition tracking in parallel [2,3]. Disease manifestations in the upper and lower air- + Claudio F. Donner Mondo Medico, Centro diagnostico, terapeutico e riabilitativo multidisciplinare Via Monsignor Cavigioli 10, 28021 Borgomanero (NO), Italia email: [email protected] Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 46 MRM MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 47 lationship and a vertical one. The concept of a horizontal relationship is based on evidence of a wide spectrum of disease severity in UAD, with disease manifesting in different parts of the respiratory tract according to the severity, e.g. at low severity only in the nasal area vs. at high severity in both upper and lower airways with asthma and rhinitis combined. The concept of a vertical relationship implies that events that take place in the upper airway may negatively affect what happens in the lower airway. For instance, the nose acts as an air conditioner to warm and humidify the air before it reaches the lower airway, but, if the nose is congested, that process is impeded. We also know that patients with asthma who get a sinus infection may often begin to wheeze. This delicate and complex interrelationship between the upper and lower airways, which most likely is at least partially mediated by the autonomic nervous system, is not yet well understood. Supporting the notion of both a horizontal and vertical relationship between the upper and lower airways is the fact that the vast majority (> 80%) of patients with asthma also have concomitant rhinitis or rhinosinusitis. Patients with asthma have more severe rhinitis or rhinosinusitis than patients without asthma. Often in a given patient, several measurable outcomes of rhinitis and asthma show a close correlation. Patients with rhinitis are at higher risk of developing asthma. Patients who have allergen introduced into the nasal airway may show both functional and inflammatory changes in the lower airway. Studies demonstrate also that treatment of nasal symptoms results in beneficial effects for the lower airway. Several factors may account for this interrelationship, e.g. when the nose is congested, patients often breathe through the mouth. When this occurs, the warming, filtering, and humidification of inspired air does not take place as it does when one breathes through the nose. With mouth breathing, the air may also have a higher concentration of inspired particulates and gaseous irritants. Secondly, patients with rhinitis who have increased responsiveness to irritants, presumably occurring via sensory nerves in the nasal membranes, may manifest bronchoconstriction via parasympathetic nerve pathways [16]. Sensorineural stimulation of the nasal airway may also stimulate increased bronchial responsiveness via the central nervous system to receptors actually present in the lower airway. This phenomenon is called the bronchial reflex. This falls under the concept of central sensitization, first noted by researchers studying pain medicine [16]. Upper airway inflammation may also propagate systemically and affect the lower airway. Experimentally, there is evidence for this concept. For example, intranasal allergen challenge has been found to result in increased expression of adhesion molecules in the pulmonary vasculature and lower airway eosinophilia. From a treatment point of view, two main aspects should be emphasized: • the unity of the respiratory airways and the influence exerted by the nose on the bronchi • the fact that both symptoms and allergic inflam- CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 ways may be linked via a systemic inflammatory response. This hypothesis holds for not only allergic but also non-allergic presentations. Several mechanisms to explain the interaction between the upper and lower airways have been proposed. The most likely mechanism is that localised airway inflammation leads to a systemic response, with bone marrow involvement resulting in the release of progenitor cells that are then recruited to tissue sites [4,5]. Several observations support the concept of UAD existing outside a purely allergic context. For example, infective inflammation occurring in both the upper and lower airways is often attributed to a direct viral effect at both sites, but the two may also be linked by indirect means [1]. The presence of lower AHR without symptoms of clinical asthma has been well documented in population studies. In addition, the relationship between AHR and inflammation is complex, with many studies not supporting a clear link between the two. As airway inflammation is central to the concept of UAD, it is possible that the upper airway may not be involved in isolated, non-asthmatic AHR. Eosinophilic bronchitis, a newly identified condition of the lower airway associated with persistent cough, is an example of lower airway inflammation without AHR, but, as yet, upper airway disease has not been investigated in association with this condition [6]. The prevalence of atopy, rhinitis and asthma have all increased worldwide over recent decades [9]. In a series of population studies of Australian schoolchildren, hay-fever prevalence increased between 1982 and 2002 from 9.1% to 38.4%, and prevalence of current asthma (defined as recent wheeze and AHR) increased from 4.5% to 11.3% [10]. Other studies indicate that rhinitis is a risk factor for later developing asthma (odds ratio, 2.59 to 11.0) [10,11]. An analysis of the same population showed that the presence of hay fever at the age of 8-10 years was predictive of the presence of troublesome asthma by the age of 23-25 years (likelihood ratio, 2.14; 95% CI, 1.59-2.89) [12]. It is well documented that allergic rhinitis is associated with increased AHR, even if there is no diagnosis of asthma [13]. People subject to allergic rhinitis have AHR present both outside the pollen season (11%-73%) and during the pollen season (50%) [1]. Clinical studies indicate that 80-100% of patients with asthma have rhinitis and 50% of patients with rhinitis have asthma, and that both the presence and severity of rhinitis are associated with worse asthma outcomes [1]. An association between asthma and sinusitis has long been recognised. In a recent study, 100% of subjects with severe asthma (requiring steroid treatment) had abnormal sinus at computed tomography scans versus 77% of subjects with mild to moderate asthma [14]. However, perhaps the most direct evidence of the relationship between rhinitis, sinusitis and asthma comes from studies that show significant improvement in asthma symptoms when sinusitis is appropriately treated [15]. Under the umbrella term of UAD, two coexistent relationships between the upper (nasal) airway and lower airway have been proposed: a horizontal re- MRM 47 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 48 48 MRM mation should be targets for treatment. Indeed, there is evidence suggesting that optimal control of rhinitis has a beneficial effect on asthma in terms of reduction of bronchial responsiveness during natural exposure to the offending allergens. Thus, one of the new clues to the treatment of UAD is the evidence of a synergistic effect of drugs used in both rhinitis and asthma. This aspect is relevant since it would allow treatment to be harmonised, possibly reducing the dosage of each drug. Ultimately, this may result in better control of the disease(s) and fewer side effects [17]. The existence of persistent airway inflammation suggests the need for continuous rather than on demand treatment. Studies have demonstrated a decrease in exacerbation rate in asthmatic patients treated to control airway hyperresponsiveness or eosinophilia compared with those treated to control clinical parameters only [18,19]. There is also evidence that airway hyperresponsiveness continues to improve in response to long term anti-inflammatory therapy, emphasising the importance of continuing regular controller treatment even when clinical endpoints have been normalised. Another lower airway inflammatory disease, chronic obstructive pulmonary disease (COPD), may also be an example of UAD. COPD is associated with elevated levels of intranasal interleukin (IL)-8, which correlates with sputum levels, indicating concomitant upper and lower airway inflammation [7]. In COPD exacerbation there is, as well as a pan-airway response, evidence of a systemic response as determined by elevated serum levels of IL-6 and C-reactive protein. But, with a predominantly infective stimulus, it is more difficult to separate site-specific effects of the provoking agent from underlying systemic processes [8]. Our traditional understanding of COPD has focused on the presence of chronic airflow obstruction and, accordingly, therapy has been mainly directed to relieve this. More recently, it has been demonstrated that airflow limitation is associated with an abnormal inflammatory response, and that the latter appears to be responsible for specific effects on mucociliary function, structural changes in the airways and lung parenchyma and extra-pulmonary systemic effects of COPD, including impairments of metabolism and inflammation, that lead to comorbid conditions [20,21]. Optimal therapeutic targeting of COPD depends on a clear understanding of the precise mechanisms of these complex processes and on early and correct evaluation of disease severity. At present, a combination of pharmacological and nonpharmacological approaches seems to be the most effective strategy to face this multi-component disease. As regards pharmacotherapy, bronchodilators and inhaled corticosteroids have shown complementary mechanisms of action, targeting different arms of the vicious cycle of COPD: a combination of the two types of drugs has the potential to address several major components of the disease, including airflow limitation, mucociliary dysfunction, and airway inflammation [22]. This translates into improvement of several clinical outcomes such as dyspnea, exacerbations and quality of life. Furthermore, since COPD is a progressive disease, with lung function worsening over time, a major target of the therapy is to modify its clinical course, i.e. slow down the evolution of lung damage to respiratory failure and improve survival. Recent evidence suggests that appropriate pharmacological therapy can reduce the long term decline of FEV1 in patients with moderate-to-severe COPD, thus slowing disease progression, and has a favourable trend on survival [23,24]. According to these data, the regulatory authorities have approved the use of the preformed combination of inhaled corticosteroid and long-acting bronchodilator (fluticasone propionate and salmeterol xinafoate) in patients with FEV1 < 60%, confirming the importance of early treatment of COPD. The primary reason for this Consensus/Dissensus Seminar is to discuss in depth the different views (otolaryngologist and pulmonologist) on the relationship between upper and lower airways, with emphasis on common pathophysiologic mechanisms and how treatment of the upper airways can benefit the lower airways. Common to both the upper and lower airways are the triggers, many of the inflammatory cells and mediators, and the treatment modalities. By contrast, there are organ-specific differences in the reaction to various stimuli in the nose or lung, with each organ manifesting its own “vocabulary” of response. To clarify these issues in a rigorous scientific “evidence based” context, the Scientific Interdisciplinary Society for Research in Lung Disease (AIMAR) has organized, in cooperation with the Italian Society of Otolaryngology (SIO), as part of its AIMAR Top Seminars 2009 program, a dedicated scientific event: “Inflammation and infection in the upper and lower respiratory tract”, Expert Opinion Consensus/ Dissensus Seminar, to be held in Stresa, April 1-4, 2009. The aim is to view the two perspectives alongside each other in a format that allows the best possible opportunity for discussion and debate: a 30-min front lecture followed by one or more interventions by dedicated discussants (10 min each) followed by general discussion amongst a highly selected faculty audience. A final Round Table will focus specifically on the consensus or dissensus emerging from the seminar and on future possible developments. We have invited leading experts from the two specialties, plus about 20 highly qualified discussants and another 30 well-known clinicians working in the field as faculty. The object is to arrive at a final consensus or dissensus on this topic, and produce a Statement that will help clarify the issue for practising clinicians. The format of the Seminar resembles that of a top-level “Expert Opinion” with the added input of evidence from the latest scientific research. The following brief summaries present the background or rationale of the main arguments that will be presented for discussion at the meeting in Stresa. Following the meeting, a report will be published in Multidisciplinary Respiratory Medicine. We hope that this scientific event, and the ensuing publication, will help clarify this stimulating issue and lead to a better understanding of airways disease. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 49 1. Corren J, Togias A, Bousquet J, eds. Lung biology in health and disease. Volume 181: Upper and lower respiratory disease. New York: Marcel Dekker, 2003. 2. Togias A. Rhinitis and asthma: evidence for respiratory system integration. J Allergy Clin Immunol 2003;111:1171-1183. 3. Rimmer J, Ruhno JW. Rhinitis and asthma: united airway disease. Med J Aust 2006;185:565-571. 4. Chanez P, Vignola AM, Vic P, Guddo F, Bonsignore G, Godard P, Bousquet J. Comparison between nasal and bronchial inflammation in asthmatic and control subjects. Am J Respir Crit Care Med 1999;159:588-595. 5. Vachier I, Vignola AM, Chiappara G, Bruno A, Meziane H, Godard P, Bousquet J, Chanez P. Inflammatory features of nasal mucosa in smokers with and without COPD. Thorax 2004;59:303-307. 6. Berry MA, Hargadon B, McKenna S, Shaw D, Green RH, Brightling CE, Wardlaw AJ, Pavord ID. Observational study of the natural history of eosinophilic bronchitis. Clin Exp Allergy 2005;35:598-601. 7. Hurst JR, Wilkinson TM, Perera WR, Donaldson GC, Wedzicha JA. Relationships among bacteria, upper airway, lower airway, and systemic inflammation in COPD. Chest 2005;127:1219-1226. 8. Hurst JR, Perera WR, Wilkinson TM, Donaldson GC, Wedzicha JA. Systemic and upper and lower airway inflammation at exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2006;173:71-78. 9. Toelle BG, Ng K, Belousova E, Salome CM, Peat JK, Marks GB. Prevalence of asthma and allergy in schoolchildren in Belmont, Australia: three cross sectional surveys over 20 years. BMJ 2004;328:386-387. 10. Guerra S, Sherrill DL, Martinez FD, Barbee RA. Rhinitis as an independent risk factor for adult-onset asthma. J Allergy Clin Immunol 2002;109:419-425. 11. Toelle BG, Xuan W, Peat JK, Marks GB. Childhood factors that predict asthma in young adulthood. Eur Respir J 2004;23:66-70. 12. Bresciani M, Paradis L, Des Roches A, Vernhet H, Vachier I, Godard P, Bousquet J, Chanez P. Rhinosinusitis in severe asthma. J Allergy Clin Immunol 2001;107:73-80. 13. Tosca MA, Cosentino C, Pallestrini E, Caligo G, Milanese M, Ciprandi G. Improvement of clinical and immunopathologic parameters in asthmatic children treated for concomitant chronic rhinosinusitis. Ann Allergy Asthma Immunol 2003;91:71-78. 14. Greiff L, Andersson M, Svensson C, Linden M, Wollmer P, Brattsand R, Persson CG. Effects of orally inhaled budesonide in seasonal allergic rhinitis. Eur Respir J 1998;11:1268-1273. 15. Stelmach R, do Patrocínio T, Nunes M, Ribeiro M, Cukier A. Effect of treating allergic rhinitis with corticosteroids in patients with mild-to-moderate persistent asthma. Chest 2005;128:3140-3147. 16. De Benedetto M, Bellussi L, Cassano P, Cataldi A, De Benedetto F, De Campora E, Foresi A, Passali D. Consensus report on the diagnosis of rhino-bronchial syndrome (RBS). Acta Otorhinolaryngol Ital 2003;23:406-408. 17. Passalacqua G, Ciprandi G, Canonica GW. United airways disease: therapeutic aspects. Thorax 2000;55(Suppl. 2):S26S27. 18. Jayaram L, Pizzichini MM, Cook RJ, Boulet LP, Lemière C, Pizzichini E, Cartier A, Hussack P, Goldsmith CH, Laviolette M, Parameswaran K, Hargreave FE. Determining asthma treatment by monitoring sputum cell counts: effect on exacerbations. Eur Respir J 2006; 27:483-494. 19. Sont JK, Willems LN, Bel EH, van Krieken JH, Vandenbroucke JP, Sterk PJ. Clinical control and histopathologic outcome of asthma when using airway hyperresponsiveness as an additional guide to long-term treatment. The AMPUL Study Group. Am J Respir Crit Care Med 1999;159:1043-1051. 20. Agustí AG. COPD, a multicomponent disease: implications for management. Respir Med 2005;99:670-682. 21. Agustí A. Systemic effects of chronic obstructive pulmonary disease. What we know and what we don't know (but should). Proc Am Thorac Soc 2007;4:522-525. 22. Cazzola M, Dahl R. Inhaled combination therapy with long-acting β2-agonists and corticosteroids in stable COPD. Chest 2004;126:220-237. 23. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J; TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007;356:775-789 24. Celli BR, Thomas NE, Anderson JA, Ferguson GT, Jenkins CR, Jones PW, Vestbo J, Knobil K, Yates JC, Calverley PM. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med 2008;178:332-338. CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 References MRM 49 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 50 Pathogenesis of respiratory inflammation Patogenesi dell'infiammazione respiratoria Giuseppe Di Maria Department of Internal Medicine, Respiratory Diseases Section, University of Catania, Catania, Italy Airways 'inflammation' plays a key role in the pathogenesis of airways disease and remodeling in COPD as well as in a number of other disease states including bronchial asthma, respiratory tract infections, cystic fibrosis, bronchiolitis and bronchiectasis. Inflammatory cells such as macrophages, neutrophils, eosinophils, CD8+ T lymphocytes, and subsequent changes which include epithelial damage and mucus hypersecretion have been investigated in a number of studies. Notably in COPD, which is also characterized by parenchymal destruction, the heterogeneity of the disease has hindered data interpretation, while extrapolation of the results of relatively non-invasive studies to the actual pathology found in the distal lung is difficult. Thus, major studies have frequently elicited conflicting interpretation, and a detailed profile of disease phenotype-specific inflammation of COPD as well as the importance of spill-over of inflammatory mediators into the circulating blood has yet to emerge. Further investigations are needed to link the different clinical and functional phenotypes of COPD to their respective inflammatory profiles in the airways thus improving the understanding of the pathogenesis of the disease as a whole. The acute effects of cigarette smoking on inflammation and oxidative stress in acute smoke exposure can result in tissue damage, as suggested by increased reactive oxygen species and products of lipid peroxidation and degradation of extracellular matrix pro- teins. Acute cigarette smoke exposure, however, has also a suppressive effect on the number of eosinophils and several inflammatory cytokines, possibly due to the antiinflammatory effect of carbon monoxide. Hopefully, in the near future data from studies on airway and parenchymal inflammation in COPD will prove useful to identify and assess the causes, severity, prognosis, and response to treatment. References 1. James AL, Wenzel S. Clinical relevance of airway remodelling in airway diseases. Eur Respir J 2007;30:134-155. 2. Hill A, Gompertz S, Stockley R. Factors influencing airway inflammation in chronic obstructive pulmonay disease. Thorax 2000;55:970-977. 3. Boser SR, Park H, Perry SF, Ménache MG, Green FH. Fractal geometry of airway remodeling in human asthma. Am J Respir Crit Care Med 2005;172:817-823. 4. De Rose V. Mechanisms and markers of airway inflammation in cystic fibrosis. Eur Respir J 2002;19:333-340. 5. Fuschillo S, De Felice A, Balzano G. Mucosal inflammation in idiopathic bronchiectasis: cellular and molecular mechanisms. Eur Respir J 2008;31:396-406. 6. Openshaw PJ, Tregoning JS. Immune responses and disease enhancement during respiratory syncytial virus infection. Clin Microbiol Rev 2005;18:541-555. 7. Barnes PJ, Chowdhury B, Kharitonov SA, Magnussen H, Page CP, Postma D, Saetta M. Pulmonary biomarkers in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2006;174:6-14. Cytology of inflammation Citologia dell'infiammazione Matteo Gelardi, Maria Luisa Fiorella, Cosimo Russo, Raffaele Fiorella Department of Otolaryngology II, University of Bari, Center of Rhinology, Bari, Italy Infective and inflammatory diseases of the nasalsinus cavities are microscopically characterized by the presence of cell populations and microbial agents that are not present under normal conditions. Characteristically, the nasal-sinus mucosa is made up of pseudo-stratified ciliated epithelium, represented by ciliated cells, mucin producing cells, striated and basal cells, and the presence of few neutrophils. In inflammatory conditions there may be bacteria, mycotic spores, eosinophils and mast cells, in different percentages, depending on the disease [1]. Nasal inflammation with signs of rhinitis can be 50 MRM caused by numerous factors, among which the common cold and allergic diseases (allergic rhinitis) are the most frequent. There are other causes, such as non-infective, non-allergic rhinitis and vasomotor conditions of nasal inflammation that give rise to particularly serious forms of rhinitis, very difficult to treat and which require advanced methods of diagnosis [2]. Cytological investigation of the nasal mucosa represents the gold standard for diagnosis of numerous rhinological diseases. In particular, through cytological investigation it is possible to diagnose a group of non-allergic “infective rhinitis”, such as: MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 51 FIGURE 1: FOUR MAIN TYPES OF NON-ALLERGIC (INFLAMMATORY) RHINITIS AS DEFINED BY CYTOLOGICAL INVESTIGATION OF THE NASAL MUCOSA A: non-allergic rhinitis with eosinophilia (NARES); B: non-allergic rhinitis with mast cells (NARMA); C: non-allergic rhinitis with neutrophilia (NARNA); D: non-allergic rhinitis with eosinophilia and mast cells (NARESMA). Magnification 1000X. rect diagnosis in the course of the first visit, especially if the specialist does not advise routine tests for allergic rhinitis disorders (history, prick test, endoscopy, nasal cytology, rhinomanometry, diagnostic kits for specific nasal provocation tests, etc.). Since these are cellular disorders, it is indispensable to perform a microscopic diagnosis of the nasal mucosa in order to determine the prevalent cellular type to arrive at a precise diagnosis. Another frequent finding during history taking of these patients is the surgical treatment of the turbinates to resolve the “obstructed nasal passages”. These surgical procedures are however insufficient and sometimes damaging to the patient, causing scarring (turbinate-septal synechiae), crusting rhinitis, and atrophy of the mucosa. Typical of these forms of rhinitis is the chronic use of nasal decongestants containing nafazoline, or similar compounds to reduce nasal congestion. It must be kept in mind that chronic use of nasal decongestants can cause a serious form of rhinitis ('pharmacological rhinitis') that can be superimposed on the pre-existing condition. Concerning the medical therapy of chronic nasal congestion, the point of no return exists where either systemic or topical therapy does not have any effect on the symptoms; therefore surgical intervention on the turbinates appears to be justified with a return to medical therapy after surgery (topical or systemic corticosteroids, antihistamines, antileukotrienes, etc.). The correct therapeutic orientation is very often “personalized” temporally, depending on the disease, in the hope of not intervening surgically once again, or developing complications. Another important aspect of these “cellular” rhinological disorders is the frequent association with nasal polyps to hypothesize a natural evolution of the disease. In fact, it has been clear since 1980 that it is not allergic rhinitis that determines such evolution, since nasal polyps accompany non-allergic rhinitis in 70-80% of the cases. We are in the process of confirming the predisposition of these cellular rhinological disorders to complications that include polyposis and asthma [6]. The data show a greater incidence of polyps and asthma in cellular rhinological diseases than in allergic rhinitis (polyps: 11.5% vs 1.7%; asthma 12% vs 6.7%). In final analysis, the clinical concept that cellular rhinological diseases are all associated must be reaffirmed. Since they are chronic diseases, chronic therapy is necessary plus a personalized follow up aimed at controlling the symptoms and prevention of the complications (rhinosinusitis, polyposis, asthma, etc.) [7]. It is the specific duty of the specialist to explain clearly and exhaustively all the information regarding the specific rhinological disease and to institute a programmed therapeutic protocol, but letting the patient know all the limitations or the strengths of the therapy and the limits of pharmacological treatment in controlling the disease, in order not to induce false expectations of a definitive recovery. CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 non-allergic rhinitis with eosinophilia (NARES) (Figure 1A), non-allergic rhinitis with mast cells (NARMA) (Figure 1B), non-allergic rhinitis with neutrophilia (NARNA) (Figure 1C), and non-allergic rhinitis with eosinophilia and mast cells (NARESMA) (Figure 1D) [3,4]. These forms are usually termed “aspecific”, a definition showing the poor knowledge of the etiological factors causing these specific diseases and a premise for the many diagnostic and therapeutic failures seen in common practice. The pseudo-allergic symptoms of these diseases are usually accompanied by nasal obstruction, pruritus, sneezing, burning sensation of the nasal mucosa, rhinorrhea, etc. These symptoms are often confused with IgE mediated rhinitis. They also present with an aspecific reactivity, which manifests with symptoms deriving from a change in posture, temperature changes, cold air, intense odours, and tobacco smoke. These symptoms are often misdiagnosed as vasomotor rhinitis. The intense and persistent nasal symptoms, together with the tendency to associate these symptoms with more serious diseases, such as bronchial asthma, aspirin sensitivity, rhinobronchial syndrome, nasal polyps, and sinusitis, is a negative aspect of these rhinopathies which should not be taken lightly in terms of health care spending and the quality of life of these patients. [5] A careful history of patients with these forms of rhinological disorders has revealed that a large number of them have consulted more than one specialist, e.g. ear, nose & throat (ENT) specialists, allergologists, pediatricians and lung specialists) before arriving at a definitive diagnosis. In our opinion nasal cytology is an essential item of evidence that allows a correct diagnosis of these rhinological diseases. In fact, ENT specialists rarely arrive at a cor- MRM 51 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 52 References 1. Gelardi M. Atlas of Nasal Cytology. Torino, Italy. Centro Scientifico Editore, 2006. 2. Bachert C. Persistent rhinitis - allergic or nonallergic? Allergy 2004;59(Suppl 76):11-15. 3. Gelardi M, Maselli del Giudice A, Fiorella ML, Fiorella R, Russo C, Soleti P, Di Gioacchino M, Ciprandi G. Non-allergic rhinitis with eosinophils and mast cells constitutes a new severe nasal disorder. Int J Immunopathol Pharmacol 2008;21:325-331. 4. Ellis AK, Keith PK. Nonallergic rhinitis with eosinophilia syndrome and related disorders. Clin Allergy Immunol 2007;19:87-100. 5. Gelardi M, Maselli Del Giudice A, Fiorella ML, Soleti P, Di Gioacchino M, Conti CM, Fulcheri M, Doyle R, Ciprandi G. Quality of life in non-allergic rhinitis depends on the predominant inflammatory cell type. J Biol Regul Homeost Agents 2008;22:73-81. 6. Gelardi M, Russo C, Fiorella ML, Fiorella R, Ciprandi G. Cell types in nasal polyps. Cytopathology 2009 (in press). 7. Gelardi M, Fiorella ML, Leo G, Incorvaia C. Cytology in the diagnosis of rhinosinusitis. Pediatr Allergy Immunol 2007;18(Suppl 18):50-52. Inflammation in upper and lower airways: similarities and differences Infiammazione nelle vie respiratorie superiori e inferiori: somiglianze e differenze Glenis Scadding Consultant Physician, Royal National Throat Nose & Ear Hospital, London, United Kingdom Many diseases affect both the upper and lower parts of the respiratory tract - which should really be considered as one organ, e.g. • allergic rhinits/asthma • non allergic rhinitis + eosinophils/asthma • chronic rhinosinusitis + nasal polyps/asthma • chronic rhinosinusitis without nasal polyps/ lower respiratory tract infection (Japan panbronchiolitis)/bronchiectasis • rhinitis/chronic obstructive pulmonary disease • cystic fibrosis • primary ciliary dyskinesia • hypogammaglobulinaemia • Wegener's granulomatosis • Churg Strauss syndrome • sarcoidosis • tuberculosis/leprosy • non allergic rhinitis without eosinophils/?neurogenic asthma Inflammatory processes in both areas are probably similar, but constrained by anatomy and physiology of airways, i.e. Upper respiratory tract (URT): - no smooth muscle, - highly reactive vasculature, - bony or cartilagineous skeleton, - resists expansion, - designed to cope with large volumes of particulate material/ pathogens. Lower respiratory tract (LRT): - smooth muscle, - reactive vasculature, - no skeleton, - designed to be protected by URT. 52 MRM Neurogenic influences are also likely to be involved in disease symptomatology, but are outside the scope of this article. Recent evidence suggests that in some of these conditions an aberrant response to bacteria or viruses may be highly relevant to aetiopathogenesis. Only a few of these can be considered in detail. Allergic rhinitis/asthma The overall view of respiratory allergy has changed profoundly in recent times with increasing attention focused on the relationship between rhinitis and asthma (i.e. between the upper and lower respiratory tract), first noted in epidemiological studies. Clinical observations provide compelling evidence for the co-existence of rhinitis and asthma, rhinitis as a risk factor for developing asthma, the occurrence of bronchial hyper-responsiveness in rhinitis, the association between upper respiratory infections and asthma exacerbations, the existence of common pathogenic mechanisms between rhinitis and asthma, and the exacerbating role of rhinosinusitis in asthma. More detailed knowledge of the mechanisms of inflammation has clarified the functional relationships between the nose and bronchi. It is therefore reasonable to consider respiratory allergy as a disorder of the whole respiratory tract manifest clinically as rhinitis and/or asthma, rather than as distinct diseases confined to specific organs. This approach has therapeutic implications because treating upper airways disease can improve the lower airways, and drugs affecting common inflammatory mechanisms can act on both compartments. The bronchial inflammatory response following allergen-specific challenge in patients suffering from asthma alone or rhinitis alone has been studied utilizing bronchial biopsy and lavage. No mor- MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 53 Chronic rhinosinusitis with nasal polyps/severe asthma The concept of 'united airways disease' refers not only to the link between allergic rhinitis and asthma, but also implies a possible link between sinus disease (rhinosinusitis) and asthma (allergic or nonallergic) and other lower airway diseases. The current classification of chronic rhinosinusitis (CRS) includes disease with and without nasal polyps. Different patterns of inflammatory and regulatory cytokines (involving distinguishable T-helper lymphocyte populations) and of remodelling markers were recently described differentiating nasal polyposis from CRS, yielding two discrete subgroups of CRS. These patterns resemble those of lower airway diseases, such as asthma and chronic obstructive pulmonary disease (COPD), and suggest a common aetiological/pathogenetic background. Whereas the link between nasal polyps and asthma is well established (improvement in asthma having been shown after medical or surgical treatment of sinus disease), that between CRS and lower airway disease is less well understood. The role of specific toxins released by resident bacteria, mainly Staphylococcus aureus, is under investigation. Remodelling occurs in the lower airway but is less obvious in the nose and sinuses. It is as yet uncertain whether this is because repair mechanisms are dysregulated in the lower airways. Rhinitis-rhinosinusitis/COPD COPD is characterised by sputum production, bacterial colonisation, neutrophilic bronchial airway inflammation and poor health status. COPD patients with potentially pathogenic microrganisms (PPMs) in their sputum show significantly higher levels of interleukin (IL)-8, leukotriene B4, tumour necrosis factor-α, neutrophil elastase and increased neutrophil chemotaxis. They also exhibit worse health status and raised plasma fibrinogen levels compared to the non-PPMs COPD group. Hurst et al. were the first to report a correlation between the degree of upper and lower airway inflammation in COPD. In both the upper and lower airways of patients with COPD, the IL-8 concentration was associated with indexes of bacterial colonisation. The finding of a raised IL-8 concentration in the nasal wash fluid of COPD patients even after prolonged smoking cessation is novel and suggests the presence of ongoing upper airway inflammation in these patients and that the upper and lower airways are behaving in a similar manner. Furthermore the exacerbations of COPD are associated with pan-airway inflammation, the systemic inflammatory response is proportional to that occurring in the lower airway and greater in the presence of a bacterial pathogen. References 1. Cruz AA, Popov T, Pawankar R, Annesi-Maesano I, Fokkens W, Kemp J, Ohta K, Price D, Bousquet J; ARIA Initiative Scientific Committee. Common characteristics of upper and lower airways in rhinitis and asthma: ARIA update, in collaboration with GA(2)LEN. Allergy 2007;62(Suppl 84):1-41. 2. Passalacqua G, Canonica GW. Impact of rhinitis on airway inflammation: biological and therapeutic implications. Respir Res 2001;2:320-323. 3. Braunstahl GJ, Overbeek SE, Kleinjan A, Prins JB, Hoogsteden HC, Fokkens WJ. Nasal allergen provocation induces adhesion molecule expression and tissue eosinophilia in upper and lower airways. J Allergy Clin Immunol 2001;107:469-476. 4. Braunstahl GJ, Kleinjan A, Overbeek SE, Prins JB, Hoogsteden HC, Fokkens WJ. Segmental bronchial provocation induces nasal inflammation in allergic rhinitis patients. Am J Respir Crit Care Med 2000;161:2051-2057. 5. Li J, Saito H, Crawford L, Inman MD, Cyr MM, Denburg JA. Haemopoietic mechanisms in murine allergic upper and lower airway inflammation. Immunology 2005;114:386396. 6. Marcucci F, Passalacqua G, Canonica GW, Frati F, Salvatori S, Di cara G, Petrini I, Bernini M, Novembre E, Bernardini R, Incorvaia C, Sensi LG. Lower airway inflammation before and after house dust mite nasal challenge: an age and allergen exposure-related phenomenon. Respir Med 2007;101:1600-1608. 7. Salib RJ, Drake-Lee A, Howarth PH. Allergic rhinitis: past, present and the future. Clin Otolaryngol Allied Sci 2003;28:291-303. 8. Salib RJ, Howarth PH. Remodelling of the upper airways in allergic rhinitis: is it a feature of the disease? Clin Exp Allergy 2003;33:1629-1633. 9. Watelet JB, Van Zele T, Gjomarkaj M, Canonica GW, Dahlen SE, Fokkens W, Lund VJ, Scadding GK, Mullol J, Papadopoulos N, Bonini S, Kowalski ML, Van Cauwenberge P, Bousquet J; GA(2)LEN Workpackage Members 2.7. Tissue remodelling in upper airways: where is the link with lower airway remodelling? Allergy 2006;61:1249-1258. 10. Bachert C, Patou J, Van Cauwenberge P. The role of sinus disease in asthma. Curr Opin Allergy Clin Immunol 2006;6:29-36. 11. Bachert C, Gevaert P, Zhang N, van Zele T, Perez-Novo C. Role of staphylococcal superantigens in airway disease. Chem Immunol Allergy 2007;93:214-236. 12. Zhang N, Van Zele T, Perez-Novo C, Van Bruaene N, Holtappels G, DeRuyck N, Van Cauwenberge P, Bachert C. Different types of T-effector cells orchestrate mucosal inflammation in chronic sinus disease. J Allergy Clin Immunol 2008;122:961-968. 13. Banerjee D, Khair OA, Honeybourne D. Impact of sputum bacteria on airway inflammation and health status in clinical stable COPD. Eur Respir J 2004;23:685-691. 14. Hurst JR, Wilkinson TM, Perera WR, Donaldson GC, Wedzicha JA. Relationships among bacteria, upper airway, lower airway, and systemic inflammation in COPD. Chest 2005;127:1219-1226. 15. Hurst JR, Perera WR, Wilkinson TM, Donaldson GC, Wedzicha JA. Systemic and upper and lower airway inflammation at exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2006;173:71-78. 16. Hellman D. Manifestations of Wegener's Granulomatosis in the Upper and Lower Airways. In: Corren J, Togias A, Bousquet J, eds. Upper and lower respiratory disease. Lung Biology in Health and Disease. London, Taylor & Francis, 2003;181:443-459. CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 phological difference between the two groups was found: the bronchial inflammatory response (cell influx and basement membrane thickening) was the same regardless of which airway was affected by disease, confirming that atopic subjects have a common inflammatory response. MRM 53 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 54 54 MRM Relation between infection and inflammation in the airways Relazione tra infezione e infiammazione nelle vie aeree Wisia Wedzicha Academic Unit of Respiratory Medicine, Royal Free and University College Medical School, University College London, Hampstead, London, United Kingdom Although the upper airways of normal subjects contain bacteria, the lower airways of patients without respiratory disease are usually sterile. However COPD patients and cigarette smokers develop increasing numbers of airway bacteria that is termed lower airway bacterial colonisation (LABC). The major bacteria that are known to colonise the airways are: Streptococcus pneumoniae, Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella catarrhalis, Klebsiella pneumoniae, and Pseudomonas aeruginosa. Patients who are colonised with bacteria are more likely to have airway bacteria isolated at exacerbation. Although it was initially considered that LABC was not important in the pathogenesis of COPD, thinking on this issue has changed and we now understand airway infection in COPD as a major driver of airway and thus systemic inflammation. A number of studies have now shown that the presence of airway bacteria in the lower airway is associated with increased airway inflammation and the higher the bacterial load the greater the inflammation [1]. COPD patients have increased nasal symptoms and greater upper airway inflammation compared to control subjects. We also showed that the level of inflammation was related to bacterial isolation and upper airway inflammation was related to LABC [2]. Some patients with COPD are prone to frequent exacerbations and we now know that the presence of LABC is associated with exacerbation frequency [3]. In addition changes in lower airway bacterial load are related to changes in airway inflammation and in FEV1 decline [4]. Thus treating stable COPD patients with antibiotics may have a number of important effects including preventing the severity and reducing the frequency of exacerbations. Bronchiectatic changes on CT scan are also common in COPD patients especially those with more severe disease [5]. Thus airway bacteria through increases in inflammation have the potential to produce structural changes in the airways that may be the mechanisms for the faster disease progression. In addition to airway bacteria, other infective agents also may affect the airways. Although viruses, especially rhinovirus which is the cause of the common cold and influenza, are usually recognised as triggers of exacerbation [6,7], respiratory syncytial virus (RSV) may also affect stable airways. We showed that RSV can be often detected from the stable airway and that patients with more frequent isolation of RSV have faster decline in lung function [8]. Respiratory viruses and airway bacteria are commonly found at COPD exacerbations and the inflammatory response is greater in the presence of both viruses and bacteria [9,10]. It is possible that respiratory viruses damage the airway epithelium allowing secondary bacterial infection. Exacerbations associated with sputum are also more likely to be associated with bacterial infection [11]. Exacerbations of COPD are also associated with pan-airway inflammation in that the upper and lower airways are involved, with the systemic inflammatory response being proportional to that occurring in the lower airway and greater in the presence of a bacterial pathogen [12]. References 1. Hill AT, Campbell EJ, Hill SL, Bayley DL, Stockley RA. Association between airway bacterial load and markers of airway inflammation in patients with stable chronic bronchitis. Am J Med 2000;109:288-295. 2. Hurst JR, Wilkinson TM, Perera WR, Donaldson GC, Wedzicha JA. Relationships among bacteria, upper airway, lower airway, and systemic inflammation in COPD. Chest 2005;127:1219-1226. 3. Patel IS, Seemungal TA, Wilks M, Lloyd-Owen SJ, Donaldson GC, Wedzicha JA. Relationship between bacterial colonisation and the frequency, character and severity of COPD exacerbations. Thorax 2002;57:759-764. 4. Wilkinson TM, Patel IS, Wilks M, Donaldson GC, Wedzicha JA. Airway bacterial load and FEV1 decline in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2003;167:1090-1095. 5. Patel IS, Vlahos I, Wilkinson TM, Lloyd-Owen SJ, Donaldson GC, Wilks M, Reznek RH, Wedzicha JA. Bronchiectasis, exacerbation indices and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2004;170:400-407. 6. Seemungal T, Harper-Owen R, Bhowmik A, Moric I, Sanderson G, Message S, MacCallum P, Meade TW, Jeffries DJ, Johnston SL, Wedzicha JA. Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2001;164:1618-1623. 7. Rohde G, Wiethege A, Borg I, Kauth M, Bauer TT, Gillissen A, Bufe A, Schultze-Werninghaus G. Respiratory viruses in exacerbations of chronic obstructive pulmonary disease requiring hospitalisation: a case-control study. Thorax 2003;58:37-42. 8. Wilkinson TM, Donaldson GC, Johnston SL, Openshaw PJ, Wedzicha JA. Respiratory syncytial virus, airway inflammation and FEV1 decline in patients with COPD. Am J Respir Crit Care Med 2006;173:871-876. 9. Wilkinson TM, Hurst JR, Perera WR, Wilks M, Donaldson GC, Wedzicha JA. Effect of interactions between lower airway bacterial and rhinoviral infection in exacerbations of COPD. Chest 2006;129:317-324. 10. Papi A, Bellettato CM, Braccioni F, Romagnoli M, Casolari P, Caramori G, Fabbri LM, Johnston SL. Infections and airway inflammation in chronic obstructive pulmonary disease MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 55 pulmonary disease. Thorax 2007;62:29-35. 12. Hurst JR, Perera WR, Wilkinson TM, Donaldson GC, Wedzicha JA. Systemic and upper and lower airway inflammation at exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2006;173:71-78. Diagnostic approach: clinical implications of the new experimental evidence L'approccio diagnostico: implicazioni cliniche delle nuove evidenze sperimentali Mario Cazzola Cattedra di Malattie Respiratorie, Università di Roma “Tor Vergata”, Roma, Italia Appropriate assessment of patients suffering from asthma or COPD is essential for an accurate diagnosis, assisting in making decisions about the choice of the most appropriate therapeutic interventions, measuring outcomes in response to interventions in both the clinical setting and in research investigations, and providing information about prognosis [1]. In recent years extensive research has gone into identifying and attempting to validate relevant diagnostic biomarkers and markers of disease activity and therapeutic response in these conditions [2,3]. Regrettably, although asthma and COPD tend to be thought of as different disease entities, their prevalence is so high that they may co-exist in the same patient; in addition, the literature shows clearly that there is a degree of overlap in disease biomarkers and markers [4]. Moreover, although a number of tools and techniques exist for measuring biomarkers and other markers in asthma and COPD, unfortunately as yet we do not have an ideal bio- or other marker and its potential outcome, and this is true both for asthma and COPD. An ideal biomarker or marker is one that: 1) has biological plausibility in terms of its role in the pathogenesis of the disease; 2) is associated with a clinically important outcome such as mortality; and 3) can be modified (by an effective intervention) to change the target outcome of interest [5]. Unfortunately both asthma and COPD are characterized by a range of pathological changes, including airflow limitation and inflammation, mucociliary dysfunction, structural changes in the airways and extrapulmonary systemic effects. Reflecting the multicomponent nature of these disorders, there is extensive heterogeneity among patients with asthma and/or COPD in terms of clinical presentation, disease severity and rate of disease progression. It is increasingly apparent that a single biomarker or marker is unlikely to be predictive of clinical outcome in all patients with asthma and/or COPD, given the diverse range of pathological mechanisms involved. For example, clinical asthma is widely assumed to be the net result of excessive inflammation driven by aberrant T-helper-2 (Th2) immunity that leads to inflamed, remodelled airways and then functional derangement that, in turn, causes symptoms. This notion of disease is actually poorly supported by data, and there are substantial discrepancies and very poor correlation between inflammation, damage, functional impairment, and degree of symptoms. The problem is further compounded by poor understanding of the heterogeneity of clinical disease. Failure to recognize and discover the underlying mechanisms of these major variants or endotypes of asthma is, arguably, the major intellectual limitation to progress at present. Fortunately, both clinical research and animal models are very well suited to dissecting the cellular and molecular basis of disease endotypes [6]. This approach is already suggesting entirely novel pathways to disease, e.g. alternative macrophage specification, steroid refractory innate immunity, the interleukin-17-regulatory T-cell axis, epidermal growth factor receptor co-amplification, and Th2-mimicking but non-T-cell interleukin 18 and 33 dependent processes that can offer unexpected therapeutic opportunities for specific patient endotypes. COPD is even more complex. In fact, COPD progresses slowly, and the disease is mechanistically and clinically heterogeneous. Consequently, there is considerable interest in defining biomarkers and markers that can be used to subcategorize the COPD population and gauge disease severity and progression. Expiratory airflow limitation has been the primary measure used to track the natural history of COPD. It has also been used to grade COPD severity. However, it must be emphasized that, since COPD progresses with age, severity and progression are not equivalent. It is clear, therefore, that clinical features other than airflow limitation are relevant to COPD natural history, but the number of distinct variables required to define the COPD population remains undefined. Recent research has advanced our understanding of COPD pathogenesis, leading to the identification of potential targets (biomarkers) and pathways (markers) for drug development. Unfortunately, although a large number of biomarkers and markers have been evaluated, none have yet been validated as effective CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 severe exacerbations. Am J Respir Crit Care Med 2006;173:1114-1121. 11. Soler N, Agustí C, Angrill J, Puig De la Bellacasa J, Torres A. Bronchoscopic validation of the significance of sputum purulence in severe exacerbations of chronic obstructive MRM 55 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 56 clinical tools [7-9], and this for several reasons. These reasons include: 1) the lack of validated short- and intermediate-term endpoints (or surrogates) that are predictive of future hard clinical outcomes; and 2) the lack of a method to provide precise phenotypes suitable for large-scale studies. 4. 5. References 1. Make BJ, Martinez FJ. Assessment of patients with chronic obstructive pulmonary disease. Proc Am Thorac Soc 2008;5:884-890. 2. Cazzola M, MacNee W, Martinez FJ, Rabe KF, Franciosi LG, Barnes PJ, Brusasco V, Burge PS, Calverley PM, Celli BR, Jones PW, Mahler DA, Make B, Miravitlles M, Page CP, Palange P, Parr D, Pistolesi M, Rennard SI, Rutten-van Mölken MP, Stockley R, Sullivan SD, Wedzicha JA, Wouters EF; American Thoracic Society; European Respiratory Society Task Force on outcomes of COPD. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J 2008;31:416-469. 3. Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, Casale TB, Chanez P, Enright PL, Gibson PG, de Jongste JC, Kerstjens HA, Lazarus SC, Levy ML, O'Byrne 6. 7. 8. 9. PM, Partridge MR, Pavord ID, Sears MR, Sterk PJ, Stoloff SW, Szefler SJ, Sullivan SD, Thomas MD, Wenzel SE, Reddel HK. A new perspective on concepts of asthma severity and control. Eur Respir J 2008;32:545-554. Snell N, Newbold P. The clinical utility of biomarkers in asthma and COPD. Curr Opin Pharmacol 2008;8:222-235. Bucher HC, Guyatt GH, Cook DJ, Holbrook A, McAlister FA. Users' guides to the medical literature: XIX. Applying clinical trial results. A. How to use an article measuring the effect of an intervention on surrogate end points. EvidenceBased Medicine Working Group. JAMA 1999;282:771-778. Anderson GP. Endotyping asthma: new insights into key pathogenic mechanisms in a complex, heterogeneous disease. Lancet 2008;372:1107-1119. Franciosi LG, Page CP, Celli BR, Cazzola M, Walker MJ, Danhof M, Rabe KF, Della Pasqua OE. Markers of disease severity in chronic obstructive pulmonary disease. Pulm Pharmacol Ther 2006;19:189-199. Franciosi LG, Page CP, Celli BR, Cazzola M, Walker MJ, Danhof M, Rabe KF, Della Pasqua OE. Markers of exacerbation severity in chronic obstructive pulmonary disease. Respir Res 2006;7:74. Rennard SI, Vestbo J. Natural histories of chronic obstructive pulmonary disease. Proc Am Thorac Soc 2008;5:878-883. Integrated care approach to the upper airway patient Terapia integrata nella patologia delle vie aeree superiori Delfo Casolino, Davide Padovani, Daria Salsi, Caterina Bruzzi UO Otorinolaringoiatria, Ospedale S. Maria delle Croci, Ravenna, Italia Upper respiratory tract (URT) diseases are prevalent medical conditions that may cause significant morbidity and medical treatment costs. They can decrease quality of life, and result in reduced workplace productivity and missed school days. Appropriate management of URT diseases may be an important component in effective management of coexisting or complicating conditions, such as asthma, COPD, allergic rhinoconjunctivitis, acute/chronic rhinosinusitis and acute/chronic otitis media. When investigating a patient for possible URT disorders, it is essential to obtain a complete history and physical examination: naso-pharyngo-laryngeal endoscopy with or without vasoconstriction should be performed to assess anatomic and mucosal abnormalities. Fibroscopes are commonly used and provide essential data for everyday ENT practice: the URT endoscopy can be performed with rigid (2.7 mm in diameter for children or 4 mm for adults, with different angulation of view: 0°, 30°, 45° and 70°) or with flexible endoscope (2.1 or 3.7 mm in diameter, with or without operative channel). Nasal examination is magnified by rigid endoscope, which can be considered the gold standard. The laryngeal examination should be performed using a rigid endoscope (different degree lens 70° 56 MRM and 90°) or a flexible endoscope, with a working channel that allows aspiration of the mucosal secretions. The working channel is also used to inject cold water or air in order to test or stimulate the sensitivity of the pharyngo-laryngeal mucosa. Classical flexible fiberoptic or the new flexible digital endoscope with a high definition distal chip camera can be used. The endoscope is connected to a videocamera and the images are displayed on a monitor; the examination is recorded and then analysed in slow-motion. Laryngeal videoendoscopy with or without stroboscopy is used to diagnose and document voice and larygeal disorders, track changes over time, and to provide biofeedback for voice and breathing therapy; it is a clinical tool that is also used in the office setting to examine vocal fold structure and gross function. Stroboscopy is a lighting technique that allows the examination of the body-cover relationship and vibration patterns, and it is valuable for describing mucosal disease and its effect on vocal fold vibration. Stroboscopy is necessary to study glottic closure and mucosal pliability, to make inferences about tension, and to identify lesions. Rigid and flexible endoscopes can be used with both continuous and stroboscopic light sources. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 57 sensitivity and functionality of the soft palate, the pharynx, larynx and cervical oesophagus. Integrated care approach to the lower airways patient Il trattamento integrato del paziente con patologie delle basse vie respiratorie Fernando De Benedetto Direttore UOC di Pneumologia, Asl Chieti, Chieti, Italia Induced inflammation of the upper airways can, through a complex interaction between cells and inflammatory cytokines, extend to the lower airways and lead to systemic consequences. Much is known today about the pathogenetic mechanisms linking the upper and lower airways. Over the years, scientific evidence supporting the association between rhinosinusitis and lower airways disease has definitively established the interrelation between the two districts and redefined the underlying pathogenetic mechanisms. Concerning the relationship between rhinitis and asthma, Braunstahl et al. analyzed, after nasal provocation with an allergen, the level of eosinophil infiltration in a group of non asthmatic subjects affected by allergic rhinitis compared to controls; they found a significantly increased infiltration of eosinophils in the epithelium and lamina propria of the nasal and bronchial mucosa, irrespective of which of the two districts was targeted by the allergenic stimulus. The same significance was found for vascular expression of ICAM-1 molecules [1,2,3]. Similar results were obtained by Chanez et al. [4]. With regard to COPD, Vachier et al. [5] investigated inflammation by analyzing the cell counts from nasal and bronchial biopsies of subjects with COPD and found differences with respect to the control group. Analogously, Hurst et al. in 2005 investigated, through dosage of IL-8 (a cytokine with a strong chemotactic and neutrophil activating effect), the nasal and bronchial inflammation in subjects with COPD and found there were differences with respect to the control group [6]. However, scant information exists about the diagnostic workup and the treatment to adopt in clinical pictures where the two districts are involved. The Consensus Report on Rhinobronchial Syndrome (RBS) [7], elaborated in 2004 by an ad hoc interdisciplinary joint working group of the Italian Otorhinolaryngology Society (SIO) and Interdisciplinary Association for Research on Lung Disease (AIMAR), defined rhinobronchial syndrome as “a nosological phenomenon that is produced when a hyperreactive, chronic or recurrent inflammatory process, in any case induced, or normal anatomical alterations of the rhinosinusal district favour the development of an inflammatory state, on infective or immunological grounds, in the lower airways, which can manifest itself also with functional impairment”. Based on this definition, a Scientific Committee composed of experts from the two Societies designed a study protocol which had as its goals to identify the characteristic symptoms of RBS, standardize an appropriate diagnostic workup and identify what is the most effective treatment option. The underlying aim was to correct the widespread dishomogeneity existing in the treatment of this disease between the different medical disciplines involved (i.e. otolaryngologists, pneumologists, allergologists, internal medicine specialists and general practitioners) in terms of the diagnostic methods and treatment models applied, with corresponding large differences in resource consumption. The study enrolled 159 subjects. In 116 of them, the diagnosis of RBS (based on the 2004 Consensus Report definition) was confirmed; the remaining 43 subjects, in whom the diagnosis was not confirmed, formed the control group. From patients' medical history, allergic diseases and recurrent infections of the airways (the prevalence of the latter was in fact double) were found to be significantly more frequent (respectively p < 0.04 and p < 0.001) in subjects affected by RBS than in the controls; clinically, RBS subjects presented significantly more marked cough (96% vs. 79%, p < 0.001) and dyspnea (69% vs. 41.9%, p < 0.002) compared to controls. The clinical picture at the level of the lower airways was a multiple one: simple chronic bronchitis (63%) most frequently found was followed by bronchial asthma (37%), chronic obstructive bronchitis (16%) and bronchiectasis (10%), while some subjects presented several pictures contemporaneously. This led the pneumologist to choose a diagnostic approach based both on lung function assessment (together with bronchial reversibility test and, where necessary, methacholine challenge) and on chest X-ray (also, in cases of suspected bronchiectasis, HRCT scan); in addition the prick test was necessary and it was positive in all subjects with a history of atopia. The treatment schemes normally employed for lower airways - i.e. antibiotics during the course of exacerbations, bronchodilators in cases of obstruction, inhaled steroids in asthma - gave positive results at the 3-month check-up, with an improvement of symptoms found in 94% of patients. Evaluating the findings from a clinical point of view, CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 Videoendoscopy, usually performed through a trans-nasal route, allows evaluation of morphology, MRM 57 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 58 a diagnostic flow-chart can be constructed that places particular emphasis on the search for symptoms such as cough and dyspnea in more or less evident association with rhinorrhea and nasal obstruction, that suggest a contemporary involvement of the two respiratory districts; if the clinical picture is not completely resolved on an empirical basis by the GP, the patient should be referred to the otolaryngologist and pneumologist for subsequent diagnostic-therapeutic management. It is the otolaryngologist's task, after fiberoptic rhinoscopy has been carried out, to seek information from the patient about a possible history of recurrent bronchitis and presence of symptoms like dyspnea and cough; in the affirmative case, assessment by the pneumologist is indicated. In the same way, it is the pneumologist's task, once lung function tests and chest imaging have been carried out, to examine the patient about a clinical history of rhinosinusitis and pharyngitis and presence of symptoms such as cough, nasal obstruction and rhinorrhea; if affirmative, assessment by the otolaryngologist is indicated. Following the above integrated (otolaryngologistpneumologist) diagnostic approach, a correct diagnostic definition of these clinical cases can be obtained; it is then simple - given the large consolidated body of evidence published on the treatment of chronic rhinosinusitis, asthma, chronic bronchi- tis and COPD - to establish what is the most appropriate treatment program. References 1. Braunstahl GJ, Fokkens W. Nasal involvement in allergic asthma. Allergy 2003;58:1235-1243. 2. Braunstahl GJ, Overbeek SE, Kleinjan A, Prins JB, Hoogsteden HC, Fokkens WJ. Nasal allergen provocation induces adhesion molecule expression and tissue eosinophilia in upper and lower airways. J Allergy Clin Immunol 2001;107:469-476. 3. Braunsthahl GJ, Kleinjan A, Overbeek SE, Prins JB, Hoogsteden HC, Fokkens WJ. Segmental bronchial provocation induces nasal inflammation in allergic rhinitis patients. Am J Respir Crit Care Med 2000;161:2051-2057. 4. Chanez P, Vignola AM, Vic P, Guddo F, Bonsignore G, Godard P, Bousquet J. Comparison between nasal and bronchial inflammation in asthmatic and control subjects. Am J Respir Crit Care Med 1999;159:588-595. 5. Vachier I, Vignola AM, Chiappara G, Bruno A, Meziane H, Godard P, Bousquet J, Chanez P. Inflammatory features of nasal mucosa in smokers with and without COPD. Thorax 2004;59:303-307. 6. Hurst JR, Wilkinson TM, Perera WR, Donaldson GC, Wedzicha JA. Relationships among bacteria, upper airway, lower airway, and systemic inflammation in COPD. Chest 2005;127:1219-1226. 7. De Benedetto M, Bellussi L, Cassano P, Cataldi A, De Benedetto F, De Campora E, Foresi A, Passali D. Consensus report on the diagnosis of rhino-bronchial syndrome (RBS). Acta Otorhinolaryngol Ital 2003;23:406-408. Pharmacology of inhaled drugs Farmacologia dei farmaci assunti per via inalatoria Francesco Scaglione Department of Pharmacology, Chemotherapy and Toxicology, University of Milan, Italy In recent years, considerable insight has been gained into the optimal management of respiratory pathologies such as chronic rhinitis, asthma and COPD. Most patients with these pathologies have mild intermittent and persistent disease, and it is acknowledged that many patients do not reach full control of all symptoms and signs. The pharmacological basis of inhaled drugs may affect their efficacy as well as safety. Inhaled steroids (ICS) The safety and efficacy profile of ICS is known to be influenced by the pharmacokinetic (PK) properties and associated pharmacodynamic (PD) effects of the drug. The efficacy of an ICS is determined by those PK characteristics that are critical for the antiinflammatory activity of the ICS in the effective control of the respiratory pathologies, whereas the safety of an ICS is improved by those PK characteristics that reduce local and systemic exposure to the active drug. The pharmacodynamic properties of 58 MRM ICS can be gleaned quickly from an assessment of their relative potency. Glucocorticoid potency can be measured in various ways, but is thought to be closely related to glucocorticoid receptor (GR) binding affinity. Figure 1 illustrates the relative GR binding affinities for most ICS. Although there is no evidence of a linear association between glucocorticoid potency and clinical response, increased potency at intranasal sites would seem desirable, because the potency, among other things, allows the reduction of daily dose. The PK properties of an ICS affect the availabilty of drug at the receptor site, as well as its potential for systemic exposure. Because the goals of ICS therapy are to deposit drug at the site of action, have it remain there as long as possible, and limit the amount that leaves the site and enters the systemic circulation, the pharmacokinetic features of particular interest are lipophilicity and systemic availability. Lipophilia is a desired characteristic in that more highly lipophilic compounds are absorbed more MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 59 Relative receptor affinity (RRA) vs dexamethasone TABLE 1: ORAL BIOAVAILABILITY OF INHALED CORTICOSTEROIDS 3500 ICS Oral bioavailability % 3000 2989 BDP BMP BUD CIC FLU FP MF TAA 15 26 11 1 7 1 1 23 2500 2244 2000 1500 1775 1345 Definition of abbreviations: BDP, beclomethasone dipropionate; BMP, beclomethasone monopropionate; BUD, budesonide; CIC, ciclesonide; FLU, flunisolide; FP, fluticasone propionate; MF, mometasone furoate; TAA, triamcinolone acetonide. From [1] mod. 1212 1000 855 500 233 177 100 Flu tic as on Mo ef me ur oa tas Flu te on tic ef as on ur oa ep t Be ropi e on clo a me te th as Cic on les e on ide Bu AP* de so Tri am nide cin olo ne Flu nis De oli xa de me th as on e 0 * Ciclesonide active principle (active metabolite) From [4] mod. quickly and thoroughly by the mucosa and retained longer in tissue, increasing exposure to the GR. In the event of systemic absorption, lipophilicity may contribute to the accumulation of drug in other tissues, possibly contributing to unwanted side effects. Thus, the ideal combination of features would include a high degree of lipophilicity coupled with low systemic absorption. The order of lipid solubility for corticosteroids has been reported as: mometasone furoate > fluticasone propionate > beclomethasone dipropionate > budesonide > triamcinolone acetonide > flunisolide. ICS can become available for systemic absorption either from the gastrointestinal tract (oral bioavailability) or from the lungs (pulmonary bioavailability). Therefore, the blood concentration of an ICS is a function of the sum of its pulmonary and orally absorbed fractions. The systemic exposure of the ICS provides limited therapeutic benefit but may increase the potential for systemic side-effects. Systemic absorption of currently available ICS varies widely (Table 1). Long-acting β2 agonists (LABA) These agents (salmeterol and formoterol) produce sustained bronchodilation and are extremely effective in providing symptomatic control for many patients. β2-adrenoceptor agonists have two main effects on the airways. First, acting via relaxation of airway smooth muscle cells, they produce bronchodila- tion. Second, previous administration of β2 agonists inhibits subsequent constrictor responses to a range of stimuli, including methacholine, histamine and allergen (i.e. it provides bronchoprotection). Salmeterol and formoterol are lipophilic and diffuse into the cell membrane. However the mechanism allowing a long term effect is different. Salmeterol possesses as part of its structure a “tail” that binds into the β-receptor at an exosite. When the tail is in association with the exosite, the molecule is prevented from dissociating from the receptor. The “head” binds to and activates the β2 receptor at the same place where albuterol binds. The head continually attaches and detaches from the receptor site, by the Charnière (hinge) principle. This repeating attachment process prolongs the drug's action. This mechanism allows a dose-independent long action. In contrast, formoterol binds the β2-receptor in a similar way to albuterol; the long action is related to the higher lipophilicity and is dose dependent. The combination of an ICS and LABA is preferred in patients with moderate to severe pathology and this combination is better than doubling the dose of ICS to achieve better asthma control and reduce exacerbation risks. Moreover the molecular mechanism of action of both LABA and ICS results in a synergism of action. Anticholinergics Tiotropium bromide is a quaternary ammonium compound structurally related to ipratropium. This compound is approved for the long-term maintenance treatment of bronchospasm associated with COPD. The potency and long duration of effect of this anticholinergic bronchodilator result primarily from a prolonged blockade of the M1 and M3 muscarinic receptors in the airways and a relatively more rapid dissociation from the M2 receptor (which provides inhibitory feedback). Regular use of the drug was associated with clinically meaningful increases in the Transitional Dyspnea Index, which has indicated reductions in dyspnea associ- CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 FIGURE 1: RELATIVE GLUCOCORTICOID RECEPTOR AFFINITY OF INTRANASAL CORTICOSTEROIDS MRM 59 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 60 ated with daily activities. Preliminary data suggest that combining tiotropium with LABA and perhaps with ICS may produce additional bronchodilator action in COPD. References 1. Derendorf H, Nave R, Drollmann A, Cerasoli F, Wurst W. Relevance of pharmacokinetics and pharmacodynamics of Clinics of inhaled drugs Aspetti clinici dei farmaci inalatori Fulvio Braido Clinica Malattie Respiratorie e Allergologia, Azienda Ospedaliera Universitaria San Martino di Genova, Genova, Italia Asthma and COPD share some inhaled drugs such as β2-agonists, anticholinergics and inhaled steroids but the rationale for use and the related clinical implications are very different. Although inflammation and bronchoconstriction are present in both diseases, their responsiveness to the available drugs is quite different in the two diseases. Th2 inflammation appears the major pathogenetic feature present in asthma, and consequently represents the essential target of its therapy. The responsiveness of eosinophilic inflammation to inhaled steroid is clinically paralleled by the efficacy of these drugs in preventing asthma exacerbations, in ameliorating symptoms and quality of life. The responsiveness of neutrophilic inflammation, often present in severe asthma, and similar to that present in COPD, is less evident. Therefore the use of inhaled steroids, based on the evidence of trials on clinical efficacy, is currently warranted for the most severe stages of the disease in the presence of frequent exacerbations. More recent data have shown that β2-agonists, besides their bronchodilator activity, may have an anti-inflammatory action of their own that enhances that of inhaled steroids. Unlike in COPD, long acting β2-agonists are not recommended for the long term treatment of asthma when used alone, due to the possibility of serious adverse effects. Anticholinergic drugs present a bronchodilator activity that is more intense in COPD than in asthma; short acting molecules are nowadays available for both diseases, while the long acting one (tiotropium) is presently indicated exclusively for COPD treatment. Asthma and COPD share the principal outcomes of inhaled therapy: symptoms relief, lung function improvement, reduction of exacerbation and mortality, improvement of quality of life. The different pathogenetic clinical features of asthma and COPD shape the different therapeutic schemes feasible with the same drugs in these pathologies. Besides 60 MRM inhaled corticosteroids to asthma. Eur Respir J 2006;28:1042-1050. 2. Op't Holt TB. Inhaled beta agonists. Respir Care 2007;52:820-832. 3 Restrepo RD. Use of inhaled anticholinergic agents in obstructive airway disease. Respir Care 2007;52:833-851. 4. Valotis A, Högger P. Human receptor kinetics and lung tissue retention of the enhanced-affinity glucocorticoid fluticasone furoate. Respir Res 2007;8:54. the use on demand of short acting β2-agonist in mild intermittent asthma and as rescue medication in the other stages of asthma severity, nowadays three therapeutic schemes are suggested. All the fixed combinations available (salmeterol + fluticasone, formoterol + budesonide and formoterol + beclomethasone) may be used on a regular basis twice daily, with different dosages. The best evidence in favour of this treatment approach comes from the GOAL study. This trial has shown that with a long term treatment with fluticasone + salmeterol it is possible to reach the level of control suggested by GINA guidelines in a large percentage of patients, that combination therapy obtains more significant clinical effects than increasing the dose of inhaled steroids alone, that long term treatment is safe and related to an improvement also of the pathogenetic features of asthma and, finally, that the clinical improvement is consistent with the quality of life improvement. The peculiar pharmacokinetic characteristics of formoterol allow the use of its combination with budesonide (and maybe also with beclomethasone, effects under evaluation in ongoing clinical trials) as optional administrations in addition to the regular schedule. This approach, tested in several SMART trials, has shown to be effective on asthma treatment objectives and seems to allow use of a less cumulative dose of steroid. The third treatment approach proposed, verified in mild persistent asthmatic patients in the BEST trial, consists in a symptoms-driven drug administration. Besides the use on demand of short acting bronchodilators in mild COPD, the other stages of severity are treated with incremental doses of the different drugs on a regular basis. Asthma and COPD, besides the similarities in pathogenesis, clinical pattern and responsiveness to the same drugs, must be considered independent entities. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 61 Farmacologia degli antibiotici Federico Pea Institute of Clinical Pharmacology and Toxicology, Department of Experimental and Clinical Pathology and Medicine, University of Udine, Italy Initial inappropriate antibiotic therapy in patients with severe pneumonia may be associated with increased mortalily rate [1]. Of note, appropriate antimicrobial therapy should be based not only on the choice of the antibiotic with the correct spectrum of activity, but also on the right dosing regimen according to three criteria: pharmacokinetic/pharmacodynamic (PK/PD) properties, site of infection and patient's pathophysiology [2]. As far as PK/PD is concerned, several studies have shown that antibiotics may exhibit time-dependent or concentration-dependent antibacterial activity. Beta-lactams, glycopeptides and oxazolidinones are timedependent antimicrobial agents, whose efficacy is mainly related to the time during which concentrations are maintained above the minimal inhibitory concentration (MIC) of the pathogen (t>MIC), with a minimum target for efficacy of t > MIC of 50-60% of the dosing interval [3]. Conversely, aminoglycosides and fluoroquinolones exhibit concentrationdependent antibacterial activity, and this means that peak to MIC ratio (Cmax/MIC) and area under the concentration-time curve to MIC ratio (AUC/MIC) are the most important parameters of efficacy, optimal thresholds being Cmax/MIC ratio of 10-12 and AUC/MIC ratio of 100-125, respectively [4]. On this basis, as a general rule, different schedule regimens must be chosen. The best choice for time-dependent antimicrobials is the multi-refracted regimen, with a total number of daily doses inversely related to the length of the elimination half-life of the drug [2]. Conversely, concentrationdependent antimicrobials may benefit from once daily dosing, this ensuring, under the same total daily dose, the highest Cmax/MIC [2]. However, when treating deep-seated infections, another important issue should be taken into account, considering that drug penetration at the infection site may consistently vary according to the physicochemical properties of the different antibiotics [5]. In the specific case of pneumonia, drug penetration at the infection site may be assessed by measuring drug levels in the epithelial lining fluid (ELF) for extracellular respiratory pathogens (the most frequent bacterial aetiological agents of nosocomial pneumonia), or in alveolar macrophages (AM) for intracellular respiratory pathogens such as Legionella pneumophila (a well known agent of nosocomial pneumonia) [2]. As a general rule, lipophilic compounds (i.e. macrolides, fluoroquinolones, tetracyclines, rifampicin, and oxazolidinones) may have better diffusion in ELF than hydrophilic compounds (i.e. beta-lactams, glycopeptides and aminoglycosides), and are the only agents able to significantly accumulate within AM [2]. Therefore, when using hydrophilic compounds, considering that only a fraction of the drug may diffuse into the ELF from plasma, it is mandatory to apply the most suitable dosing schedule regimen according to the PK/PD principles in order to avoid a significant risk of underexposure in ELF. This aspect may become especially crucial in the critically ill patients with severe sepsis, in whom several pathophysiological situations may add further complexity due to the expansion in the extracellular fluids and/or to an increase of glomerular filtration rate [5,6]. Accordingly, in critically ill patients the best administration schedule for time-dependent antimicrobials should be considered intravenous extended infusion [7] or, even better, continuous infusion [8,9], as suggested by the improved clinical outcomes recently observed in some clinical studies [10-13]. Conversely, for concentration-dependent antibiotics the strategy of high dose short course regimens might be feasible with the intent of achieving more rapid bacterial killing and, if possible, preventing the spread of resistance [14]. An intriguing example comes from a recent clinical study which comparatively assessed the efficacy of levofloxacin 750 mg/24h for 5 days vs. 500 mg/24h for 10 days in the treatment of hospitalized patients with community acquired pneumonia [15]. Although the clinical success rate was similar among the two patient groups, the percentage of patients with resolution of purulent sputum and fever by day 3 of therapy was significantly higher among those who received higher dose short course regimens. Accordingly, it may be speculated that high dosage short course regimens with concentration-dependent antimicrobials might prove to be especially useful in shortening time to resolution of symptoms in seriously ill patients. In conclusion, clinical pharmacology of antibiotics represents a helpful tool for optimization of pneumonia treatment with the intent of both improving clinical outcome and reducing the risk of resistance spread. References 1. Niederman MS. Use of broad-spectrum antimicrobials for the treatment of pneumonia in seriously ill patients: maximizing clinical outcomes and minimizing selection of resistant organisms. Clin Infect Dis 2006;42(Suppl 2):S72S81. 2. Pea F, Viale P. The antimicrobial therapy puzzle: could pharmacokinetic-pharmacodynamic relationships be helpful in CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 Pharmacology of antibiotics MRM 61 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 62 3. 4. 5. 6. 7. 8. 9. addressing the issue of appropriate pneumonia treatment in critically ill patients? Clin Infect Dis 2006;42:1764-1771. Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis 1998;26:1-10. Preston SL, Drusano GL, Berman AL, Fowler CL, Chow AT, Dornseif B, Reichl V, Natarajan J, Wong FA, Corrado M. Levofloxacin population pharmacokinetics and creation of a demographic model for prediction of individual drug clearance in patients with serious community-acquired infection. Antimicrob Agents Chemother 1998;42:10981104. Pea F, Viale P, Furlanut M. Antimicrobial therapy in critically ill patients: a review of pathophysiological conditions responsible for altered disposition and pharmacokinetic variability. Clin Pharmacokinet 2005;44:1009-1034. Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med 2008;34:17-60. Lomaestro BM, Drusano GL. Pharmacodynamic evaluation of extending the administration time of meropenem using a Monte Carlo simulation. Antimicrob Agents Chemother 2005;49:461-463. Mouton JW, Vinks AA. Continuous infusion of beta-lactams. Curr Opin Crit Care 2007;13:598-606. Roberts JA, Lipman J, Blot S, Rello J. Better outcomes 10. 11. 12. 13. 14. 15. through continuous infusion of time-dependent antibiotics to critically ill patients? Curr Opin Crit Care 2008;14:390396. Lodise TP Jr., Patel N, Kwa A, Graves J, Furuno JP, Graffunder E, Lomaestro B, McGregor JC. Predictors of 30day mortality among patients with Pseudomonas aeruginosa bloodstream infections: impact of delayed appropriate antibiotic selection. Antimicrob Agents Chemother 2007;51:3510-3515. Lorente L, Jiménez A, Palmero S, Jiménez JJ, Iribarren JL, Santana M, Martín MM, Mora ML. Comparison of clinical cure rates in adults with ventilator-associated pneumonia treated with intravenous ceftazidime administered by continuous or intermittent infusion: a retrospective, nonrandomized, open-label, historical chart review. Clin Ther 2007;29:2433-2439. Lorente L, Lorenzo L, Martin MM, Jiménez A, Mora ML. Meropenem by continuous versus intermittent infusion in ventilator-associated pneumonia due to gram-negative bacilli. Ann Pharmacother 2006;40:219-223. Rello J, Sole-Violan J, Sa-Borges M, Garnacho-Montero J, Muñoz E, Sirgo G, Olona M, Diaz E. Pneumonia caused by oxacillin-resistant Staphylococcus aureus treated with glycopeptides. Crit Care Med 2005;33:1983-1987. Grossman RF, Rotschafer JC, Tan JS. Antimicrobial treatment of lower respiratory tract infections in the hospital setting. Am J Med 2005;118(Suppl 7A):29S-38S. Shorr AF, Khashab MM, Xiang JX, Tennenberg AM, Kahn JB. Levofloxacin 750-mg for 5 days for the treatment of hospitalized Fine Risk Class III/IV community-acquired pneumonia patients. Respir Med 2006;100:2129-2136. Clinical aspects of antibiotic therapy in respiratory tract infections Aspetti clinici della terapia antibiotica nelle infezioni del tratto respiratorio Pierluigi Viale Clinic of Infectious Diseases, University of Udine, Udine, Italy In the context of respiratory tract infections, pneumonia represents the field in which an appropriate antibiotic therapy is of the highest clinical relevance. The term “pneumonia” encompasses a wide spectrum of diseases, with huge differences in clinical presentation, grading of severity, mortality, microbiological agents and chemosensitivity pattern. When depicting antibiotic use in pneumonia, the minimum classification required is communityacquired vs. health-care associated pneumonia, and within the latter ventilator-associated pneumonia. Additionally, all decisions on drug choice and dosage in any kind of infection (pneumonia included) must be guided by careful assessment of clinical severity. In fact, the present and future of antibiotic therapy is characterized by patient-tailored treatment as opposed to disease- or microorganismtailored decisions [1]. To optimally define the principles of antimicrobial choice, it is therefore mandatory to combine information on grading of clinical severity, setting and, for nosocomial pneumonia, timing of onset calculated from hospital admission (or from start of mechanical ventilation). 62 MRM In the field of community-acquired pneumonia (CAP), clinical research on outcome predictive factors has undergone tremendous development. Also the most recent Guidelines of the Infectious Diseases Society of America and the American Thoracic Society recommend a routine use of the two most reliable prognostic indexes (Pneumonia Severity Index and CURB-65) to assess the grade of severity of pneumonia, and assign to this mode of assessment a key role in clinical decisions, even more important than that assigned to microbiological diagnosis [2]. It is likely that in the near future additional scales will be employed in clinical practice, such as the SCAP score [3], and that different systems for clinical severity assessment will be employed in different clinical-epidemiological settings, with definition of additional risk factors and better weighting of comorbidities. Clinical severity scores, obviously, do not replace clinical judgement but are highly useful mainly as early warning tools for severe forms or as useful criteria to define which patients might be managed on an out-patient basis. Briefly, it is nowadays possible to classify CAP MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 63 72 hours from hospital/ICU admission), late VAP (onset more than 10 days after hospital/ICU admission) and intermediate VAP (occurring between 4 and 10 days of hospital/ICU stay) [4]. In the first setting, antibiotic therapy will be the same as in severe CAP. In intermediate VAP the antimicrobial spectrum will need to include the microorganisms colonizing the gastroenteric tract (besides taking into account any outbreak occurring at the time the patient's stay). In late VAP the therapy shall be chosen keeping in mind that the patient's flora is completely subverted into nosocomial flora. Therefore, in early VAP, S. pneumoniae and methicillin-sensitive S. aureus are the treatment target; in intermediate VAP Legionella spp and Enterobacteriaceae should be included, while in late VAP the antimicrobial spectrum should include P. aeruginosa, methicillin-resistant S. aureus, and ESBL-producing Enterobacteriaceae. References 1. Pea F, Viale P. The antimicrobial therapy puzzle: could pharmacokinetic-pharmacodynamic relationships be helpful in addressing the issue of appropriate pneumonia treatment in critically ill patients? Clin Infect Dis 2006;42:1764-1771 2. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44 (Suppl 2):S27-S72. 3. España PP, Capelastegui A, Gorordo I, Esteban C, Oribe M, Ortega M, Bilbao A, Quintana JM. Development and validation of a clinical prediction rule for severe communityacquired pneumonia. Am J Respir Crit Care Med 2006;174:1249-1256. 4. American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcareassociated pneumonia. Am J Respir Crit Care Med 2005;171:388-416. Clinical implications of pharmacologic evidence: inflammation Conseguenze cliniche delle evidenze farmacologiche: l'infiammazione Fulvio Braido Clinica Malattie Respiratorie e Allergologia, Azienda Ospedaliera Universitaria San Martino di Genova, Genova, Italia Asthma and rhinitis, on the one hand, and COPD on the other have found in inflammation an important pathogenetic factor but the clinical implications of its treatment seem different in the different pathologies. Th2 inflammation is the major pathophysiological feature in asthma and allergic rhinitis, and this is the reason for a combined treatment of them. The immunopathological relationship between allergic rhinitis and asthma has been amply demonstrated and we have much evidence about the effects of rhinitis treatment on asthma outcomes. In both diseases, the international guidelines identify inhaled steroids as the fundamental drug for the long term management of persistent cases. Obviously, it seems essential to establish a therapeutic plan that allows the achievement of the best results in terms of function, symptoms and quality of life without CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 into three categories: - Mild CAP of the young adult, where a simple and low-cost strategy can be applied, i.e. monotherapy on an out-patient basis; - Mild CAP of the elderly patient with or without comorbidities, where a short hospital admission and combination antibiotic therapy is suggested, with early switch to monotherapy; - Severe CAP, where intensivist assessment, microbiological diagnosis and de-escalation antibiotic treatment approach are pivotal, particularly if the patient presents any risk factor for multidrugresistant microorganisms. Similar principles can be applied in the choice of antimicrobial therapy for health-care associated pneumonia not associated to mechanical ventilation. The main difference with CAP is represented by the microbiological ecosystem, much more complex in the hospital setting or in other healthcare facilities such as long-term facilities. Therefore, it is necessary to consider, besides clinical-epidemiological grading, also up-to-date information on the current microbial ecosystem in the hospital/ward where the patient is admitted, particularly the chemosensitivity pattern. On the other hand, the therapeutic approach to ventilator-associated pneumonia (VAP) is completely different: in this field no clinical severity grading applies but on the contrary these infections represent the archetype of life-threatening infections. In this field the role of microbiological diagnosis is pivotal. Pending culture results, the most relevant criteria to define treatment choice in the calculated therapy are the time between ICU (or hospital) admission and VAP onset, and the microbial ecosystem of the ICU itself. The first element is useful to assess which microorganisms are more likely causing the infection, the latter to define the probable chemiosensitivity pattern to be covered. With respect to timing of onset, three clinical settings apply, with different microbiological (and consequently therapeutic) priorities: early VAP (within MRM 63 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 64 exceeding the recommended daily dose of bronchial and nasal steroid. In this sense, a treatment schedule that considers antihistamines and antileukotrienes could be useful. Although the clinical effects of the available drugs is clearly demonstrated, their potential role in preventing the disease evolution needs to be further clarified. Fibroblast plays an important role in airways remodelling. Baouz et al. demonstrated the pharmacological response of lung myofibroblasts to β2-agonist combined with inhaled steroids, represented in vitro by an anti-inflammatory/anti-contractile effect [1]. Descalzi et al. showed an enhanced anti-remodelling activity in vitro due to beclomethasone plus formoterol/albuterol in bronchial fibroblast, providing new insight on the additive effects of inhaled corticosteroid and β2-agonist for asthma therapy [2]. The efficacy in asthma patients of these drugrelated effects needs to be investigated and it appears crucial in defining the feasibility of an “on demand” asthma treatment. While the responsiveness of eosinophilic inflammation to steroid is undeniable, the responsiveness of neutrophilic inflammation, often present in severe asthma and typically present in COPD, does not appear so obvious. A recent meta-analysis seems to show that their use in COPD could be attentively evaluated in a risk/benefit study [3]. References 1. Baouz S, Giron-Michel J, Azzarone B, Giuliani M, Cagnoni F, Olsson S, Testi R, Gabbiani G, Canonica GW. Lung myofibroblasts as targets of salmeterol and fluticasone propionate: inhibition of alpha-SMA and NF-kappaB. Int Immunol 2005;17:1473-1481. 2. Descalzi D, Folli C, Nicolini G, Riccio AM, Gamalero C, Scordamaglia F, Canonica GW. Anti-proliferative and antiremodelling effect of beclomethasone dipropionate, formoterol and salbutamol alone or in combination in primary human bronchial fibroblasts. Allergy 2008;63:432-437. 3. Yang IA, Fong KM, Sim EH, Black PN, Lasserson TJ. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2007;2:CD002991. Clinical implications of pharmacologic evidence: management approach to infection Conseguenze cliniche delle evidenze farmacologiche: approccio al trattamento delle infezioni Lucio Casali, Valentina Malafoglia Università degli Studi di Perugia, Azienda ospedaliera Santa Maria, Terni, Italia The diseases of the upper respiratory tract are often neglected in the attention of physicians both in childhood and adulthood. Infections represent the most frequent origin and a correct attention must be given to the clinical framework, to the diagnosis and decisional consequences regarding the therapeutic choices. Upper respiratory tract infections (URTIs) represent, in fact, the most common acute illness in the general population and account for most of the diagnoses made in the outpatient setting in many parts of the world [1]. Viruses are probably the most prominent cause of URTIs but physicians must be able to recognize the distinctive signs and symptoms of bacterial infections so as to avoid, or at least limit, the potential complications through an effective treatment. Viruses such as rhinovirus, adenovirus and parainfluenza virus are frequently reported as the source of URTIs [2]; however, even in specialized laboratories it is not always possible to give an established diagnosis. In a young and selected population like that of athletes the pathogens commonly associated with common cold symphtoms are rhinovirus (1040% of cases), corona virus (20%) and respiratory syncytial virus (10%) [3]; influenza parainfluenza viruses and adenoviruses are less frequently causes 64 MRM of these illnesses in this category of patients. Usually viral URTIs are considered benign and self limiting diseases lasting 5-14 days on average, with typical symptoms such as rhinorrea, cough and fever. However, even the common cold can bring more serious complications: acute bacterial sinusitis develops in about 2.5% of adults [4] and a consequent infection involving the lower respiratory tract is not uncommon [5]. These possibilities must be taken into account when weighing up the few findings gathered from physical examination against the discomfort of the patients. In this light risk factors like young age, birth weight, comorbidities, immunodeficiency disorders, malnutrition and crowding must be carefully taken into account [6]. The treatment options are not numerous since antibiotics are not indicated in uncomplicated forms and an antiviral therapy has yet to prove real efficacy. A symptomatic treatment with a decongestant topically administered or with non steroid antiinflammatory drugs is generally recommended. Sinusitis Sinusitis is one of the most common illnesses in the general population. It is defined as “inflammation MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 65 concluded that this drug could be a suitable alternative to the recent fluoroquinolones for the treatment of acute sinusitis. A recent meta-analysis comparing the role and the effect of fluoroquinolones with beta-lactam antibiotics in the treatment of acute sinusitis [14] concluded that respiratory fluoroquinolones were comparable to beta-lactams for the treatment of acute bacterial sinusitis, a condition usually with a benign clinical course. The primary use of fluoroquinolones may be considered in cases where betalactam treatment has failed and when drug-resistant pathogens are suspected as playing a possible or probable role. Therefore, the most recent guidelines of the American Accademy of Otolaryngology-Head and Neck Surgery (AAO-HNS) [15] state that when selecting an antibiotic for acute sinusitis it is important to consider some factors that could modify the choice of initial antibiotic therapy: • local resistance patterns, with about 15% of S. pneumoniae having intermediate penicillin resistance and 25% high resistance • amoxicillin is ineffective against beta-lactamaseproducing M. catarrhalis and H. influenzae • recent use of antibiotics is an important risk factor for the presence of antibiotic-resistant bacteria Following these points the same guidelines recommend that the optimal therapy should include high dose amoxicillin-clavulanate (4 g per day amoxicillin equivalent) or a respiratory quinolone (levofloxacin, moxifloxacin, gemifloxacin). Moreover the pharmacokinetic features of the recent fluoroquinolones and their pharmacodynamic effects in terms of their clinical efficacy and penetration power [16] into the mucosa of the target make these drugs optimal in overcoming the problems of resistance, and shortening the clinical course of disease with a better quality of life for the patients. Another non negligible resource is prevention of exacerbation through the resort to vaccination against influenza and pneumococcal infection [17]. In conclusion, to limit the role of these conditions clinicians must accurately evaluate the role of these diseases and their important consequences. References 1. Woodwell DA, Cherry DK. National Ambulatory Medical Care Survey: 2002 summary. Adv Data 2004;346:1-44. 2. Barrett B, Locken K, Maberry R, Schwamman J, Brown R, Bobula J, Stauffacher EA. The Wisconsin Upper Respiratory Symptom Survey (WURSS): a new research instrument for assessing the common cold. J Fam Pract 2002;51:265. 3. Nieman DC. Current perspective on exercise immunology. Curr Sports Med Rep 2003;2:239-242. 4. Gwaltney JM Jr, Hendley JO. Transmission of experimental rhinovirus infection by contaminated surfaces. Am J Epidemiol 1982;116:828-833. 5. Puhakka T, Mäkelä MJ, Alanen A, Kallio T, Korsoff L, Arstila P, Leinonen M, Pulkkinen M, Suonpää J, Mertsola J, Ruuskanen O. Sinusitis in the common cold. J Allergy Clin Immunol 1998;102;403-408. CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 of one or more of the paranasal sinuses” and is categorized on the basis of its duration as acute (< 4 weeks), subacute (4-8 weeks) or chronic (> 8 weeks) [7]. The cause of sinusitis can be viral (mainly for the acute type) or bacterial (acute, subacute and chronic forms). Viral infection is the most common cause and usually resolves in 7-10 days, while acute bacterial sinusitis, although self-limiting, can resolve without treatment after one month in 75% of cases [7]. However, when untreated, sinusitis can provoke complications both intracranial and in the lower respiratory tract. The viral agents generally are not different from those mentioned above, while the bacterial pathogens most commonly present are: Streptococcus pneumoniae, Haemophilus influenzae and, to a lesser degree, Moraxella catarrhalis [810]. Antibiotic treatment is recommended to shorten the duration of the infection and associated symptoms (so allowing the patient to resume daily activities) as well as to decrease mucosal damage and prevent the risk of suppurative complications [11]. The persistence of an infective sinusitis might be seen as a threat for a potential diffusion of the infection to the bronchial tree and, when the local host defence mechanisms are impaired, also to the lung tissue. Part of the infective load can escape the swallowing processes and can be inhaled, particularly during sleep. The presence of some comorbidities like COPD, diabetes, GERD or the simple coexistence of an acute bronchitis or of damage to the mucociliary clearance process, as occurs in smokers or in subjects who breathe heavily polluted air, can make these individuals prone to an extension of the original infection to the bronchial tree and lungs. On the other hand, the bacterial flora commonly present in sinusitis can be detected also in the infections of the lower respiratory tract. These situations can be seen as true causes of exacerbation in COPD with important sequelae on the pulmonary function [12] which can determine the progressive trend especially in those with advanced disease. When a viral etiology is present one can expect possible exacerbations in the course of asthma. According to the above considerations, the treatment of sinusitis must be seen as of primary importance in order to overcome the infection at the site of its initial location and limit or totally prevent its extension to other proximal or distant areas. The main, but no longer recent, guidelines recommend 10-14 days of therapy with high doses of amoxicillin, amoxicillin-clavulanate, cefdinir, cefuroxime, a macrolide or a new fluoroquinolone (9). Beta-lactams are indicated for initial antimicrobial therapy in adults with mild disease who have not received antimicrobials within the past 4-6 weeks. The use of a “respiratory” fluoroquinolone such as levofloxacin is recommended for patients with a mild or moderate infection or recent antimicrobial exposure. In a comparative study [13] cefdinir, an extended spectrum cephalosporin, proved to be as effective as levofloxacin and the authors MRM 65 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 66 6. Teichtahl H, Buckmaster N, Pertnikovs E. The incidence of respiratory tract infection in adults requiring hospitalization for asthma. Chest 1997;112:591-596. 7. CDC Centers for Disease Control and Prevention. Non specific upper respiratory tract infection. 2006. Available at: http://www.cdc.gov/drugresistance/community/hcp-infosheets/adult-nurti.htm 8. Gwaltney JM Jr, Scheld WM, Sande MA, Sydnor A. The microbial etiology and antimicrobial therapy of adults with acute community-acquired sinusitis: a fifteen-year experience at the University of Virginia and review of other selected studies. J Allergy Clin Immunol 1992;90:457-461. 9. Anon JB, Jacobs MR, Poole MD, Ambrose PG, Benninger MS, Hadley JA, Craig WA; Sinus And Allergy Health Partnership. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg 2004;130(Suppl 1):1-45. 10. Jacobs MR, Felmingham D, Appelbaum PC, Grüneberg RN; The Alexander Project Group. The Alexander Project 19982000: susceptibility of pathogens isolated from communityacquired respiratory tract infection to commonly used antimicrobial agents. J Antimicrob Chemoter 2003;52:229-246. 11. Dagan R, Klugman KP, Craig WA, Baquero F. Evidence to support the rationale that bacterial eradication in respiratory 12. 13. 14. 15. 16. 17. tract infection is an important aim of antimicrobial therapy. J Antimicrob Chemother 2001;47:129-140. Bhowmik A, Seemungal TA, Sapsford RJ, Wedzicha JA. Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations. Thorax 2000;55:114-120. Henry DC, Kapral D, Busman TA, Paris MM. Cefdinir versus levofloxacin in patients with acute rhinosinusitis of presumed bacterial etiology: a multicenter, randomized, double-blind study. Clin Ther 2004;26:2026-2033. Karageorgopoulos DE, Giannopoulou KP, Grammatikos AP, Dimopoulos G, Falagas ME. Fluoroquinolones compared with beta-lactam antibiotics for the treatment of acute bacterial sinusitis: a meta-analysis of randomized controlled trials. CMAJ 2008;178:845-854. Rosenfeld RM. Clinical practice guidelines on adult sinusitis. Otolaryngol Head Neck Surg 2007;137:365-377. Pea F, Marioni G, Pavan F, Staffieri C, Bottin R, Staffieri A, Furlanut M. Penetration of levofloxacin into paranasal sinuses mucosa of patients with chronic rhinosinusitis after a single 500 mg oral dose. Pharmacol Res 2007;55:38-41. Burge PS. Prevention of exacerbations: how are we doing and can we do better? Proc Am Thorac Soc 2006;3: 257-261. Pathogenetic and clinical framework of rhinosinusal disease Inquadramento patogenetico e clinico nella patologia rinosinusale Luisa Bellussi Istituto di Discipline ORL, Università degli Studi di Siena, Siena, Italia The correlation between upper airways disease (rhinitis, sinusitis) and asthma is a known fact and it has always been interpreted according to two opposed perspectives: on the one hand, upper respiratory tract infections and asthma are considered as distinct nosological entities, the former being regarded as a risk factor for the development of bronchial hyperresponsiveness; on the other hand, rhinitis, sinusitis and asthma are considered as expressions of the same pathological process that involves the whole respiratory system, but with a temporal sequencing that can mask their close aetiopathogenetic interdependence. This fundamental difficulty of nosological classification has delayed the possibility of establishing a specific diagnostic-therapeutic approach for patients with upper and lower airways inflammation. The greatest problem is the clinical heterogeneity of rhinitis, sinusitis and asthma, which impedes reaching a wide consensus on their classification. While asthma is classified as extrinsic or intrinsic based on the existence or not of an IgE-mediated mechanism underlying the inflammation, the classification of rhinitis into its different forms is considerably more complex and far from an aetiologic definition: rhinitis can be infectious (viral or bacterial), allergic (or vasomotor-specific) or non-allergic non-infectious (vasomotor aspecific, or non-allergic noninfectious perennial rhinitis, NANIPER). This latter 66 MRM category risks being a sort of 'deposit' for all the forms of nasal hyperreactivity whose aetiology cannot be identifed. It is known, moreover, that due to the effect of “priming” allergic inflammation not only predisposes to new sensitization, but renders the respiratory mucosa more sensitive to any sort of stimulus, whether physical, chemical or biological with overlapping histopatologic, symptomatologic and clinical pictures. It is for this reason that the aetiologic diagnosis of rhinitis needs to follow a carefully planned diagnostic path that involves first of all an accurate patient's personal and family history, paying special attention to the environment in which the patient lives and works, then an objective examination by means, if possible, of endoscopy so as to be able to inspect the middle meatus into which the openings of the frontal paranasal sinuses converge, the upper meatus and olfactory fissure, the choanal region, the rhinopharynx and lump of adenoid tissue, the opening of the Eustachian tube. If combined with instrumental examinations such as rhinomanometry performed at baseline conditions and after pharmacological decongestion of the nasal mucosa, endoscopy can by itself orient the diagnosis on an anatomico-structural basis toward disreactive forms, which are difficult to resolve with medical therapy alone. While allergometric skin tests represent the first step in rhinoallergological diagnosis, in the case of a negative MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 67 dysfunction caused by allergic inflammation is simply the starting point of the sinusal pathological cycle that leads, if not treated, to acute, recurrent and chronic bacterial infection. In rhinosinusitis the real issue, in fact, is: for the acute forms, to identify through clinical and endoscopic examination the most appropriate moment in which to begin antibiotic treatment and establish its duration; and for the recurrent and chronic forms, to search for factors predisposing to infection. In any case, it is good always to remember that the link between the upper and lower airways is not solely a matter of their continuity or contiguity but of their strict functional interdependence: a congested nose through which it is difficult to breathe properly, or an inflamed or infected nasosinusal mucosa will never be able to explicate adequately the functions of warming, humidifying, filtering and purifying of the air we breathe - functions that are essential - before it passes into the lower airways. References 1. Mygind N, Dahl R, eds. The nose and paranasal sinuses in asthma. Allergy 1999;54:(Suppl. 57). 2. Bousquet J, Van Cauwenberge P, Khaltaev N; Aria Workshop Group; World Health Organization. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol 2001;108 (Suppl 5):S147-S334. 3. Fokkens WJ. Thoughts on the pathophysiology of non allergic rhinitis. Curr Allergy Asthma Rep 2002;2:203-209. 4. Fokkens WJ, Lund V, Mullol J. EPOS 2007. European position paper on rhinosinusitis and nasal polyps 2007. A summary for otorhinolaryngologists. Rhinology 2007;45: 97-101. Links between allergic rhinitis and asthma I legami tra asma e rinite allergica Attilio Boner Department of Mother Child and Biology-Genetics, Department of Pediatrics, Università di Verona, Verona, Italy Allergic rhinitis is the most common of atopic disorders, affecting 10-30% of the adult population, with higher peaks of prevalence in childhood [1]. The development of allergic rhinitis is affected by familial and environmental factors; about 70% of allergic children show a family history of atopic disorders. Although allergic rhinitis is frequently regarded as a nuisance illness, several studies have demonstrated that the bothersome nature of symptoms (rhinorrhea, nasal congestion and sneezing) impairs the usual performance of daily activities, quality of sleep, cognitive function, and work productivity. It has also been reported that severity, more than the persistence of symptoms, is the factor most affecting quality of life [2]. In this context, a recent case-control investigation on a population of 1,834 students (aged 15-17 years; 50% girls) showed that allergic rhinitis adversely impacts school performance: young people with reported symptoms on an examination day were, compared to their fellow students without symptoms, 40% more likely to drop a grade in summer examinations, and 70% more likely to drop a grade if they reported taking sedating antihistamines at the time of their examination [3]. The relationship between allergic rhinitis and poor school performance was specific and related to the severity of symptoms: students who reported a history of allergic rhinitis in previous years and who had a symptom score on any examination day of > 2 (on a 10-point Likert scale) were more than twice as likely to drop a grade. Complications of allergic rhinitis and concomitant diseases are well documented, such as acute and chronic sinusitis, nasal polyps, otitis media/otitis CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 response it is good to follow these up with a specific nasal provocation test, which can reveal an organ allergy that may be considered as a predisposing factor to bronchial hyperreactivity or the first step on the allergic road to asthma and to the involvement of the entire respiratory system. This test, which has a high sensitivity but low specificity, can be made more reliable by dosing some mediators of the allergic reaction into the secretions. Nasal cytology, although easy to carry out, is limited by difficulties in its interpretation due to the lack of standardization. Even NARES (non allergic rhinitis with eosinophils), the form that seems the easiest of all the aspecific vasomotor rhinitis forms to classify on account of its specific cellular pattern, needs in realty to be investigated with care: no precise cut-off, in fact, exists for defining eosinophilia, and a positive cytological examination in the presence of negative allergometric skin tests is not sufficient to exclude organ sensitization or an underlying error in the chosen panel of allergens tested. Hence the need for a reasoned interpretation of all the diagnostic means available, because while it is true that the therapeutic efficacy of the available pharmacological drugs has to rely on evidencebased criteria, it is equally true that this is strictly correlated to a correct diagnostic definition. Clinical research has shown that sinusitis is synonymous with rhinosinusitis: it seems limiting, nevertheless, to classify sinusitis as intermittent or persistent according to the intensity and duration of symptoms, by analogy with the classification proposed by the document ARIA for a reasoned approach to the treatment of allergic rhinitis. The ostiomeatal MRM 67 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 68 68 MRM media with effusion, hearing impairment, abnormal craniofacial development, sleep apnea, aggravation of underlying asthma and increased propensity to develop asthma. In particular, evidence shows that rhinitis and asthma are intimately linked: up to 81% of subjects with asthma report symptoms of rhinitis. Conversely, the risk of asthma increases from 2% in subjects without rhinitis to 6.7-18.8% in subjects with allergic rhinitis [4]. As regards the temporal sequence of this association, follow-up studies in adults have shown that allergic rhinitis might precede asthma [5]. In addition, data from a longitudinal investigation on a large population-based cohort followed over a 37year period suggest that childhood allergic rhinitis was associated with a significant 2- to 7-fold increased risk of incident asthma in preadolescence, adolescence, or adult life as well as with a 3-fold increased risk of childhood asthma persisting compared with remitting by middle age [6]. Thus, allergic rhinitis in childhood seems to be a predictor of both incidence and persistence of asthma in adult age. The close association between rhinitis and asthma is supported not only by epidemiological data but also by similar underlying pathogenesis and immunologic mechanisms. In fact, both diseases are expressions of an inflammatory IgE-mediated process within a continuous airway system. In bronchial biopsies from patients with allergic rhinitis an increased number of inflammatory cells, including eosinophils, has been reported [7]. Furthermore, many patients with allergic rhinitis and no clinical evidence of asthma showed an increased bronchial response to methacholine, attenuated by the treatment with intranasal corticosteroids [8]. Thus, bronchial eosinophilia and hyperresponsiveness, pathologic features characterising asthma, may also be observed in allergic rhinitis. Presumably, the inflammation present in the upper airways might contribute to the inflammation in the lower airways, either directly through aspiration of nasal inflammatory secretions (postnasal drip) or through the absorption of inflammatory mediators in the systemic circulation. Most recent data point to a circulatory pathway, involving bloodstream and bone marrow, as a major mode of nasobronchial cross-talk [9,10]. Interestingly, a number of trials have reported that intranasal treatment of allergic rhinitis resulted in amelioration of asthma symptoms, reduction of bronchial responsiveness and improvement in lung function [11], supporting the hypothesis that allergic rhinitis may also be a risk factor for increased asthma morbidity. The goal of therapy is to provide an effective control of symptoms, thereby improving quality of life and minimizing the risk of complications. Avoiding or reducing the exposure to triggers, such as allergens, viral infections, pollutants and drugs, should be the first line of defence, to implement whenever possible. As far as pharmacotherapy is concerned, intranasal corticosteroids are recognized as the most effective medications. They have proven to be effective in reducing nasal blockage, rhinorrhea, sneezing, and nasal itch in adults and children. In comparative trials they have been more effective in controlling symptoms of AR than oral or intranasal H1-antihistamines, intranasal cromoglycate, oral antileukotrienes and the association between oral antileukotrienes and oral antihistamines [12,13]. The potent effect of intranasal corticosteroids on nasal blockage and the extensive anti-inflammatory properties favour them above other treatments, especially when nasal obstruction is the major symptom and when disease is long-lasting. References 1. Marinho S, Simpson A, Söderström L, Woodcock A, Ahlstedt S, Custovic A. Quantification of atopy and the probability of rhinitis in preschool children: a populationbased birth cohort study. Allergy 2007;62:1379-1386. 2. Bousquet J, Neukirch F, Bousquet PJ, Gehano P, Klossek JM, Le Gal M, Allaf B. Severity and impairment of allergic rhinitis in patients consulting in primary care. J Allergy Clin Immunol 2006;117:158-162. 3. Walker S, Khan-Wasti S, Fletcher M, Cullinan P, Harris J, Sheikh A. Seasonal allergic rhinitis is associated with a detrimental effect on examination performance in United Kingdom teenagers: case-control study. J Allergy Clin Immunol 2007;120:381-387. 4. van Cauwenberge P, Watelet JB, Van Zele T, Wang DY, Toskala E, Durham S, Fokkens W, Lau S, Leynaert B, Wickman M, Salapatas M, Burney P, Mullol J; GA2LEN workpackages 3.2 and 3.3. Does rhinitis lead to asthma? Rhinology 2007;45:112-121. 5. Settipane RJ, Hagy GW, Settipane GA. Long-term risk factors for developing asthma and allergic rhinitis: a 23-year follow-up study of college students. Allergy Proc 1994;15:21-25. 6. Burgess JA, Walters EH, Byrnes GB, Matheson MC, Jenkins MA, Wharton CL, Johns DP, Abramson MJ, Hopper JL, Dharmage SC. Childhood allergic rhinitis predicts asthma incidence and persistence to middle age: a longitudinal study. J Allergy Clin Immunol 2007;120:863-869. 7. Brown JL, Behndig AF, Sekerel BE, Pourazar J, Blomberg A, Kelly FJ, Sandström T, Frew AJ, Wilson SJ. Lower airways inflammation in allergic rhinitics: a comparison with asthmatics and normal controls. Clin Exp Allergy 2007;37:688-695. 8. Shaaban R, Zureik M, Soussan D, Antó JM, Heinrich J, Janson C, Künzli N, Sunyer J, Wjst M, Burney PG, Neukirch F, Leynaert B. Allergic rhinitis and onset of bronchial hyperresponsiveness: a population-based study. Am J Respir Crit Care Med 2007;176:659-666. 9. Wang Y, McCusker CT. Interleukin-13-dependent bronchial hyper-responsiveness following isolated upper-airway allergen challenge in a murine model of allergic rhinitis and asthma. Clin Exp Allergy 2005;35:1104-1111. 10. Braunstahl GJ, Fokkens W. Nasal involvement in allergic asthma. Allergy 2003;58:1235-1243. 11. Halpern MT, Schmier JK, Richner R, Guo C, Togias A. Allergic rhinitis: a potential cause of increased asthma medication use, costs, and morbidity. J Asthma 2004;41:117126. 12. van Cauwenberge P, Van Hoecke H, Vandenbulcke L, Van Zele T, Bachert C. Glucocorticosteroids in allergic inflammation: clinical benefits in allergic rhinitis, rhinosinusitis, and otitis media. Immunol Allergy Clin North Am 2005;25:489-509. 13. Rodrigo GJ, Yañez A. The role of antileukotriene therapy in seasonal allergic rhinitis: a systematic review of randomized trials. Ann Allergy Asthma Immunol 2006;96:779-786. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 69 Terapia medica della rinite allergica e della rinosinusite Michele de Benedetto UOC di Otorinolaringoiatria, AO “V.Fazzi”, Lecce, Italia Patients affected by a rhinosinusal disease usually report to the doctor because they have a blocked nose, often with an almost continuous anterior and/or posterior rhinorrhea, sneezing, sometimes also pruritus. Behind these symptoms lie different pathogenetic pictures as the cause: acute or exacerbated chronic rhinosinusitis, allergic rhinitis, vasomotor rhinitis (with its multiple forms), rhinitis medicamentosa, and nasal polyposis. In allergic rhinitis, the aim of medical treatment is to reduce symptoms, without interferring with the patient's daily activities and cognitive performance, as well as to prevent complications (asthma and rhinosinusitis). The three most important classes of drugs used in medical therapy of allergic rhinitis are: antihistamines, intranasal corticosteroids, and antileukotrienes. According to EAACI (European Academy of Allergy and Clinical Immunology) and ARIA (Allergic Rhinitis and its Impact on Asthma), oral antihistamines should have as part of their pharmacological characteristics: i) a potent and selective antagonist action on H1 receptors; ii) no significant pharmacokinetic interference with food, other drugs or intestinal transport proteins; iii) no interaction with the cytochrome PA503A (CYP3A). In terms of efficacy, they should be active in treating intermittent or persistent allergic rhinitis and capable of improving all nasal symptoms, including obstruction. Regarding side effects, they should have no sedative effects or provoke any cognitive or psychomotor alteration, no anticholinergic effects, no cardiological effects, and they should be able to be used during pregnancy and breast-feeding. The advent of intranasal corticosteroids in 1974 represents the most significant innovation that has taken place in the treatment of rhinosinusal diseases as a whole, above all allergic rhinitis. Today they are considered the first choice of treatment for moderate-severe allergic rhinitis or those forms in which nasal obstruction is the predominant symptom. Intranasal corticosteroids inhibit the start of the inflammatory response, reducing the permeability of the nasal mucosa, the number of inflammatory cells and, as a consequence, the release of their chemical mediators. We have now arrived at the third generation of this class of drugs, with a gradual reduction of their systemic bio-availability from values of around 40% for beclometasone and triamcinolone to 11% for budesonide and right down to 0.5% for fluticasone furoate, which at the present moment has the highest receptor affinity for glucocorticoids and, for this reason, has practically no side effect on the hypothalamic-hypophyseal system. Due to these characteristics, the FDA has authorized their use in the USA in infants 3 years of age and upwards. Antileukotrienes are another class of drugs that are proving of particular interest in the treatment of allergic rhinitis. By blocking the action of leukotrienes in the allergic cascade, they improve symptoms, especially in terms of reducing the nasal obstruction. Rhinosinusitis is a phlogistic-infective process of multifactorial origin that simultaneously affects the mucosa lining the nasal and paranasal cavities, and develops in response to any factor whatsoever that determines obstruction of the ostiomeatal complex. Different types of rhinosinusitis exist according to the time course, with different symptomatologic features. These go from acute rhinosinusitis, that presents with a maximum duration of 6 weeks or up to 4 recurrent episodes in a year lasting at least 10 days and is resolved with medical therapy, to exacerbated chronic rhinosinusitis that has a longer duration of up to 8 weeks with more than 4 recurrent episodes in a year lasting more than 10 days. This latter form is often not resolvable with medical therapy alone since - as CT scan shows - there is a hyperplasia of the mucosa of the ostio-meatal complex and paranasal sinuses. Both the acute and chronic forms are differentiated as recurrent or refractory, depending on whether the aetiological agents are different (recurrent) or the same (refractory). The germs most frequently causing acute bacterial rhinosinusitis are Streptococcus pneumoniae together with Haemophilus influenzae and Moraxella catarrhalis, while those that cause the chronic form are, besides S. pneumoniae, Staphylococcus aureus, Pseudomonas aeruginosa, some Bacteroides and Fusobacterium. Objective examination of the nose with flexible or rigid fiberoptic endoscope is, alone, resolutive for a correct diagnosis, while imaging diagnostics (CT or NMR) have only a confirmatory role in the clinical diagnosis and are useful for the investigation of eventual complications. Medical therapy of rhinosinusitis includes also: • nasal lavage, preferably with isotonic solution, for a constant cleansing of the mucosa; • intranasal corticosteroids, for their antiinflammatory action; • mucolytics and/or mucoregulators, to restore the protective mucus layer of the epithelial lining. A systemic corticosteroid can provide valuable support to the action of the antibiotic therapy. Considering the bacterial strains most frequently detected as the cause of rhinosinusitis and their resistance to the various antibiotic classes, the molecules recommended by the Guidelines of the American Academy of ORL are: last generation quinolones and protected amoxicillin, but at high doses (3gr/die). References CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 Medical treatment of allergic rhinitis and rhinosinusitis 1. Fokkens WJ, Lund V, Mullol J. EPOS 2007. European position paper on rhinosinusitis and nasal polyps 2007. A summary MRM 69 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 70 70 MRM for otorhinolaryngologists. Rhinology 2007;45:97-101. 2. ARIA: Allergic Rhinitis and its Impact on Asthma. Workshop report. 2001. 3. Malling HJ, Abreu-Nogueira J, Alvarez-Cuesta E, Björkstén B, Bousquet J, Caillot D, Canonica GW, Passalacqua G, Saxonis-Papageorgiou P, Valovirta E. Local immunotherapy. Allergy 1998;53:933-944. 4. van Cauwenberge P, Bachert C, Passalacqua G, Bousquet J, Canonica GW, Durham SR, Fokkens WJ, Howarth PH, Lund V, Malling HJ, Mygind N, Passali D, Scadding GK, Wang DY. Consensus statement on the treatment of allergic rhinitis. European Academy of Allergology and Clinical Immunology. Allergy 2000;55:116-134. Acute exacerbations of COPD Riacutizzazioni della BPCO Gianni Balzano Pneumology Unit, Salvatore Maugeri Foundation, Scientific Institute of Telese, Telese Terme (BN), Italy Acute exacerbations (AEs) of baseline symptoms dyspnea, cough, and/or sputum - are frequently associated with the natural course of COPD and may require an increase in the baseline, regular treatment of the patient [1]. Severity, time course, and recovery of an AE of COPD vary widely [2], and patients' symptoms, lung function, quality of life, health-care resources utilization, and mortality may seriously be affected [3,4]. Infection of the tracheobronchial tree and air pollution are thought to be responsible in most cases for AEs of COPD, although the causative factor remains unknown in as much as one-third of the patients [5]. Among the infections, bacteria are likely to be involved in at least 50% of cases, although it is not always feasible to differentiate between bacterial infection associated with an AE and chronic colonization of the tracheobronchial tree in stable COPD [6]. An increase in the baseline sputum neutrophilic inflammation typical of stable COPD and/or an increase in sputum purulence both support a role for bacterial infection in the etiology of an AE, but some biomarkers, such as the serum concentration of procalcitonin, have recently been introduced and may more reliably assist in the etiologic diagnosis and antibiotic treatment prescription [7]. Viruses and atypical bacteria seem less frequently responsible for AEs of COPD, being found, according to one study, in 30-40% and 5-28% of cases, respectively [5]. Several medical conditions, including pneumonia, congestive heart failure and pulmonary embolism, can mimic AE of COPD. Hence the diagnosis, which often may easily be gleaned from the medical history (mainly: increased dyspnea, cough, sputum, and purulence of sputum), needs to be confirmed, especially in the case of a lack of response to treatment, with objective evaluations, such as spirometry, pulse oximetry and arterial blood gas measurements, chest X-ray, ECG, and laboratory tests [2,8]. With regard to treatment of AE of COPD, the first step is to increase the dose and/or frequency of bronchodilator drugs, generally by adding a shortacting bronchodilator [9]. In addition, if the baseline FEV1 of the patient is less than 50% of predict- ed, systemic glucocorticosteroids (prednisone or prednisolone, 30-40 mg per day for 7-10 days) should be added to bronchodilators, as they have been shown to reduce recovery time, length of hospital stay and risk of early relapse [10] and to improve pulmonary function and gas exchange [11]. If the presence of bacterial infection is suggested by the clinical picture (in particular, increased dyspnea, increased sputum volume, and increased sputum purulence) then the patient should receive antibiotic treatment [12]. Patients presenting with severe AEs are difficult to manage at home and should be hospitalized. After initial hospital evaluation, they should be admitted, in the case of severe underlying COPD, significant comorbidities, older age, etc, to the general respiratory ward; alternatively, in the case of changes in mental status, severe/worsening hypoxemia, and/or hypercapnia, and/or respiratory acidosis, etc, to the intensive care unit. Supplemental oxygen is the treatment of choice for hypoxemia and should be titrated in order to achieve adequate levels of oxygenation without producing CO2 retention or acidosis [13]. A moderate to severe dyspnea, with respiratory frequency of > 25 breaths per minute, accompanied by objective signs of severe acidosis (pH < 7.35) and/or hypercapnia (PaCO2 > 45 mmHg) indicates the need for non invasive mechanical ventilation (NIV) [14]. In the case of failure of NIV or in more severe cases of acute respiratory failure (respiratory frequency > 35 breaths per minute, life-threatening hypoxemia, very severe acidosis, with a pH < 7.25, and/or severe hypercapnia, with a PaCO2 > 60 mmHg, etc.) invasive mechanical ventilation should be applied, either by oro-tracheal tube or tracheostomy [15]. References 1. Burge S, Wedzicha JA. COPD exacerbations: definitions and classifications. Eur Respir J Suppl 2003;41:46s-53s. 2. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000;161:1608-1613. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 71 obstructive pulmonary disease. Thorax 1995;50:834-837. 10. Aaron SD, Vandemheen KL, Hebert P, Dales R, Stiell IG, Ahuja J, Dickinson G, Brison R, Rowe BH, Dreyer J, Yetisir E, Cass D, Wells G. Outpatient oral prednisone after emergency treatment of chronic obstructive pulmonary disease. N Engl J Med 2003;348:2618-2625. 11. Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, Anderson P, Morgan NA. Effects of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med 1999;340:19411947. 12. Saint S, Bent S, Vittinghoff E, Grady D. Antibiotics in chronic obstructive pulmonary disease exacerbations. A metaanalysis. JAMA 1995;273:957-960. 13. O'Driscoll BR, Howard LS, Davison AG; British Thoracic Society. BTS guidelines for emergency oxygen use in adult patients. Thorax 2008;63(Suppl 6): vi1-vi68. 14. Lightowler JV, Wedzicha JA, Elliott MW, Ram FS. Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and metaanalysis. BMJ 2003;326:185. 15. Conti G, Antonelli M, Navalesi P, Rocco M, Bufi M, Spadetta G, Meduri GU. Noninvasive vs conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Intensive Care Med 2002;28:1701-1707. Inflammation in COPD and tobacco smoking L'infiammazione nella BPCO e nel fumo di tabacco Stefano Nardini, Caterina Baghiris Pulmonary and TB Unit- General Hospital, Vittorio Veneto (TV), Italy In the development of COPD, which is a leading cause of mortality and morbidity, inflammation plays a leading role. The disease involves different parts of the lungs in different ways, according to individual variability: in some people lesions of the central airways predominate, while in others lung parenchyma lesions are the main feature. Whatever the principal site of the lesion, tobacco smoking is the main cause of COPD, although other inhaled airborne pollutants may contribute. These inhaled gases and particles can cause damage to the respiratory system not only through inflammation but also through oxidative stress, especially if it is not effectively counter-balanced by the anti-oxidative system of the lungs. Overall, the above factors cause a number of abnormalities, which end in the central airways with mucous hypersecretion and ciliary dysfunction, in the peripheral lung with airflow limitation and hyperinflation, and, as far as the vascular compartment is concerned, with gas exchange abnormalities and pulmonary hypertension. Systemic effects (e.g. systemic inflammation and skeletal muscle wasting) as well as a decrease in local immunological response have also been demonstrated. Pulmonary rehabilitation is very important in the management of patients with COPD, to delay or reduce their disability. The first step in rehabilitation includes trying to achieve the best possible respiratory function and reduction of respiratory symptoms. Smoking cessation reduces such symptoms and the rate of decline of FEV1, but affects only partially inflammation (though it definitely reverses epithelial damage and consequently increases resistance to respiratory pathogens). How tobacco smoking causes COPD is largely unknown. Smoking causes inflammation of bronchi and lung and is associated with increased infiltration of immune cells but the inflammation persists after smoking cessation and anti-inflammatory drugs are not able to cure COPD. Some authors have proposed COPD as an autoimmune disease, triggered by smoking. It has long been known that smoking cessation can limit the decline in FEV1 observed in smoker COPD patients. The FEV1 improves during the first year after cessation and then, in sustained quitters, the rate of decline is reduced by some 50%. Even if smokers succeed only partially in quitting, alternating abstinence with relapses, they still show a reduction in the fall rate which is intermediate between continuing smokers and sustained quitters. In summary, the issue of inflammation in COPD and its links with smoking and smoking cessation CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 3. Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 2002;57:847-852. 4. Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA 1995;274:18521857. 5. White AJ, Gompertz S, Stockley RA. Chronic obstructive pulmonary disease. 6: The aetiology of exacerbations of chronic obstructive pulmonary disease. Thorax 2003;58:73-80. 6. Monsó E, Ruiz J, Rosell A, Manterola J, Fiz J, Morera J, Ausina V. Bacterial infection in chronic obstructive pulmonary disease. A study of stable and exacerbated outpatients using the protected specimen brush. Am J Respir Crit Care Med 1995;152:1316-1320. 7. Stolz D, Christ-Crain M, Morgenthaler NG, Leuppi J, Miedinger D, Bingisser R, Müller C, Struck J, Müller B, Tamm M. Copeptin, C-reactive protein, and procalcitonin as prognostic biomarkers in acute exacerbation of COPD. Chest 2007;131:1058-1067. 8. Wilkinson TM, Donaldson GC, Hurst JR, Seemungal TA, Wedzicha JA. Early therapy improves outcomes of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2004;169:1298-1303. 9. Moayyedi P, Congleton J, Page RL, Pearson SB, Muers MF. Comparison of nebulized salbutamol and ipratropium bromide with salbutamol alone in the treatment of chronic MRM 71 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 72 need to be further studied. Even if the effects of smoking cessation on inflammation are weak, the evidence of the effects on survival and quality of life of COPD patients is so overwhelming that smoking cessation should be implemented in the daily practice of chest physicians as the only certain way known to modify the natural history of COPD - at least in the early stage of this disease - and consequently as a cornerstone of its management. ERS recommendations on smoking cessation in respiratory patients should provide the lead for this implementation. References 1. Saetta M, Di Stefano A, Maestrelli P, Ferraresso A, Drigo R, Potena A, Ciaccia A, Fabbri LM. Activated T-lymphocytes and macrophages in bronchial mucosa of subjects with chronic bronchitis. Am Rev Respir Dis 1993;147:301-306. 2. Pesci A, Majori M, Cuomo A, Borciani N, Bertacco S, Cacciani G, Gabrielli M. Neutrophils infiltrating bronchial epithelium in chronic obstructive pulmonary disease. Respir Med 1998;92:863-870. 3. Turato G, Di Stefano A, Maestrelli P, Mapp CE, Ruggieri MP, Roggeri A, Fabbri LM, Saetta M. Effect of smoking cessation on airway inflammation in chronic bronchitis. Am J Respir Crit Care Med 1995;152:1262-1267. 4. Rutgers SR, Postma DS, ten Hacken NH, Kauffman HF, van Der Mark TW, Koëter GH, Timens W. Ongoing airway inflammation in patients with COPD who do not currently smoke. Thorax 2000;55:12-18. 5. Peinado VI, Barberá JA, Abate P, Ramírez J, Roca J, Santos S, Rodriguez-Roisin R. Inflammatory reaction in pulmonary muscular arteries of patients with mild chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1999;159:1605-1611. 6. MacNee W. Pathophysiology of cor pulmonale in chronic obstructive pulmonary disease. Part two. Am J Respir Crit Care Med 1994;150:1158-1168. 7. Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J 1977;1:1645-1648. 8. Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, Conway WA Jr, Enright PL, Kanner RE, O'Hara P, et al. Effects smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA 1994;272:1497-1505. 9. Donaldson GC, Seemungal TA, Patelet IS, Bhowmik A, Wilkinson TM, Hurst JR, Maccallum PK, Wedzicha JA. Airway and systemic inflammation and decline in lung function in patients with COPD. Chest 2005;128:19952004. 10. Wouters EF, Creutzberg EC, Schols AM. Systemic effects in COPD. Chest 2002;121(Suppl 5):127S-130S. 11. Tønnesen P, Carrozzi L, Fagerström KO, Gratziou C, Jimenez-Ruiz C, Nardini S, Viegi G, Lazzaro C, Campell IA, Dagli E, West R. Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy. Eur Respir J 2007;29:390-417. New evidence from large international trials Nuove evidenze da ampi studi internazionali Robert Stockley Department of Medicine, Queen Elizabeth Hospital, Edgbaston, Birmingham, United Kingdom COPD is a chronic slowly progressive disease characterised by predominantly irreversible airflow obstruction and punctuated by intermittent exacerbations. Most of the clinical trials and hence therapy of this condition has focused on short-term outcomes, especially the FEV1. This measure relates to the patients general health status, exercise capacity and predicts mortality. Conventional bronchodilators and inhaled corticosteroids produce an increase in group average FEV1 and this is accompanied by improved health status and exercise capacity, at least in the short-term. In addition, these therapies also reduce exacerbation rates and hence also improve health status by this action. However the effects of these therapies either alone or in combination for the long-term management and prognosis of COPD have been less well studied. Several recent long-term studies involving large patient cohorts have attempted to address these issues and they have resulted in unexpected observations, raising further questions about COPD management. 72 MRM TORCH [1] TORCH was the first COPD trial designed with mortality as the primary outcome. The study randomised 6,112 patients studied over 3 years and just failed statistically to demonstrate a benefit of ICS on mortality. The study was complicated by excess withdrawals from the placebo arm. Subsequent analysis suggested that combination therapy almost normalised FEV1 decline [2]. INSPIRE [3] INSPIRE investigated the effect of combination therapy (salmeterol/fluticasone, SFC) versus tiotropium on exacerbation rates in 1,323 COPD patients over 2 years. A similar rate of exacerbations was found in both arms although more patients withdrew on tiotropium. An increased reporting of “pneumonia” was seen in the SFC arm and more antibiotics were prescribed for exacerbations in the same arm compared to tiotropium. Interestingly, mortality was lower in patients on SFC, although the lack of a placebo arm did not permit a clarification of the importance of this finding. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 73 UPLIFT [5] Despite the suggestion from two recent meta-analysis/nest case-controlled studies that anticholinergic agents increased mortality in COPD [6,7], UPLIFT was designed to address this issue. The study included 5,993 patients randomised to tiotropium therapy or placebo over 4 years. Like with all recent studies, withdrawals were greatest in the placebo arm (a suggestion of efficacy of the drug). However the study did not indicate either an effect on mortality or FEV1 decline (the primary outcome measures). Subsequent post hoc analyses of subgroups did suggest a possible, though minimal, effect on both end points. In summary the short-term benefits of triple combination therapy seem additive in a patient cohort. Inhaled corticosteroids may have a benefit on overall mortality and long-term lung function decline. References 1. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J; TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007;356:775-789. 2. Celli BR, Thomas NE, Anderson JA, Ferguson GT, Jenkins CR, Jones PW, Vestbo J, Knobil K, Yates JC, Calverley PM. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med 2008;178:332-338. 3. Wedzicha JA, Calverley PM, Seemungal TA, Hagan G, Ansari Z, Stockley RA; INSPIRE Investigators. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med 2008;177:19-26. 4. Aaron SD, Vandemheen KL, Fergusson D, Maltais F, Bourbeau J, Goldstein R, Balter M, O'Donnell D, McIvor A, Sharma S, Bishop G, Anthony J, Cowie R, Field S, Hirsch A, Hernandez P, Rivington R, Road J, Hoffstein V, Hodder R, Marciniuk D, McCormack D, Fox G, Cox G, Prins HB, Ford G, Bleskie D, Doucette S, Mayers I, Chapman K, Zamel N, FitzGerald M; Canadian Thoracic Society/Canadian Respiratory Clinical Research Consortium. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med 2007;146:545555. 5. Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S, Decramer M; UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med 2008;359:1543-1554. 6. Singh S, Loke YK, Furberg CD. Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA 2008;300:1439-1450. 7. Lee TA, Pickard AS, Au DH, Bartle B, Weiss KB. Risk for death associated with medications for recently diagnosed chronic obstructive pulmonary disease. Ann Intern Med 2008;149:380-390. Rhinitis and sinusitis Le rinosinusiti Desiderio Passali Istituto di Discipline ORL, Università degli Studi di Siena, Siena, Italia Rhinosinusal diseases account for a large part of the clinical practice of otolaryngologists and general practitioners. Of these, rhinosinusitis is the one that has greatest need, considering its high social costs and risk of serious complications, of a correct therapeutic approach right from the outset of its natural history. Based on our present knowledge of nasosinusal pathophysiology, rhinosinusitis can be defined as any inflammatory process starting in the nose that, owing to close anatomic proximity, goes on to involve, through obstruction of the ostiomeatal complex, the sinusal cavities. More specifically, a closed ostium is no longer able to ventilate the cavity and less still to drain the secretions, and the diminished concentration of O2 associated to accumulation of secretions modifies the pH, altering the physiological metabolism of the mucosa. These variations of the sinusal environment create an ideal terrain for bacteria to multiply within a closed cavity; among the possible pathogens, Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis, the so-called “Infernal Trio”, are the germs that most frequently cause acute bacterial rhinosinusitis. The diagnostic approach to rhinosinusal diseases should be centered on an otolaryngological objective examination through rhinofibroscopy plus a series of rhinological instrumental examinations, e.g. frontal active rhinomanometry, acoustic rhinometry, and measurement of nasal mucociliary transport time, possibly combined with laboratory examinations and diagnostic imaging. Focusing on the therapeutic management, the main goals of the treatment of rhinosinusitis are to eradicate infection, reduce disease duration and prevent relapse. Choosing the antibiotic that is most appropriate for each specific case is thus very important. CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 OPTIMAL [4] Optimal was a 1-year study of 449 patients randomised to tiotropium, tiotropium and salmeterol, or both plus fluticasone. All combinations had a similar effect on exacerbation rates although the combinations resulted in better group measures in FEV1 and improvement in health status. MRM 73 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 74 This choice should be guided by a careful analysis of a series of factors that include the patient's general conditions, specific intolerances or allergies, concomitant pharmacological treatments, the mode of administration of the drug and, obviously, suspected or known resistance to antibiotics of the pathogens causing the rhinosinusitis. Although eradication of the infection remains the main treatment goal, numerous other support therapies, that have emerged from the latest advances in rhinosinusal pathophysiology, are of great importance in the management of rhinosinusitis. Among these, those that at present enjoy the widest consensus of the scientific community are: nasal decongestants, topical cortisone, non steroid antinflammatories, mucoregulators and, in the case of allergy, antihistamines. Finally, humidification of the nasal cavities with physiological or isotonic solution, thanks to its demonstrated effects of lubrification, humidification and removal of atmospheric inhalants from the nasal cavities, has gained a progressively wide consensus both in the treatment of acute forms and in postsurgical management of chronic rhinosinusitis. Asthma and rhinitis Asma e rinite Alfredo Potena Arcispedale S. Anna, Azienda Ospedaliero-Universitaria di Ferrara, Ferrara, Italia A close relation between asthma and allergic rhinitis has been reported by several epidemiological and clinical studies. However, the nature of this relation remains unclear. The prevalence of asthma and rhinitis varies throughout the world and allergic rhinitis is shown to be two times more prevalent than asthma. In rural countries, however, the numbers are usually lower than in more urbanized countries [1]. It was demonstrated that eosinophilic inflammation is present not only in asthmatics with nasal symptoms but also in asthmatics without clinical evidence of rhinitis [2]. The hypothesis that more severe rhinitis was associated with more severe asthma was supported by the results of a study in which subjects with high numbers of eosinophils in nasal mucosa were more likely to present more severe bronchial hyperresponsiveness [3]. Allergic rhinitis and sinusitis are associated with more severe asthmatic symptoms and more exacerbations in patients with poorly controlled asthma, even if they are not associated with low lung function [4]. Allergic and non-allergic rhinitis are risk factors for the development of asthma in adolescents and adults. Moreover, the presence of rhinitis and surrogates of asthma severity or health-resource consumption are associated. The same risk factors can induce asthma and rhinitis, including indoor and outdoor allergens, occupational agents, and nonspecific factors such as aspirin. Recognition of occupational rhinitis and avoidance of the causal factors might prevent development of severe persistent asthma [5]. Among risk factors it has been demonstrated that cigarette smoking is an important independent risk factor for the development of new asthma cases in adults with allergic rhinitis [6]. Atopic patients with no asthma and no rhinitis have 74 MRM some degree of lower airway inflammation. Rhinitis patients with no asthma have increased bronchial eosinophilia comparable with the group with both asthma and rhinitis. Also, in rhinitis patients without asthma there is an increase in thickness of the reticular basement membrane layer, a marker of airway remodelling [7]. The disease severity is an important factor in healthrelated quality of life (HRQoL), and psychosocial factors such as perceived control of disease explain a substantial amount of the variability in HRQoL among adults with rhinitis [8]. Rhinitis, even in the absence of atopy, is a powerful predictor of adult-onset asthma. In patients with asthma, treatment of concomitant allergic rhinitis was associated with significant reductions in risk of emergency room treatment and hospitalization for asthma [9]. The effect of rhinitis therapy on asthma outcomes in adult and adolescent patients with both seasonal allergic rhinitis and persistent asthma was investigated in a randomized controlled study that demonstrated the efficacy of treatment with fluticasone propionate aqueous nasal spray added to fluticasone/salmeterol for daytime total nasal symptom scores and individual daytime nasal specific symptoms (congestion, rhinorrhea, sneezing, and itching) [10]. Failure to consider treatment of rhinitis as essential to asthma management might impair clinical control of asthma. Furthermore, asthma and rhinitis in some patients can be controlled by the sole use of nasal medication [11]. New therapeutic options are now available for the treatment of allergic rhinitis and other inflammatory diseases. Among these, fluticasone furoate demonstrates high systemic clearance, low oral bioavailability and low absolute bioavailability after intranasal administra- MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 75 10. 11. 12. References 1. Shaaban R, Zureik M, Soussan D, Neukirch C, Heinrich J, Sunyer J, Wjst M, Cerveri I, Pin I, Bousquet J, Jarvis D, Burney PG, Neukirch F, Leynaert B. Rhinitis and onset of asthma: a longitudinal population-based study. Lancet 2008;372:1049-1057. 2. Gaga M, Lambrou P, Papageorgiou N, Koulouris NG, Kosmas E, Fragakis S, Sofios C, Rasidakis A, Jordanoglou J. Eosinophils are a feature of upper and lower airway pathology in non-atopic asthma, irrespective of the presence of rhinitis. Clin Exp Allergy 2000;30:663-669. 3. Ciprandi G. Cirillo I, Vizzaccaro A, Milanese M, Tosca MA. Nasal obstruction in patients with seasonal allergic rhinitis: relationships between allergic inflammation and nasal airflow. Int Arch Allergy Immunol 2004;134:34-40. 4. Dixon AE, Kaminsky DA, Holbrook JT, Wise RA, Shade DM, Irvin CG. Allergic rhinitis and sinusitis in asthma: differential effects on symptoms and pulmonary function. Chest 2006;130:429-435. 5. Demoly P, Bousquet J. The relation between asthma and allergic rhinitis. Lancet 2006;368:711-713. 6. Polosa R, Knoke JD, Russo C, Piccillo G, Caponnetto P, Sarva M, Proietti L, Al-Delaimy WK. Cigarette smoking is associated with a greater risk of incident asthma in allergic rhinitis. J Allergy Clin Immunol 2008;121:1428-1434. 7. Braunstahl GJ, Fokkens WJ, Overbeek SE, KleinJan A, Hoogsteden HC, Prins JB. Mucosal and systemic inflammatory changes in allergic rhinitis and asthma: a comparison between upper and lower airways. Clin Exp Allergy 2003;33:579-587. 8. Chen H, Katz PP, Eisner MD, Yelin EH, Blanc PD. Health-related quality of life in adult rhinitis: the role of perceived control of disease. J Allergy Clin Immunol 2004;114:845-850. 9. Corren J, Manning BE, Thompson SF, Hennessy S, Strom BL. 13. 14. 15. Rhinitis therapy and the prevention of hospital care for asthma: a case-control study. J Allergy Clin Immunol 2004;113:415-419. Nathan RA, Yancey SW, Waitkus-Edwards K, Prillaman BA, Stauffer JL, Philpot E, Dorinsky PM, Nelson HS. Fluticasone propionate nasal spray is superior to montelukast for allergic rhinitis while neither affects overall asthma control. Chest 2005;128:1910-1920. Stelmach R, do Patrocinio TNM, Ribeiro M, Cukier A. Effect of treating allergic rhinitis with corticosteroids in patients with mild-to-moderate persistent asthma. Chest 2005;128:3140-3147. Goyal N, Hochhaus G. Fluticasone furoate nasal spray in allergic rhinitis. Drugs Today (Barc) 2008;44:251-260. Scadding GK, Keith PK. Fluticasone furoate nasal spray consistently and significantly improves both the nasal and ocular symptoms of seasonal allergic rhinitis: a review of the clinical data. Expert Opin Pharmacother 2008;9:27072715. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, Zuberbier T, Baena-Cagnani CE, Canonica GW, van Weel C, Agache I, Aït-Khaled N, Bachert C, Blaiss MS, Bonini S, Boulet LP, Bousquet PJ, Camargos P, Carlsen KH, Chen Y, Custovic A, Dahl R, Demoly P, Douagui H, Durham SR, van Wijk RG, Kalayci O, Kaliner MA, Kim YY, Kowalski ML, Kuna P, Le LT, Lemiere C, Li J, Lockey RF, MavaleManuel S, Meltzer EO, Mohammad Y, Mullol J, Naclerio R, O'Hehir RE, Ohta K, Ouedraogo S, Palkonen S, Papadopoulos N, Passalacqua G, Pawankar R, Popov TA, Rabe KF, Rosado-Pinto J, Scadding GK, Simons FE, Toskala E, Valovirta E, van Cauwenberge P, Wang DY, Wickman M, Yawn BP, Yorgancioglu A, Yusuf OM, Zar H, AnnesiMaesano I, Bateman ED, Ben Kheder A, Boakye DA, Bouchard J, Burney P, Busse WW, Chan-Yeung M, Chavannes NH, Chuchalin A, Dolen WK, Emuzyte R, Grouse L, Humbert M, Jackson C, Johnston SL, Keith PK, Kemp JP, Klossek JM, Larenas-Linnemann D, Lipworth B, Malo JL, Marshall GD, Naspitz C, Nekam K, Niggemann B, Nizankowska-Mogilnicka E, Okamoto Y, Orru MP, Potter P, Price D, Stoloff SW, Vandenplas O, Viegi G, Williams D; World Health Organization; GA(2)LEN; AllerGen. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008;63(Suppl 86):8-160. Baiardini I, Pasquali M, Giardini A, Specchia C, Passalacqua G, Venturi S, Braido F, Bonini S, Majani G, Canonica GW. Rhinasthma: a new specific QoL questionnaire for patients with rhinitis and asthma. Allergy 2003;58:289-294. COPD BPCO Stefano Centanni, Silvia Della Fiore II Clinica di Malattie dell'Apparato Respiratorio, Università degli Studi di Milano, Ospedale San Paolo, Milano, Italia COPD is one of the main causes of morbidity and mortality in the adult population, with a rising incidence and significant consequences in terms of average direct and indirect costs. In particular, given the present growth rates, it is estimated that within 10-15 years COPD will be the third cause of mortality, and fifth cause of disability after ischemic heart disease, depression, road accidents and cerebrovascular disease [1]. COPD is a complex disease characterized by different phenotypes and clinical manifestations. For this reason, basing diagnosis, severity staging and follow up solely on spirometry indexes seems too simplistic and totally inadequate, both as a general concept and in clinical CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 tion, with an high receptor affinity [12]. Fluticasone furoate consistently improved the nasal and ocular symptoms of seasonal allergic rhinitis in patients sensitized to several allergens [13]. The ARIA statements [14] suggest that rhinitis and asthma should always be considered together in diagnosis and management. In patients with rhinitis particularly if persistent, moderate to severe, or allergic - it is important to ask simple questions about asthma and eventually to refine the diagnosis with pulmonary function tests [15]. MRM 75 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 76 76 MRM practice, to define the terms and complexity of the problem. From the clinical point of view COPD can be defined as a preventable and treatable disease, characterized by the presence of progressive, irreversible (or not fully reversible) airflow limitation and mostly associated to an inflammatory response in the lung secondary to the inhalation of particles or toxic gases of volountary (smoke) or environmental (pollution) origin [2]. The international scientific community considers COPD a lung disease whose effects involve both the respiratory system and other organs and body systems. In this optic it is necessary to carefully evaluate and differentiate comorbidity and complications: in the cardiovascular setting, for example, coronaropathy associated to COPD is probably a comorbidity, i.e. a disease of different districts of the organism caused by a common risk factor, in this case cigarette smoking. Cor pulmonale, on the contrary, seems to be more a consequence of COPD, in particular of the evolution of its natural history. Heart failure, a significant clinical problem which the pneumologist faces frequently in the management of COPD patients, seems to exemplify the need for a correct and rigorous classification of consequences and systemic effects of the disease. Key points of enormous value are the structural and functional effects of COPD. Among the former, are included, obviously, airway remodelling, damage to the lung parenchyma, skeletal muscle alterations, while the latter include the role of inflammation and its systemic effects and the role of ageing in chronic degenerative diseases. Undoubtedly these components are interdependent and constitute a vicious circle of great consequence in the clinical management of patients with chronic obstructive bronchitis. The effects of lung function limitations far more complex alterations than FEV1 and the Tiffeneau Index - in terms of exercise capacity, the consequent skeletal muscle deconditioning, progressive adaptation (including mental) to a sedentary lifestyle, the systemic consequences of hypoxia and oxidative stress, the smoke-related endothelial alterations and their repercussions on the pulmonary and systemic small vessels, the role and aetiopathogenesis of exacerbations and their impact on the immunological system and, finally, the interdependence with other chronic diseases such as diabetes - are just some pieces of a fascinating puzzle that the pneumologist is called on today to piece together in a global perspective. All this with the knowledge that this new approach cannot and must not take our attention away from the local manifestations in the lung that, whatever the systemic impact be, certainly remain the central elements of the disease. In brief, then, we should confront with an open mind the “new” without forgetting the certainties we already have gained. From this point of view there is now experimental evidence showing that adequate treatment strategies are able to slow the functional decline and prevent exacerbations, thus assuring the patient an improved prognosis and quality of life [3]. Patients affected by COPD see a progressive worsening of their health status, with consequent deterioration of the quality of life (QoL) on account of the progressive increase of dyspnea, first during exercise, then as disease advances also at rest, forcing them into an ever more marked sedentary condition [4]. The diagnosis once made, treatment of COPD must thus be aimed at achieving some priority goals, amongst which the improvement of symptoms, of exercise tolerance, of the patient's health status and consequently of the general clinical picture as well as the secondary prevention of complications and exacerbations [5]. The reduction of invalidity and of mortality is the most important long term challenge, but the improvement of exercise tolerance and consequently reducing the sedentary state increasingly appear as fundamental goals, also for the repercussions these outcomes have on the systemic consequences of COPD. Recent studies have confirmed the usefulness of medium-long term treatment of patients affected by COPD, in particular the role of the combination of ICS/LABA but also that of anticholinergics [4,6], in slowing down the decline of lung function, thus interferring in the natural history of the disease. This evidence suggests the desirability and importance of treating COPD patients at an earlier stage of disease in order to slow down the functional decline, assuring a better physical activity tolerance and reducing the number of exacerbations. These results are fundamental for delaying the “inevitable” sedentary state that causes a worsening of lifestyle which is a significant factor in the development of some of the more important complications of the disease, ensuring the patient at the same time a presumably improved QoL [7]. References 1. GOLD, “Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease”, 2006. http://www.goldcopd.com 2. Sanguinetti CM, De Benedetto F, Nardini S, Donner CF. AIMAR EXP-O 2008 Consensus/Dissensus Seminar “COPD is/is not a sistemic diseaseas?” Multidisciplinary Respiratory Medicine 2008;3:400-401. 3. Jones PW. Interpreting thresholds for a clinically significant change in health status in asthma and COPD. Eur Respir J 2002;19:398-404. 4. O'Donnell DE, Flüge T, Gerken F, Hamilton A, Webb K, Aguilaniu B, Make B, Magnussen H. Effects of tiotropium on lung hyperinflation, dysponea and exercise tolerance in COPD. Eur Respir J 2004;23:832-840. 5. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000;161:1608-1613. 6. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J; TORCH investigators. Salmeterol and fluticasone propronate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007;356:775-789. 7. Mora S, Cook N, Buring JE, Ridker PM, Lee IM. Physical activity and reduced risk of cardiovascular events:potential mediating mechanisms. Circulation 2007;116:2110-2118. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 77 Infezioni delle alte e basse vie respiratorie Pierluigi Viale, Luigia Scudeller Clinic of Infectious Diseases, University of Udine, Udine, Italy In the field of lower respiratory tract infection, a first issue to be discussed is that of disease classification. In the Guidelines for treatment of nosocomial pneumonia proposed by ATS and IDSA in 2005, the category of 'health-care associated pneumonias' (HCAP) was introduced, with the aim to differentiate them both from hospital-acquired pneumonia (HAP) sensu strictu and from community-acquired pneumonia (CAP) [1]. The term HCAP is intended to include pneumonias occurring in patients in a soto-say “intermediate” sphere, i.e. not staying in hospital but who have had recent contact with the healthcare system through nursing homes, hemodialysis clinics, or hospitalization. This definition has not met with much favour in the medical literature, and only three works, two retrospective and one monocentric, have attempted to verify its effectiveness in the clinical practice [2-4]. However, at the beginning of the present year, an Italian group published an important and decisive paper on the issue, based on a prospective, multicentric cohort study on 362 hospitalised patients during two 1-week surveillance periods. This study demonstrated that around 25% of these cases were included in the definition of HCAP and that their clinical course was characterized by higher resource consumption as determined by longer hospital stay (mean 18.7 days [CI, 15.9 to 21.5 days] vs. 14.7 days [CI, 13.4 to 15.9 days]) and higher mortality rate (17.8% [CI, 10.6% to 24.9%] vs. 6.7% [CI, 2.9% to 10.5%]) [5]. The study demonstrates perhaps definitively that HCAP is in fact a distinct clinical entity and that it should be considered as a highly severe disease where aggressive management strategies should be applied. Another issue where the scientific debate is still intense is the definition of a score that best predicts clinical severity of CAP. Severity scores have a pivotal role in the management of CAP, helping to guide some cardinal decisions such as the appropriate venue for care, diagnostic strategies, and intensity of antibiotic therapy. In more than a decade of clinical research, many prognostic scores have been developed, with different levels of complexity, each with its pros and cons. The two most popular (adopted, for instance, in the ATS guidelines) are the Pneumonia Severity Index (PSI) and the British Thoracic Society's CURB-65 which, despite some concerns about their overestimation of the predictive value of ages higher than 50 and 65 years respectively, have proved to be the most accurate for predicting pneumonia-related mortality [6,7]. To these, in recent times, a third score has been added, the SCAP score, that has also proved very efficient in predicting mortality, and whose most innovative characteristic is to use an age cut-off of 80 years, much more relevant in identifying the population at higher risk [8]. However, it is likely that mortality as the only outcome parameter would be inadequate to define management strategies at best. In fact, other endpoints linked to clinical management complexity (such as incidence of complications, time to clinical stability and duration of hospital stay) could have a higher value in guiding operative decisions. In this perspective, of great interest is the multicentric Spanish study published in January 2009, where the three main scores underwent a prospective validation in two independent cohorts of patients hospitalized with CAP (one of 1,189 patients admitted to a single centre, the other of 671 patients admitted to three different hospitals) to assess the accuracy and discriminatory power in predicting clinically relevant outcomes such as admission to the ICU, need for mechanical ventilation, progression to severe sepsis, and treatment failure, and their correlation with hospital stay length. The rate of all adverse outcomes and hospital length of stay increased directly with increasing SCAP, PSI, or CURB-65 scores (p < 0.001) in both cohorts. However, the SCAP score showed a higher discriminatory power than PSI or CURB-65, resulting to be the score most apt to predict the most significant complications in patients with CAP admitted to hospital [9]. Also on the issue of identifying outcome-related variables early in the clinical course of pneumonia, the role of early and frequent radiological follow up has recently been emphasized anew. Chest radiograph remains the cornerstone of the diagnosis of pneumonia both in clinical studies and in clinical practice. However, its role as a prognostic tool is much less clear, although the presence of multilobar infiltrates and pleural effusions are included in two widely used pneumonia severity indexes, namely SCAP and PSI score. Moreover, the attitude to repeat the chest radiograph within 24 to 48 h of ICU admission in patients with CAP is often questioned, because data on the clinical relevance of changes in radiologic images are very few. Recently, a secondary analysis in a multicenter observational study conducted in 457 patients with CAP admitted to ICU demonstrated that radiologic progression of pulmonary infiltrates in the first 48 h is a significant adverse prognostic feature. In fact, subjects in this cohort with radiologic progression had an increased risk of ICU death (adjusted OR, 3.1; 95% CI, 1.7 to 5.7) [10]. It is therefore increasingly evident that management of pneumonia should be constantly updated, to ensure management strategies able to address the CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 Upper and lower respiratory tract infections MRM 77 Multidisciplinary Respiratory Medicine 2009; 4(1): 46-79 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 78 continuous evolution of microbial populations and the changes in patient population characteristics. References 1. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcareassociated pneumonia. Am J Respir Crit Care Med 2005;171:388-416. 2. Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest 2005;128:3854-3862. 3. Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and communityacquired pneumonia: a single center experience. Antimicrob Agents Chemother 2007;51:3568-3573. 4. Carratalà J, Mykietiuk A, Fernandez-Sabé, Suárez C, Dorca J, Verdaguer R, Manresa F, Gudiol F. Health care-associated pneumonia requiring hospital admission: epidemiology, antibiotic therapy, and clinical outcomes. Arch Intern Med 2007;167:1393-1399. 5. Venditti M, Falcone M, Corrao S, Licata G, Serra P; Study Group of the Italian Society of Internal Medicine. Outcomes of patients hospitalized with communityacquired, health care-associated, and hospital-acquired pneumonia. Ann Intern Med 2009;150:19-26. 6. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM, Marrie TJ, Kapoor WN. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997;336:243-250. 7. Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, Lewis SA, Macfarlane JT. Defining community-acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003;58:377-382. 8. España PP, Capelastegui A, Gorordo I, Esteban C, Oribe M, Ortega M, Bilbao A, Quintana JM. Development and validation of a clinical prediction rule for severe communityacquired pneumonia. Am J Respir Crit Care Med 2006;174:1249-1256. 9. España PP, Capelastegui A, Quintana JM, Diez R, Gorordo I, Bilbao A, Zalcain R, Menendez R, Torres A. Prospective comparision of severity scores for predicting clinically relevant outcomes for patients hospitalized with communityacquired pneumonia. Chest; in press, Prepublished online January 13, 2009. doi:10.1378/chest.08-2179 10. Lisboa T, Blot S, Waterer GW, Canalis E, de Mendoza D, Rodriguez A, Rello J; Community-Acquired Pneumonia Intensive Care Units Study Investigators. Radiologic progression of pulmonary infiltrates predicts a worse prognosis in severe community-acquired pneumonia than bacteremia. Chest 2009;135;165-172. Innovation in pharmacological respiratory research Innovazione nella ricerca farmacologica in campo respiratorio Giuseppe Recchia Vice President-Medical & Scientific Director GlaxoSmithKline, Verona, Italy The evolution of medical and social culture as well as changes in healthcare politics, with an increased demand on saving, may ultimately lead to new drivers and enhanced barriers for drug reimbursement, such as value-based pricing and pay-for-perfomance. This novel scenario has generated the need to revise the evaluation criteria of innovation in the pharmaceutical context. If Pharma is to remain at the forefront of medical research and continue helping patients to live healthier and longer, it must become more innovative. In this context, the drivers for evolution are increased R&D productivity and innovation, i.e. incremental benefit of new drugs over available treatments in order to address unmet therapeutic need, in terms of improved efficacy and safety profile, ease of use (i.e. route of administration, devices, drug delivery), efficacy in subgroups of patients resistant/refractory to current treatments, drugs for orphan diseases. Along these lines, as regards chronic respiratory obstructive diseases such as asthma and COPD several new treatments are currently under development. Many of them display a highly specific mechanism, targeting a single receptor, enzyme or mediator, and may be effective in distinct subgroups of 78 MRM patients. More selective targeting of drugs to patients with particular subtypes of asthma or COPD might be possible in future with the identification of clinical phenotypes, biomarkers and genetic profiles. Nonetheless, an important step in simplifying the management of asthma and COPD and improving patient adherence with prescribed therapy is to reduce the dose frequency to the minimum necessary to maintain disease control. Therefore, the incorporation of once-daily dose administration is an important goal to improve adherence, leading to improved overall clinical outcomes. Since combination therapy with inhaled corticosteroids (ICSs) and a long acting β2-agonist (LABA) is now considered the elective therapeutic option for patients suffering from moderate to severe asthma or COPD, there is presently interest in developing fast-onset, once-daily combinations in a single device. The coming years will be pivotal as data for the most promising compounds become available from clinical studies. In fact, next-generation once-daily ICSs are under development as well as steroids with improved anti-inflammatory efficacy due to the addition of a NO-donating group. Furthermore, “dissociated” corticosteroids, devoid of detrimental MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 79 Asthma Although most subjects with asthma are well controlled with available treatments, about 10% of patients with severe disease do not respond well. Thus, severe asthma refractory to current therapies should be considered a major unmet need, driving to explore novel pharmacologic targets. Improved knowledge of asthma mechanisms has led to the recognition of different phenotypes that might reflect distinct types of inflammation. Thus, new classes of anti-mediator agents are under development, such as inhibitors of p38 MAP Kinase, Th2derived cytokines (i.e. IL-13), chemokine receptors and FLAP (5-lipoxygenase-activating protein). They could prove useful as monotherapies but also in combination with ICS, to reduce the corticosteroid insensitivity often observed in severe asthma. New immunomodulatory agents that influence the function of T-regulatory and T-helper cells in atopic patients are now progressing and may play a role in future therapy as well as new monoclonal antibodies directed to IgE or peptide-based vaccines or immunotherapy to induce IgE-specific antibodies. COPD Regarding COPD, some new long-acting antimuscarinic agents (LAMAs) are under development. The current opinion is that it will be advantageous to develop inhalers containing a combination of several classes of long-acting bronchodilator drugs in an attempt to simplify treatment regimens as much as possible. Consequently, several options for oncedaily dual-action ultraLABA+LAMA combination products are currently being evaluated for COPD treatment. It is likely that the development of oncedaily dual-action ultraLABA+LAMA combination products may serve as a basis for improved “triple therapy” combinations through coformulation with novel ICSs or novel antiinflammatory compounds such as inhaled phosphodiesterase (PDE)4 inhibitors, thus simplifying treatment regimens for COPD patients. A different approach is to develop a dimer molecule in which both pharmacologic activities are present: these molecules are known as M3 antagonist-β2-agonist (MABA) bronchodilators. The advent of a successful MABA product will revolutionize the field and open the door for a new range of combination products. The COPD pattern of inflammation is different from that of asthma, with predominance of neutrophils, macrophages, and cytotoxic T lymphocytes: several new compounds targeted at the inflammatory process are now in clinical development, such as antagonists of leukotriene B4, interleukin-8, tumor necrosis factor-α, transforming growth factor-β. In particular, antagonists of CXCR2, CXCR3 and CCR2 seem to be promising. Oxidative and nitrative stress, which are increased in COPD and amplify airway inflammation, possibly reducing the response to corticosteroids, are an important target for future therapy: stable antioxidants, such as analogues of superoxide dismutase, and inducible nitric oxide synthase inhibitors are now in clinical development. Broader-spectrum anti-inflammatory agents in development for COPD include selective phosphodiesterase inhibitors (PDE4B), inhibitors of p38 MAP kinase, nuclear-factor κB and phosphoinositide-3-kinase-γ. Presumably, an inhaled formulation is required for these compounds to improve the tolerability profile. There is also search for elastase inhibitors to prevent the development of emphysema and for drugs that may reverse the lung destruction. In general terms, it will be crucial to identify surrogate markers to predict clinical efficacy in respiratory diseases, so that new therapeutic approaches can be assessed. CF Donner Statements, Expert Opinion Consensus/Dissensus Seminar, Stresa, April 2009 - Razionali, Seminario di consenso/dissenso - l'opinione degli esperti, Stresa, aprile 2009 effects linked to the activation of gene transcription and with beneficial effects associated with transrepression, might become available. A variety of once-daily β2-agonists or ultra-long-acting β2-agonists (ultraLABAs) is also under development. MRM 79 RUBRICA MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 80 AIMAR Newsletter / Notiziario AIMAR EDITED BY /A CURA DI STEFANO NARDINI email: [email protected] Associazione Scientifica Interdisciplinare per lo Studio delle Malattie Respiratorie Questo numero di Multidisciplinary Respiratory Medicine è quasi interamente occupato dalla traduzione italiana delle raccomandazioni dell'ERS sulla disassuefazione dal fumo nei soggetti affetti da pneumopatie. Questa traduzione, dovuta alla cortesia dell'ERS e dell'Osservatorio Fumo Alcol e Droga dell'Istituto Superiore di Sanità, vuole dare - almeno nelle intenzioni - un contributo alla ripartenza, su nuove basi, della pratica clinica pneumologica. Perché definire in modo così “pomposo” un solo documento, e per di più su una materia, il fumo, decisamente non prioritaria per alcuna unità operativa pneumologica? La prima considerazione da svolgere è relativa all'effettiva necessità di ripartire in pneumologia su nuove basi, dato che alcuni potrebbero chiedersi se l'attuale assetto non sia più che sufficiente alla bisogna. La risposta a questo eventuale dubbio non può che essere positiva (c'è cioè bisogno di una ri-partenza, su nuove basi) e nasce da due motivazioni: la prima è che tutte le specialità (quindi non solo la nostra) debbono mutare il proprio assetto per rispondere alle nuove esigenze epidemiologiche cioè per rispondere ai nuovi bisogni della comunità di appartenenza, ossia all'elevata prevalenza di malattie cronico - degenerative. La seconda è che, nell'attuale situazione di riorganizzazione e razionalizzazione della sanità italiana, se si vuole sopravvivere come strutture operative (e non solo come singoli professionisti) si deve rivedere la propria pratica, adattandola alle risorse disponibili. Una riorganizzazione, dunque, per rispondere a nuove esigenze con minori risorse. E ritengo che chiunque di noi preferisca essere soggetto attivo (che propone sviluppi), piuttosto che passivo (che subisce tagli), di qualunque ri-organizzazione. Come più volte esposto, anche dalle colonne di questo giornale, la nostra riorganizzazione deve tendere a ridurre il carico delle malattie respiratorie 80 MRM e delle loro conseguenze sulla comunità attraverso la creazione di una rete con il territorio, nella quale la UO specialistica pneumologica sia lo snodo. La rete deve coprire tutta la “filiera”, garantendo la presenza specialistica sia nell'area della prevenzione primaria (fumo, inquinamento), sia in quella secondaria (diagnosi strumentale precoce) sia infine nella riabilitazione (riduzione e ritardata insorgenza dell'invalidità). Se le premesse svolte sono corrette, allora il fumo di tabacco occupa un posto prioritario, non solo in prevenzione (la disassuefazione dal fumo è il più efficace mezzo per ridurre mortalità e morbilità della popolazione, principalmente attraverso la riduzione dei casi di malattie respiratorie e cardiache), ma anche in terapia e riabilitazione (la disassuefazione dal fumo è la più efficace misura terapeutica, insieme all'ossigenoterapia, per migliorare la qualità di vita e la sopravvivenza nella BPCO e migliora perfino la sopravvivenza dei malati di tumore non operabili). Quindi lo specialista pneumologo dovrebbe attivarsi sul fronte della disassuefazione da subito. E altrettanto dovrebbe attivarsi sui fronti della diagnosi precoce, integrandosi con i medici di medicina generale e della riabilitazione, oltre che con le strutture distrettuali. La seconda considerazione riguarda il fatto che si tratta di un documento dell'ERS, società respiratoria internazionale che è di riferimento per tutti noi. E il fatto che questa società abbia inteso istituire un gruppo di lavoro apposito per la disassuefazione dal fumo e ne abbia poi pubblicato il lavoro risultante, è un segno dell'importanza dell'argomento. Anche perché - finalmente - si parla di disassuefazione dal fumo come misura terapeutica, essenziale per l'assistenza ai malati di malattie respiratorie e si dissipa una volta per tutte l'equivoco del trattamento del fumatore come pratica soltanto preventiva primaria. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 81 Per tali ragioni, la traduzione italiana delle raccomandazioni ERS è il modo migliore per porre all'ordine del giorno della Pneumologia italiana la necessità di cambiamento. Con questa traduzione, che fa parte del progetto ICEPERG ((Implementation of smoking CEssation in respiratory Patients according to the European Respiratory society Guidelines) di disseminazione e implementazione delle raccomandazioni dell'ERS, già presentato nel precedente numero del notiziario, si mette a disposizione della medicina respiratoria italiana lo stato dell'arte della disassuefazione. Al tempo stesso, AIMAR prosegue dunque nelle sua iniziative di formazione e ricerca: mette a disposizione di tutti uno strumento attuale di miglioramento della pratica clinica e pone un altro tassello nel progetto di ricerca ICEPERG. Tale progetto è un esempio di iniziativa di formazione e ricerca “sul campo” su un argomento “nuovo”, che coinvolge un centinaio di Colleghi sul territorio nazionale. Caratteristica di tutti i progetti di AIMAR è di riportare fedelmente i risultati delle ricerche portate avanti, non solo ai soci, ma anche alla comunità scientifica internazionale. È con piacere che annunciamo a tutti che il prossimo congresso dell’American Thoracic Society, a San Diego, ha accettato la presentazione di cinque comunicazioni su altrettanti progetti istituzionali di formazione e ricerca della nostra società scientifica. Ma questi non sono gli unici piani su cui si svolge l'azione di AIMAR. Infatti vi sono anche i seminari dedicati alla discussione di argomenti scientifici più “rarefatti” in ampia interazione tra esperti internazionali. Sempre nello scorso notiziario, ci eravamo soffermati sulla descrizione dell'evento EXP-O di Venezia, dedicato agli aspetti sistemici della BPCO. A primavera a Stresa ci sarà un altro importante seminario, appartenente alla stessa tipologia, dedicato alle patologie di interesse comune, pneumologico e otorinolaringoiatrico. A gennaio, sponsor anche AIMAR, si sono tenuti il convegno di Bari, sulla patologia respiratoria da inquinamento ambientale e, a Verona, il 12° congresso su asma bronchiale e BPCO, durante il quale c'è stata anche una sessione dedicata alle prospettive future della medicina respiratoria. A febbraio, si svolge il convegno regionale trentino su aspetti educazionali del paziente respiratorio cronico. Ma l'appuntamento più importante per noi soci AIMAR è quello della sesta conferenza internazionale sulla gestione e la riabilitazione dell'insufficienza respiratoria cronica e seconda conferenza italiana sull'approccio multidisciplinare alla medicina respiratoria, che avranno luogo a Napoli, tra il 4 e il 7 marzo 2009 (Figura qui sotto). Oltre al grande interesse scientifico, che nasce dal numero e dalla qualità degli specialisti internazionali e nazionali coinvolti (il programma è consultabile sul sito AIMAR all'indirizzo web: www.aimarnet.it), l'assise napoletana sarà importante anche perché verranno dati due annunci: il primo relativo al primo congresso congiunto AIMAR - capitolo italiano dell'ACCP, che si terrà nella primavera del 2011 e il secondo relativo alla costituzione ufficiale dell'Alleanza per le malattie toraco-polmonari (ATP) al cui statuto hanno già aderito formalmente 11 società scientifiche oltre ad AIMAR, società che aveva proposto l'aggregazione (i lettori ne hanno avuto notizia dalle “Pagine del segretario” sui numeri di marzo e giugno 2007, di Aria, Ambiente e Salute). Si tratta di due grandi passi concreti nella direzione dell'auspicata unità della medicina respiratoria italiana che, speriamo già da Napoli, proceda ulteriormente nel cammino con altre società scientifiche. Nel frattempo, si sono svolti sul territorio nazionale numerosi altri eventi di carattere formativo e orga- MRM 81 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 82 nizzativo, sponsorizzati - o direttamente organizzati - da AIMAR. A dicembre, a Barletta, sulla gestione integrata dell'insufficienza respiratoria progressiva; a san Bonifacio, in provincia di Verona, il quarto incontro di pneumologia in età pediatrica e a San Giovanni Lupatoto il convegno della sezione regionale veneta di AIMAR dal titolo “Le patologie respiratorie, una sfida per il presente e il futuro”, dedicato agli aspetti interdisciplinari dei percorsi diagnostici e terapeutici in medicina respiratoria. Ma va segnalato, per il suo particolare interesse e attualità, il corso avanzato tenuto da AIMAR a Milano, il 10 e 11 dicembre, avente come argomento la programmazione, la gestione e il controllo dell'unità operativa di pneumologia. 82 MRM In tal sede, sono state evidenziate nel dettaglio le problematiche che rendono necessario modificare l'assetto organizzativo e operativo delle UO di Pneumologia, che sono state sommariamente descritte nella prima parte di questo rapporto. Inoltre sono state discusse le possibili soluzioni operative, che verranno esposte in un articolo scientifico che comparirà su uno dei prossimi numeri di questa rivista. Un altro (piccolo) contributo alla ri-partenza su nuove basi della pratica clinica pneumologica, che peraltro non potrà fare a meno della partecipazione attiva di tutti i soci AIMAR e, in prospettiva, di tutti gli specialisti italiani. From the CFC Bulletin / Notiziario CFC Prosegue su Multidisciplinary Respiratory Medicine, a fronte della collaborazione tra AIMAR e Collegio Federativo Cardiologia (CFC), la pubblicazione di estratti del bollettino CFC, mensile di informazione e aggiornamento del Collegio. email: [email protected] CUORE E METABOLISMO RIDUZIONE DEI TASSI DI MORTALITÀ PRECOCE NEI PAZIENTI DIABETICI DI TIPO 2 Obiettivo dello studio è stato testare l'ipotesi che una serie di cambiamenti nell'utilizzo dei farmaci ipolipemizzanti, antipertensivi e ipoglicemizzanti orali possa essere associata alla riduzione dei tassi di mortalità precoce nei diabetici di tipo 2. A tale scopo i ricercatori hanno analizzato i dati di 197 studi clinici condotti in Gran Bretagna. Sono stati analizzati 48.579 pazienti con diabete di tipo 2 diagnosticato per la prima volta tra il 1996 e il 2006, tenendo conto di tutte le cause di mortalità e della somministrazione di farmaci ipolipemizzanti, antipertensivi e ipoglicemizzanti orali. Dal 1996 al 2006 l'incidenza del diabete di tipo 2 è risultata in aumento, mentre è diminuita nelle donne l'età media alla diagnosi. In un modello di regressione multipla aggiustato per età e comorbilità, la prescrizione di statine prima o dopo la diagnosi, la somministrazione di farmaci agenti sul sistema renina-angiotensina prima o dopo la diagnosi e l'assunzione di metformina prima o dopo la diagnosi sono risultate associate ad un minore tasso di mortalità. È molto probabile che una sempre più ampia diffusione dei controlli di lipidi, glicemia e pressione arteriosa possa a sua volta aver contribuito alla recente diminuzione dei tassi di mortalità precoce sia tra gli uomini sia tra le donne con diabete di tipo 2. Diabetes Care 2008,31;9: 1761-1766. STUDIO SIRCA: ASSOCIAZIONE TRA LIVELLI PLASMATICI DI LEPTINA E CALCIFICAZIONE CORONARICA Gli autori hanno valutato l'ipotesi che i livelli plasmatici di adiponectina e di leptina siano associati indipendentemente, ma in modo opposto, alla calcificazione dell'arteria coronarica, che costituisce una misura di aterosclerosi subclinica. Inoltre hanno valutato quali, tra i diversi biomarcatori di adi- RUBRICA MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 83 posità e di resistenza all'insulina, siano più forti predittori di calcificazione coronarica, oltre ai tradizionali fattori di rischio come la sindrome metabolica e la proteina C reattiva (CRP). A tale scopo sono stati valutati 860 pazienti non diabetici, asintomatici. Dallo studio SIRCA è emerso che, sebbene i livelli di leptina e di adiponectina siano associati entrambi a marker metabolici e di infiammazione, solo la leptina costituisce un significativo predittore indipendente di calcificazione coronarica. Journal of American College of Cardiology 2008,52;3:231-236. PREVENZIONE ANCHE LE CINESI SOFFRONO PER IL FUMO PASSIVO Ulteriori conferme sul ruolo del fumo passivo nello sviluppo di malattia cardiovascolare anche nella donna e in Cina. Lo studio “Passive Smoking and Risk of Peripheral Arterial Disease and Ischemic Stroke in Chinese Women Who Never Smoked” ha dimostrato un incremento significativo di incidenza oltre che di cardiopatia ischemica anche di vasculopatia periferica e di ictus nelle fumatrici passive rispetto ad un gruppo di controllo non esposto. http://circ.ahajournals.org/cgi/content/abstract/118/15/1535 SCOMPENSO CARDIACO NUOVO SCORE PER VALUTARE GLI SCOMPENSATI I pazienti ricoverati per scompenso cardiaco hanno un'elevata possibilità di essere riammessi in ospedale, se non sono adeguatamente trattati. Lo studio propone un algoritmo per stratificare i pazienti dimessi con uno score composto da 19 semplici parametri. Tra i quali: l'età, la creatininemia, le malattie delle vie respiratorie, del fegato e la depressione. Inoltre: bassi livelli di pressione arteriosa, sodiemia. Fattori predittivi negativi sono la terapia con statine o beta bloccanti. Am Heart J 2008;156:662-673. MRM 83 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 84 IPOTIROIDISMO E SCOMPENSO CARDIACO Un nuovo studio di Rodondi N e coll. ha evidenziato che anziani con ipotiroidismo subclinico severo hanno un rischio raddoppiato rispetto ai soggetti con tiroide normo-funzionante di sviluppare scompenso cardiaco. Si rende, pertanto, necessario sottoporre a screening i pazienti per ipotiroidismo subclinico e, se riscontrati positivi, trattarli. Rodondi N et al. J Am Coll Cardiol 2008;52:1152-1159. L'UTILIZZO DEI BLOCCANTI DEL TNF PUÒ FAVORIRE LO SCOMPENSO CARDIACO Dopo i glitazoni un nuovo farmaco utilizzato nel trattamento dell'artrite reumatoide viene messo sotto accusa per la possibilità di determinare sia l'insorgenza che l'aggravamento dello scompenso cardiaco nei pazienti anziani. È il risultato di una meta-analisi condotta da Soko Setoguchi e coll. di Boston in uno studio di confronto con il metotrexate che non avrebbe avuto quest'effetto. Am Heart J 2008;156:336-341. CARDIOPATIA ISCHEMICA PCI ED ANGINA STABILE Pubblicati i dati di un trial randomizzato che ha confrontato gli effetti della PCI rispetto al trattamento farmacologico ottimizzato nell'angina stabile. Il miglioramento dei sintomi è stato più evidente con la PCI specie nei soggetti con angina più severa. Purtroppo il beneficio è durato per un periodo che andava dai 6 ai 24 mesi. Dopo 36 mesi non si è evidenziata più alcuna differenza statisticamente significativa. N Eng J Med 2008;359:677-687. COMPENSO GLUCIDICO NEL PAZIENTE CRITICO Piuttosto sconcertante il risultato di una review e una meta-analisi di 29 trial randomizzati. Un più stretto controllo della glicemia nei pazienti diabetici non migliorerebbe la sopravvivenza e non ridurrebbe il bisogno di nuovi trattamenti dialitici. C'è soltanto una riduzione delle setticemie nei pazienti ricoverati in terapia intensiva. I mancati benefici pare siano imputabili ai rischi di ipoglicemia che può essere associata ad eventi neurologici che vanno dalle semplici vertigini al coma. JAMA 2008;300:933-944. IPERTENSIONE GLI IPERTESI OCCULTI SONO PIÙ A RISCHIO DEI PRE-IPERTESI I soggetti con ipertensione “mascherata” hanno un rischio di eventi cardiovascolari più elevato rispetto ai soggetti con pre-ipertensione. La corretta e precoce individuazione dell'ipertensione mascherata nella popolazione dei preipertesi (lo studio ha osservato 591 soggetti per un tempo medio di circa 7 anni) consente di ottenere una migliore statificazione prognostica finalizzata alla costruzione di un'ottimale strategia di prevenzione. A tale scopo è stata associata, alla misurazione clinica, la misurazione domiciliare con apparecchi automatici validati o le misure giorno-notte registrate mediante il moni84 MRM toraggio ambulatorio della pressione arteriosa delle 24 ore. Con queste metodiche sono stati considerati veri pre-ipertesi i soggetti con misure domiciliari al di sotto dei 135/85 mmHg con valori di pressione clinica nel range dell'ipertensione. Am J Hypertens 2008;21:879-883. BENEFICI DELLA RIDUZIONE DELLA PRESSIONE ARTERIOSA NEGLI STUDI ADVANCE, ONTARGET ED ASCOT Al 18th Scientific Meeting of the European Society of Hypertension ed il 22nd Scientific Meeting of the International Society of Hypertension (ISH) svoltosi a Berlino, sono stati discussi i nuovi risultati dai sottostudi dei noti trials Action in Diabetes and Vascular Disease: PreterAx and DiamicroN MR Controlled Evaluation (ADVANCE) trial, the ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial (ONTARGET), and the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT). Questi nuovi sottostudi forniscono ulteriori prove circa il beneficio che può essere atteso se si utilizzano strategie di trattamento più aggressive o di combinazione in ragione della multifattorialità della malattia. L'ANGOLO DEL POLSO MAN IS AS OLD AS HIS ARTERIES Numerosi Autori hanno studiato gli effetti dell'invecchiamento sull'apparato cardiovascolare ed è ben noto che tali effetti sono accelerati ed accentuati da stati patologici quali l'ipertensione arteriosa, il diabete eccetera. In un articolo uscito sul “Journal of the American College of Cardiology” del 2007, due Maestri come O'Rourke ed Hashimoto descrivono i fattori meccanici che entrano in gioco nel determinismo dell'invecchiamento arterioso, indicano quali sono gli effetti sul cuore, sui grandi vasi, sul microcircolo, suggeriscono come monitorizzare l'invecchiamento arterioso e le misure preventive e terapeutiche da mettere in atto. NURSING CARDIOLOGICO CORRELAZIONE TRA CARATTERI DELLA PERSONALITÀ E CORONAROPATIA Circa 50 anni fa venne introdotta la personalità di tipo A come fattore predisponente alla coronaropatia. L'entusiasmo della scoperta venne smorzato dai risultati di un trial pubblicato nel 2002. Oggi sembra che soltanto l'ostilità e la rabbia siano gli aspetti emozionali che mantengano un valore predittivo per la coronaropatia. Nel 1995 Denollet e coll. hanno introdotto una terza personalità chiamata D da 'Distressed' che darebbe un fattore prognostico negativo nella CAD. J Cardiovasc Med 2008,9:761768. Tratto da Bollettino CFC, anno 1, numero 6, novembre 2008, pubblicato da Edizioni Internazionali srl, Div. EDIMES, Pavia. L'Angolo della Cultura (non solo Medicina...) A CURA DELLA REDAZIONE La redazione intende lasciare questo spazio a disposizione per la presentazione di contributi culturali, anche non strettamente inerenti l'area medica. Gli interessati possono pertanto sottoporre alla redazione qualunque contributo (articolo, poesia, ecc.) che possa essere di interesse per i lettori e/o stimolare una riflessione ed un eventuale dibattito culturale. RUBRICA MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 85 email: : [email protected] Nello sguardo dell'amico scopriamo noi stessi In the eyes of a friend we discover ourself Francesco Iodice Già Direttore U.O. s.c. di Fisiopatologia Respiratoria, Ospedale A. Cardarelli, Napoli e-mail: [email protected] È singolare che la maggior parte degli uomini consideri un sentimento nobile come l'Amicizia come uno scambio di aiuti, una società di interessi, un commercio, insomma, da cui sperano di poter guadagnare qualche cosa. François de La Rochefoucauld, scrittore Massime Da quando il bambino esce dalla ristretta cerchia dei rapporti familiari per cominciare a entrare in contatto con la società che lo circonda, l'intera esistenza umana è accompagnata - talvolta scandita dalle amicizie: nella scuola e poi sul lavoro, nel tempo libero e in vacanza, per giovani, adulti e vecchi, per uomini e donne, per single e coniugati, eterosessuali, bisex e gay, gli amici sono una costante senza la quale sembra di non poter vivere. Eppure, il nostro tempo è caratterizzato o da solitudine di massa - ciascuno davanti al suo computer, vittima di bulimia informatica per non perdere neppure un frammento di mondo - o da adunate di massa - in occasione di concerti, o davanti a maxischermi per le partite di calcio - ma non più dall'Amicizia che è quel rapporto a due che evita alla solitudine di impazzire e alla gran massa di affogarci. Oggi “amicizia” è diventata una parola che cataloga amori che non si vogliono svelare, rapporti coniugali resi esangui dalla quotidianità, conoscenze utili a scambi di favore, relazioni ipocrite che un giorno potranno rivelarsi vantaggiose. Tutte cose che nulla hanno a che fare con l'Amicizia che costituisce l'esigenza della nostra anima quando nei fatti vuole trovare un significato, nel dolore un argine, nella gioia una comunicazione, nella monotonia della ripetizione un lampo di novità. Tutto ciò - che non è possibile nella solitudine, dove il dolore dilaga e la gioia resta inespressa, e neppure nella gran massa che concede espressione solo all'applauso - si può verificare solo nell'Amicizia dove la parola fuoriesce dalla “concretezza”, oggi La litografia “Amicizia, amore e verità”, pubblicata da Currier & Ives nel 1874. da tutti invocata ed eretta a valore, che altro non è che un limitarsi del linguaggio, un controllo delle parole, uno stare ai fatti, atteggiamento così frequente nelle cosiddette “persone serie”, quelle persone, cioè, realiste e di poche parole a cui non verrebbe mai in mente di chiedere a se stessi: “che ci faccio qui sulla terra? quali azioni debbo compiere perché la mia vita sia degna di essere vissuta?”. Nella solitudine queste domande restano nascoste mentre in mezzo alla gente sono considerate “pallose” e possono ingenerare qualche sospetto perché domande troppo cariche di senso. Eppure, l'anima è proprio di questi quesiti che si nutre: poco realisti ma carichi di simbolismo. Gli antichi greci, accanto al singolare ed al plurale, avevano inventato il “duale” che è lo spazio dell'amicizia, quello spazio cioè dove ogni parola, ancorché di senso eccedente, non viene mai considerata folle dall'amico che con affetto accetta ogni nostro sconfinamento. Secondo un'analisi della MSN Messenger, la mesMRM 85 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 86 L'amicizia si fa “nella fatica, riposo; nella calura, riparo; nel pianto, conforto” (Umberto Galimberti). saggeria della Microsoft (in tempi di Internet, l'analista non poteva che appartenere alla rete), ci sono quattro categorie principali di amici: 1) i “coltivatori”, coloro che tengono molto agli amici e cercano di avere incontri molto frequenti; 2) i “potatori”, che hanno la tendenza a fare amicizia molto in fretta e a porvi fine altrettanto rapidamente; 3) i “mietitori”, che hanno una ristretta cerchia di amici fidati che però frequentano raramente; 4) i “raccoglitori”, che fanno amicizia facilmente con molte persone, ma poi non approfondiscono il rapporto. Ciascuno può provare a riconoscersi in un modello. Sempre secondo il sondaggio, le amicizie migliori seguono di solito una rigida divisione sessuale: uomini con uomini, donne con donne. Pur essendoci, tuttavia, casi di grande amicizia fra maschi e femmine, preferiamo in questa sede non affrontare questo sentimento diverso dall'amore ma che qualche volta in amore si trasforma: d'altronde, proprio l'Amicizia è l'unico sentimento che con l'Amore può gareggiare. Per la verità, l'Amicizia precede l'Amore non solo nell'ordine alfabetico ma anche in quello morale, e dell'Amore, l'Amicizia è la forma più pura e disinteressata. Per capire il carattere disinteressato dell'Amicizia, è necessario capire anzitutto il carattere interessato dell'Amore. L'Amore è una forma di associazione a fini più o meno confessabili, nell'Amicizia invece le parti contraenti non si associano in vista di un fine, bensì per il solo godimento del sentimento di fratellanza. Il carattere interes- Asterix e Obelix: i due celebri Galli, amici per la pelle, creati nel 1959 dalla geniale matita di René Goscinny e Albert Uderzo. 86 MRM Jack Lemmon e Walter Matthau nella locandina di un loro famoso film: “The Front Page “ di Billy Wilder (1974). sato dell'Amore appare nel matrimonio allorché moglie a marito arrivano all'odio e desiderano vivere lontanissimi uno dall'altra, ma tornano istantaneamente ad unirsi quando qualcosa minaccia le ragioni “sociali”del loro matrimonio. Che cosa determina questo costante fondo di male nell'Amore? Forse la disparità fra le parti, che in Amore sembra condizione indispensabile, mentre condizione indispensabile nell'Amicizia è la parità, onde il detto del filosofo antico, amicitia inter aequales. Altra ragione fortissima del male nell'Amore è, secondo i casi, di dominare o di esser dominato; questa seconda condizione riguarda gli uomini che nell'Amore amano lasciarsi dominare. Ora come può esserci felicità di purezza se c'è autorità da una parte e sudditanza dall'altra? Infatti, sia il sottomettere gli altri a sé, come il sentirsi sommessi altrui contengono in sé i germi della ribellione, dell'odio, della vendetta. Uno degli amanti può sentirsi in una posizione particolarmente spiacevole, può avere cioè la sensazione di essere caduto in una trappola insidiosa. E su chi legittimamente vendicarsi di questo stato inglorioso, di questo marchio se non sulla persona stessa che amiamo? Quando la disparità fra gli amanti sparisce, anche la materia del contendere, la conflittualità fra gli amanti scompare. Noi camminiamo e, così camminando, attraversiamo la vita a generazioni separate. La generazione comune è il legame più forte che unisce uomo ad uomo. Noi amiamo i nostri figli, amiamo i nostri genitori e continuiamo ad amarli nel ricordo, ma nell'amore fra generazioni diverse vi è qualcosa di innaturale e, per quanto velatissimo, qualcosa di mostruoso. All'amore fra generazioni diverse manca la prima condizione d'amore, che è la condizione di parità. MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 87 Il sorriso sereno dell'amicizia fra due seniores. Nell'amore fra generazioni diverse, l'amore è corrotto dalla variante più aspra della lotta di classe, che è la lotta fra generazione e generazione. L'amore invece fra uomini di medesima generazione è l'amore più naturale e dunque più libero, più disinteressato, e più profondo perché amore fra pari; è amore senza invidia e senza gelosia. Sentimento che non è costretto né alla rinuncia, né all'ambizione (megalomania, così frequente e così tormentosa nell'amore). Noi uomini di una medesima generazione, uniti dal legame più forte, coltiviamo la solidarietà più legittima, l'amicizia più profonda, la vera fratellanza. I più si giustificano: dove trovare il tempo per coltivare un'amicizia? La mancanza di tempo è un alibi, e quanto poco ne avevamo quando passavamo le ore a parlare con gli amici: era un bisogno, un'esigenza così forte da anteporre il sonno e lo studio, la famiglia e il dovere. Non a caso, l'Amicizia è diffusa tra i giovani e in vecchiaia, perché si dispone di molto tempo. E che dire di una cultura che concepisce l'amicizia come “una perdita di tempo”? Non ci prendiamo in giro: non è il tempo che ci manca, è la capacità di stare l'uno con l'altro in quella forma intermedia che non è la fusione dell'amore e neppure l'anonimato dei rapporti interpersonali - è la capacità di muoversi in quella zona di confine tra le prescrizioni della ragione e quegli sprazzi di follia che di continuo attraversano la nostra anima e che solo l'amicizia sa accogliere. Perché nella nostra breve esistenza ci dovremmo privare di questo spazio? Quale perverso tiranno ci impone di stare ai fatti e nient'altro che ai fatti? Tra l'anonimato del pubblico e la solitudine del privato, vogliamo conservare lo spazio intermedio dell'Amicizia che va assolutamente tutelata perché forse è l'unico spazio che ci rimane per un residuo di sincerità, una forma di autoriconoscimento, secondo il modulo che Platone ci indica quando dice: “Se uno, con la parte migliore del suo occhio guarda la parte migliore dell'occhio dell'amico, vede se stesso”. Infatti, nell'amicizia scopriamo noi stessi, l'amico ci fa venire a contatto con la parte migliore di noi, perché il suo sguardo è lo sguardo dell'altro che indaga il tuo cuore e lo scruta e, poiché è sincero, non può che dirti ciò che è male e ciò che è bene per te. A meno che non si diventi per se stesso il maggiore ingombro da evitare, qualcuno con cui non si sa che rapporti avere, qualcuno da scansare o addirittura da affogare con le cose da fare - per esempio i viaggi - (quante volte abbiamo sentito da iperattivi e disordinati produttori di stress: “Vado spesso in giro per il mondo per divertirmi e non pensare!”) per non trovarsi a tu per tu con questo sconosciuto cioè se stesso - che lo sguardo accogliente dell'amico potrebbe cominciare a raccontare. “Senza amici, nessuno sceglierebbe di vivere”, scriveva Aristotele duemila e trecento anni orsono. E Madre Teresa di Calcutta di rincalzo: “Trova il tempo di essere amico: è la strada della felicità”. Parole che rimangono valide anche agli albori del ventunesimo secolo, nell'era degli sms, delle chatline e di Internet. MRM 87 RUBRICA MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 88 Meeting Calendar Questa rubrica informa i lettori dei prossimi eventi congressuali, nazionali ed internazionali, nell’ambito della Medicina Respiratoria; fornisce un recapito a cui rivolgersi per ottenere ulteriori informazioni. email: [email protected] WHEN WHERE WHAT WHO TO CONTACT February 5-6 Napoli (Italy) February 5-7 Sitges, Barcelona (Spain) Congresso: “Il paziente respiratorio: dalla clinica alle strategie terapeutiche”II edizione Fifth Forum on Respiratory Tract Infections February 9-10 Milano (Italy) Maui, Hawaii (USA) Agra (India) 2009 February 15-18 February 18-22 February 19-21 Bari (Italy) February 20-21 Albuquerque, New Mexico (USA) Rovereto, TN (Italy) February 21 February 27-28 Messina (Italy) February 27 Foggia (Italy) February 28 Manfredonia, FG (Italy) March 4-7 Napoli (Italy) March 24-27 Brussels (Belgium) Barcelona (Spain) Cannizzaro, CT (Italy) March 27-28 March 27-28 April 1-4 88 MRM VII Forum Internazionale: Respiro, funzione vitale 9th Annual Symposium: Current Concepts in Pulmonary & Critical Care International Critical Care Congress and 15th Annual Conference of Indian Society of Critical Care Medicine CardioPneumo AIMEF 2009 6° Congresso Nazionale - 4th International Conference on Cardiovascular and Respiratory Disease in Family Medicine 2009 New Mexico Thoracic Society Symposium: Update on Respiratory Tract Infections Convegno Regionale in Pneumologia. Aspetti Educazionali del Paziente Respiratorio Cronico Congresso: Il Management delle Patologie Respiratorie: dalla prevenzione al trattamento nella pneumologia del prossimo futuro Convegno: “Appropriatezza di impiego degli antibiotici nelle infezioni delle vie respiratorie” Convegno: “Appropriatezza di impiego degli antibiotici nelle infezioni delle vie respiratorie” Pulmonary Advances “VI International Conference on Management & Rehabilitation of Chronic Respiratory Failure” and “II Italian Conference on a Multidisciplinary Approach to Respiratory Medicine” 29th International Symposium on Intensive Care and Emergency Medicine 12th International Conference on Home Mechanical Ventilation Problemi Aperti in Medicina Respiratoria: Confronto con gli esperti. Seconda edizione Stresa, NO (Italy) Inflammation and infection in upper and lower respiratory tract: Expert Opinion Consensus/Dissensus Seminar = evento AIMAR iDea Congress, Roma [email protected] www.ideacpa.com Publi Creations - Aim www.aim-internationalgroup.com/ 2009/respinf Academy www.academy-congressi.it [email protected] www.ala-hawaii.org/test_new.asp www.criticare2009.org Acmesi, Bari www.acmesi.net www.cardiopneumoaimef.it Judy Holcopmbe (505) 899-1254 [email protected] Elsevier, Milano [email protected] www.elsevier.it Aim, Milano www.aimgroup.it Meeting Planner, Bari www.meeting-planner.it Meeting Planner, Bari www.meeting-planner.it www.effetti.it www.makevent.it www.intensive.org www.jivd-france.com iDea Congress, Roma [email protected] www.ideacpa.com [email protected] www.aimarnet.it = evento patrocinato da AIMAR MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 89 WHEN WHERE WHAT WHO TO CONTACT April 2-4 Stresa, NO (Italy) 3rd European Respiratory Care Association Congress April 23-25 Philadelphia, PA (USA) San Diego, CA (USA) Vieste, FG (Italy) Pollenzo, CN (Italy) Vienna (Austria) Ravenna (Italy) Scientific Meeting: “Internal Medicine 2009” Victory Project Congressi, Milano [email protected] www.victoryproject.it www.acponline.org ATS 2009 International Conference [email protected]. May 15-20 May 29-30 June 6 September 12-16 September 20 December 2-5 Milano (Italy) December 6-10 Buenos Aires (Argentina) = evento AIMAR Convegno: “Giornate pneumologiche garganiche” Meeting Planner, Bari www.meeting-planner.it Convegno: Riabilitazione nelle Malattie Granda Esprit Convegni, Cuneo Cardio-Polmonari Croniche [email protected] European Respiratory Society ERS, Lausanne (Switzerland) Annual Congress 2009 www.ersnet.org Convegno: “Rinite ed Asma” Mael Impruneta (Fi) +39 055 2373684 [email protected] X Congresso UIP - XL Congresso Nazionale AIPO iDea Congress, Roma Certezze Scientifiche e Criticità Organizzative [email protected] in Pneumologia www.ideacpa.com XXI World Allergy Congress Ana Juan Congress, Buenos Aires www.anajuan.com = evento patrocinato da AIMAR MRM 89 MRM 01-2009_def:Layout 1 24/02/09 10:09 Pagina 90 Cara/o Collega, il Consiglio Direttivo di AIMAR mi ha incaricato qualche tempo fa di curare l'organizzazione di un sistema assembleare interno all'Associazione, analogamente a quanto già presente in altre Società Scientifiche nazionali ed internazionali (ad esempio European Respiratory Society). Nell’accingermi al lavoro ho rilevato che circa il 40% degli iscritti non ha dichiarato la propria attività corrente e questo elemento è imprescindibile da un tentativo di costituire Assemblee con caratteristiche dottrinali e pratiche soddisfacenti. Poiché la nostra Associazione è largamente multidisciplinare appare fondamentale inquadrare al meglio il “corpus” societario prima di formulare delle proposte che dovrebbero per quanto possibile venire incontro alle attese. Chiederei pertanto a tutti i soci di rispondere a questo breve e semplice questionario al fine di impostare i passi successivi prima di sottoporli al vaglio del Consiglio Direttivo. Un cordiale saluto Lucio Casali Coordinatore delle Aree Scientifiche e di Ricerca Da restituire alla segreteria AIMAR Fax +39 0322 869737 QUESTIONARIO INFORMATIVO Cognome e Nome: ______________________________________________________________________________________________________________ Età:____________________________________________________________________________________________________Sesso: ___________________ via:_______________________________________n: __________cap: ____________città: _________________prov:_______________________ e-mail: ________________________________________________ telefono ___________________________________________________________ Anno di laurea: __________________________________________________________________________________________________________________ Titolo e anno delle specializzazioni conseguite (possibilmente in ordine cronologico): 1) ________________________________________________________________________________________________________________________________ 2) ________________________________________________________________________________________________________________________________ 3) ________________________________________________________________________________________________________________________________ 4) ________________________________________________________________________________________________________________________________ 5) ________________________________________________________________________________________________________________________________ Quale di queste specialità viene esercitata quotidianamente? ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ In quale delle seguenti categorie collochi la tua attività? o o o o o o o Università Ospedale Territorio Medico di Medicina Generale Specialista convenzionato Sanità Pubblica Altro (specificare): _____________________________________________________________________________________________________________ N.B. è possibile indicare più di una categoria (ad es. Università + Ospedale) Oltre alla tua attività corrente svolgi anche ricerca? o o o o SI NO Saltuariamente In caso affermativo, in quale campo? ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ Come vorresti sviluppare in futuro la vita di un’Associazione come AIMAR? ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________ #
Scaricare