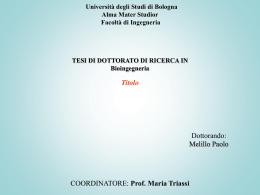
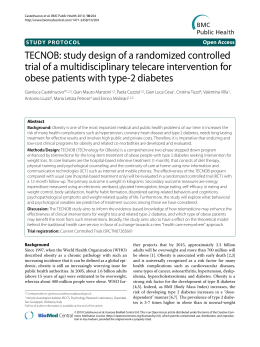
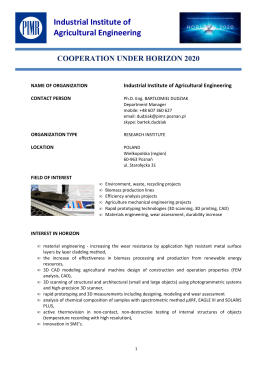
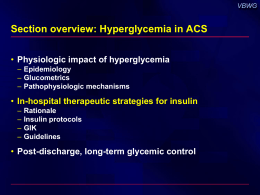
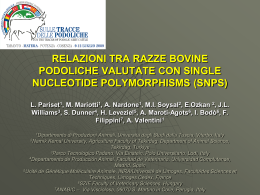
European Heart Journal Advance Access published March 29, 2015 CLINICAL RESEARCH European Heart Journal doi:10.1093/eurheartj/ehv083 Coronary artery disease Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes in the risk of coronary artery disease Stephanie Ross 1,2,3, Hertzel C. Gerstein 1,4, John Eikelboom 1,4, Sonia S. Anand 1,2,3,4, Salim Yusuf 1,2,4, and Guillaume Paré 1,2,3,5,6* 1 Population Health Research Institute, Hamilton Health Sciences, McMaster University, Hamilton General Hospital Campus, Hamilton, ON, Canada; 2Department of Clinical Epidemiology & Biostatistics, Population Genomics Program, McMaster University, Hamilton, ON, Canada; 3Population Genomics Program, Chanchlani Research Centre, McMaster University, Hamilton, ON, Canada; 4Department of Medicine, McMaster University, Hamilton, ON, Canada; 5Department of Pathology and Molecular Medicine, McMaster University, Hamilton, ON, Canada; and 6Thrombosis and Atherosclerosis Research Institute, Hamilton Health Sciences and McMaster University, Hamilton, ON, Canada Received 6 January 2015; revised 19 February 2015; accepted 3 March 2015 Introduction ----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords Genetic variants † Dysglycaemia † Diabetes † Coronary artery disease Introduction Large prospective observational studies have reported that type 2 diabetes increases the risk of cardiovascular events by 2-fold following the adjustment for other risk factors.1 These and other studies have also reported a progressive relationship between various measures of glycaemia, including fasting glucose (FG) and glycated haemoglobin (HbA1c), and cardiovascular outcomes, both in people with diabetes and in people without a history of diabetes or cardiovascular events.1,2 Conversely, large randomized controlled trials assessing the effect of glucose lowering have also yielded mixed results.3 – 7 For instance, meta-analyses have demonstrated a modest 9% reduction in the composite cardiovascular outcome and a 15% reduction in coronary artery disease (CAD).8 – 10 Moreover, at least one analysis suggests that this effect on CAD is due to the effect of the intervention on HbA1c.11 * Corresponding author. Tel: +1 905 527 4322, Fax: +1 905 296 5806, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected]. Downloaded from by guest on April 20, 2015 Type 2 diabetes is a strong risk factor for coronary artery disease (CAD). However, the absence of a clear reduction in CAD by intensive glucose lowering in randomized controlled trials has fuelled uncertainty regarding the causal role of dysglycaemia and CAD. ..................................................................................................................................................................................... Objective To assess whether Mendelian randomization supports a causal role of dysglycaemia and diabetes for risk of CAD. ..................................................................................................................................................................................... Methods Effect size estimates of common genetic variants associated with fasting glucose (FG), glycated haemoglobin (HbA1c), and diabetes were obtained from the Meta-Analyses of Glucose and Insulin-Related Traits Consortium and Diabetes Genetics Replication and Meta-Analysis consortia. The corresponding effect estimates of these single nucleotide polymorphisms (SNPs) on the risk of CAD were then evaluated in CARDIOGRAMplusC4D. ..................................................................................................................................................................................... Results SNPs associated with HbA1c and diabetes were associated with an increased risk of CAD. Using information from 59 genetic variants associated with diabetes, the causal effect of diabetes on the risk of CAD was estimated at an odds ratio (OR) of 1.63 (95% Confidence Interval (CI): 1.23–2.07; P ¼ 0.002). On the other hand, nine genetic variants associated with HbA1c were associated with an OR of 1.53 per 1% HbA1c increase (95% CI: 1.14–2.05; P ¼ 0.023) in the risk of CAD while this effect was non-significant among 30 genetic variants associated with FG per mmol/L (OR: 1.18, 95% CI: 0.97 –1.42; P ¼ 0.102). No significant differences were observed when categorizing genetic loci according to their effect on either b-cell dysfunction or insulin resistance. ..................................................................................................................................................................................... Conclusions These Mendelian randomization analyses support a causal role for diabetes and its associated high glucose levels on CAD, and suggest that long-term glucose lowering may reduce CAD events. Page 2 of 9 Methods Data sources All single nucleotide polymorphism (SNP) associations were taken from public repositories of genome-wide databases, where each of .3 million SNPs are tested for their relationship with a given outcome using data from .80 000 individuals. Effect size estimates for single SNPs associated with glucose traits (FG and HbA1C) were obtained from the MetaAnalyses of Glucose and Insulin-Related Traits Consortium (MAGIC) study, a genome-wide association study (GWAS) consisting of .133 010 of European descent without diabetes.15 – 17 Genetic data for the association of diabetes was obtained from the Diabetes Genetics Replication and Meta-Analysis (DIAGRAM) Consortium study, a GWAS of 34 840 cases and 114 981 controls of European descent.18 Genetic data for the association of the risk of CAD was obtained from the Coronary Artery Disease Genome-wide Replication and Meta-Analysis (CARDIoGRAMplusC4D) Consortium study, a two-stage GWAS of 63 746 cases of CAD and 130 681 controls.19 When not available in CARDIoGRAMplusC4D, effect estimates were obtained from the CARDIoGRAM, which is a meta-analysis of 22 GWAS studies of 22 233 cases and 64 762 controls.20 Coronary artery disease outcomes were defined as one of the following: myocardial infarction (MI), .50% stenosis in at least one coronary vessel at angiography, history of percutaneous transluminal coronary angioplasty or coronary artery bypass graft surgery, angina or death due to CAD.19 Genetic data on the association of low-density lipoprotein (LDL), high-density lipoprotein (HDL), total cholesterol (TC), and triglycerides (TG) were obtained from the Global Lipids Genetics Consortium study, a GWAS of 188 577 individuals from 60 studies.21 Genetic data for the association of body mass index (BMI) was obtained from the Genetic Investigation of Anthropometric Traits (GIANT) GWAS in .133 154 European individuals.22 Further details of each consortium are included in the Supplementary material online, Methods. SNP selection SNPs were selected if they were associated with at least one of the two glucose traits (FG and HbA1C) or diabetes at genome-wide-level significance of P , 5 × 1028. For duplicate SNPs and SNPs associated with glucose trait or diabetes that were ,500 kb apart, we obtained the linkage disequilibrium estimates using data from the 1000 Genomes Pilot 123 and then assigned a lead SNP based on the strength of association with either glucose traits or diabetes (Supplementary material online, Figure S1). Statistical analysis We first tested FG, HbA1c, and diabetes separately for the risk of CAD. This was done by using the effect estimates of SNPs associated with FG, HbA1c, or diabetes with their corresponding genetic effect estimates on CAD using data from the MAGIC, DIAGRAM, and CARDIOGRAMplusC4D consortia, respectively. Figure 1 represents the schematic representation of the Mendelian Randomization design. Linear regressions (without intercept) were performed using the effect estimates of SNPs on FG, HbA1C, and diabetes as the independent variables and the genetic effect sizes on CAD as the dependent variable. Since SNPs associated with dysglycaemia may not only be directly associated with the risk of CAD but also with other CAD risk factors, we adjusted the causal effect of dysglycaemia on the risk of CAD for other CAD risk factors. This was done by developing multivariate models adjusting the effect of each SNP on CAD for its genetic effect on LDL, HDL, TC, TG, and BMI. Throughout the manuscript, the effect of the SNPs associated with diabetes on the risk of CAD was expressed as the relative risk of CAD among diabetic individuals when compared with individuals without diabetes. Here, literature estimates of the prevalence of diabetes and the prevalence of CAD in non-diabetic individuals were obtained,1,2,24 and these estimates were applied to derive the relative risk of CAD associated with diabetes (further details in Supplementary material online, Methods). Estimates of FG available in units of mg/dL were converted to mmol/L using a multiplication factor of 0.055. Genetic effects of fasting glucose and HbA1c on risk of CAD were expressed per 1 mmol/L and 1% genetic increase in fasting glucose and HbA1c, respectively. Next, the causal effects of glucose traits and diabetes on the risk of CAD derived from Mendelian randomization were compared with estimates obtained from observational studies to determine if there was a similar magnitude of effect. We compared the magnitude of the genetic effect for the risk of CAD to the effect obtained from observational studies using a z-test based on the Altman and Bland method.25 We also derived power estimates of the causal effect of SNPs associated with glucose traits and diabetes on the risk of CAD using simulations. To do so, we first calculated the predicted effect of each SNP on CAD by matching their effect on glycaemia or diabetes with expected effect on CAD based on estimates from observational studies. We then performed 10 000 random simulations, regressing the predicted effect of each SNP on CAD on their known effect on glucose traits and diabetes. Finally, loci were categorized according to their effect on ‘b-cell dysfunction’ or ‘insulin resistance’ to determine if association with CAD could be ascribed to either hypo- or hyperinsulinaemia, respectively. Only SNPs with an unequivocal effect on ‘b-cell dysfunction’ or ‘insulin resistance’ based on literature reviews were included in this analysis, with all SNPs of unknown function or with conflicting reports excluded. All statistical analyses were performed using R. Downloaded from by guest on April 20, 2015 The conflicting reports from epidemiological studies and clinical trials regarding the potential effects of dysglycaemia on cardiovascular outcomes have fuelled uncertainty regarding the etiologic relationship between dysglycaemia and CAD. However, Mendelian randomization analyses may help to clarify the relationship between glucose traits, diabetes, and risk of CAD. This approach uses genetic associations to explore the effects of modifiable exposures on outcomes. It is based on the principle that genetic variants are randomly allocated at birth and this distribution is independent of many factors that may bias observational associations,12 such as confounding factors and reverse causation.13 However, this approach does not rule out the possibility that genetic variants associated with dysglycaemia may also be correlated with other CAD risk factors such as dyslipidaemia, blood pressure elevation, or weight gain.12 This limitation can be circumvented by adopting the method proposed by Do et al. 14 to adjust Mendelian randomization analyses for genetic effects on these other risk factors. This approach allows for the dissection of causal influences for the risk of CAD among sets of correlated glucose traits and CAD risk factors. To explore the relationship between dysglycaemia-related indices (i.e. FG, HbA1C and diabetes) and the risk of CAD, we identified genetic variants associated with these three indices and then confirmed whether their genetic effect supports a causal association with CAD. We also explored whether genetic variants that modify b-cell function have a different relationship to CAD than variants that modify insulin resistance. S. Ross et al. Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes Page 3 of 9 Figure 1 Schematic representation of the Mendelian randomization design. Association of glucose levels and diabetes with risk of coronary artery disease Thirty SNPs were associated with FG,15 nine associated with HbA1C,17 and 59 associated with diabetes.18 Further details on the risk alleles and minor allele frequencies for the trait-specific SNPs are presented in Supplementary material online, Table S1. To investigate the consistency and directional effect of SNPs association with glucose traits and CAD, we plotted the effect of SNPs on FG, HbA1c, and diabetes with their corresponding effect on risk of CAD (Figure 2). Next, to explore whether SNPs associated with glucose traits and diabetes predict the risk of CAD, we performed linear regression analyses for each trait using the respective effect sizes of SNPs on FG, HbA1c, and diabetes as the independent variables with the corresponding effects sizes for CAD as the dependent variables (Figure 3). SNPs associated with HbA1C and diabetes were significantly associated with an increased risk of CAD (odds ratio, OR: 1.53 per % increase in HbA1c, 95% Confidence Interval (CI): 1.14– 2.05; P ¼ 0.023, and OR: 1.57, 95% CI: 1.16–2.05; P ¼ 0.008, respectively) while SNPs associated with FG were not associated with risk of CAD (P . 0.05; Figure 3). When regression models for HbA1C and diabetes were adjusted for the effects of SNPs on other CAD risk factors (i.e. LDL, HDL, TC, TG, and BMI), only SNPs associated with diabetes remained significantly associated with CAD (OR: 1.63, 95% CI: 1.23 –2.07; P ¼ 0.002) while association with HbA1c (OR:1.66, 95% CI: 0.44–6.35; P ¼ 0.510) and FG (OR: 1.16, 95% CI: 0.94–1.42; P ¼ 0.185) were non-significant. Comparison with literature estimates from observational studies To date, the largest prospective meta-analysis to assess the effects of glucose traits and diabetes on the risk of CVD is the Emerging Risk Factor Collaboration (ERFC).1,2 The authors reported that diabetes was associated with an increased risk of CAD (hazard ratio (HR): 2.00, 95% CI: 1.83–2.19) in 698 782 individuals from 102 prospective studies. They also observed similar trends for FG (HR: 1.02 per mmol/L, 95% CI: 1.02 –1.03), and HbA1C (HR: 1.43 per %, 95% CI: 1.07 –1.91) in 294 998 individuals without diabetes or CAD from 73 prospective studies. We sought to determine whether the causal effects of glycaemia and diabetes on the risk of CAD estimated using Mendelian randomization were consistent with the aforementioned estimates obtained from the ERFC (Figure 4). We observed that the causal effects of diabetes on the risk of CAD derived from our Mendelian randomization was similar to that of the risk estimates obtained from the ERFC (P for difference ¼ 0.161). There were also no statistical differences for glucose traits SNPs and the corresponding literature estimates (P for difference .0.05 for all). Using reported risk estimates from observational studies, we estimated power to detect a genetic association between CAD and diabetes at 100%, 72.2% for HbA1C, and 5.6% for FG. Effect of gene function on coronary artery disease risk estimates We also explored whether the causal association of diabetes with CAD differed between sets of genes known to influence either Downloaded from by guest on April 20, 2015 Results Page 4 of 9 S. Ross et al. Figure 3 Genetic estimates of association of diabetes, glycated haemoglobin, and fasting glucose with risk of coronary artery disease. Analyses were adjusted for the potential pleiotropic effects of low-density lipoprotein, high-density lipoprotein, total cholesterol, triglyceride, and body mass index. Downloaded from by guest on April 20, 2015 Figure 2 Effect of SNPs associated with levels of fasting glucose, glycated haemoglobin, and diabetes on the risk of coronary artery disease. Each black dot represents an SNP associated with a glycaemic trait (fasting glucose, glycated hemoglobin or diabetes) with a P , 5 × 1028. The association of each SNP with coronary artery disease (b-value) is represented by the y-axis while association with glycaemic trait is represented by the x-axis. The blue line illustrates regression of coronary artery disease effects on glycaemic effects. The P-value for the association of fasting glucose SNPs with the risk of coronary artery disease was 0.102, glycated haemoglobin SNPs with the risk of coronary artery disease was 0.023, diabetes SNPs with the risk of coronary artery disease was 0.008. Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes Page 5 of 9 Figure 4 Comparison of estimated effects of glycaemia and diabetes on coronary artery disease derived from genetic analysis with estimates from observational studies. Observational estimates represent estimates obtained from the Emerging Risk Factor Collaboration.1,2 b-cell function or insulin resistance. We thus stratified diabetes SNPs according to their known biological function, namely: ‘b-cell dysfunction’ or ‘insulin resistance’ (Figure 5). Among the 59 SNPs associated with diabetes, there were 26 loci associated with b-cell dysfunction and 11 loci associated with insulin resistance. Loci influencing b-cell dysfunction and insulin resistance were both associated with an increased risk in CAD (OR 1.83, 95% CI: 1.19–2.62; P ¼ 0.015 and OR: 2.35, 95% CI: 1.46–3.53; P ¼ 0.01, respectively). Discussion Using genetic information from 59 SNPs with known association with diabetes, our Mendelian randomization analysis supports a causal role of diabetes for CAD. We demonstrated that SNPs associated with HbA1C and diabetes were associated with an increased risk of CAD, which is consistent with findings from large observational studies.1,2 Furthermore, consistent results were obtained when restricting the analysis to genes affecting either b-cell dysfunction or insulin resistance, suggesting that the therapeutic interventions that act through these different pathways have the potential to reduce CAD irrespective of their mechanism of action. Although Downloaded from by guest on April 20, 2015 Figure 5 Subgroup analysis of loci influencing b-cell dysfunction or insulin resistance on risk of coronary artery disease. our estimates of the effect of diabetes on CAD appeared to be more modest in comparison with observational studies1,2 this may be explained by residual confounding or bias among these studies. SNPs associated with HbA1C were also associated with an increased risk of CAD but the effect was attenuated after adjustment for other CAD risk factors. SNPs associated with FG were not associated with the risk of CAD but we had limited power to detect an effect for FG (5.6%). These analyses have several strengths. First, the random allocation of genetic variants acts to reduce the potential effects of confounding and reverse-causation observed in epidemiological studies. Furthermore, unlike other Mendelian randomization analyses that have assessed the effect of glucose traits on the risk of CVD outcomes,26 we were able to control for genetic effects on other CAD risk factors such as blood lipids, blood pressure, and obesity. We also had very robust estimates from the CARDIOGRAMplusC4D, DIAGRAM, GIANT, GLGC, and MAGIC consortia which collectively included a total of 681 875 individuals. The differences we observed between carriers and non-carriers of genetic variants represent lifelong effects on HbA1C and diabetes. Indeed, in the UKPDS trial, the authors reported a non-significant reduction in the risk of MI among patients randomized to intensive or conventional glucoselowering strategies.27 In addition, after 8.5 years of post-trial observations, those originally randomized to the active arm experienced a 15% reduction in MI (P ¼ 0.01) and 13% reduction in all-cause mortality (P ¼ 0.007).28 Similar trends were also observed in the DCCT/ EDIC trial.29 Thus, the genetic properties of our analysis provide further support that long-term treatment with glucose-lowering agents may be beneficial. Also, loci involved in b-cell dysfunction and insulin resistance were both associated with CAD. While the causal effect of diabetes on CAD using all SNPs was nominally lower than in each individual subgroup, these differences may be due to fewer SNPs in each subgroup with wider confidence intervals and the exclusion of SNPs with unknown function. Taken together, these results suggest that long-term treatment with glucose-lowering agents, regardless of the mechanism of action, may be required Page 6 of 9 Supplementary material Supplementary material is available at European Heart Journal online. Acknowledgements We are thankful to all the participants having agreed to contribute to this project, and to the DIAGRAM, CARDIoGRAMplusC4D, MAGIC, GIANT, and GLCC consortia for making their data available. Funding This work was supported by the following grants: J.E., receiving support from Canada Research Chair in Cardiovascular Medicine; S.S.A. received support from Canada Research Chair in Ethnic Diversity and Cardiovascular Disease, Eli Lilly Canada/May Cohen Chair in Women’s Health, and Heart and Stroke Foundation of Ontario/Michael G. DeGroote Chair in Population Health Research; H.C.G. received support from Population Health Institute Chair in Diabetes Research and Care; G.P. received support from Canada Research Chair in Genetic and Molecular Epidemiology, CISCOProfessorship in Integrated Health Systems. Conflict of interest: J.E. received consulting fees, grant support, and lecture fees from Sanofi-Aventis, Bristol-Myers Squibb, and AstraZeneca, consulting fees and grant support from Novartis, and consulting fees and lecture fees from Eli Lilly; S.S.A. received lecture fees from Bristol-Myers Squibb; H.G.C. received honoraria for consulting and academic presentations from Sanofi-Aventis, Novo Nordisk, and Eli Lilly; and G.P. received consulting fees from Sanofi-Aventis and Bristol-Myers Squibb. References 1. Sarwar N, Gao P, Seshasai SR, Gobin R, Kaptoge S, Di AE, Ingelsson E, Lawlor DA, Selvin E, Stampfer M, Stehouwer CD, Lewington S, Pennells L, Thompson A, Sattar N, White IR, Ray KK, Danesh J. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet 2010;375:2215 – 2222. 2. Di AE, Gao P, Khan H, Butterworth AS, Wormser D, Kaptoge S, Kondapally Seshasai SR, Thompson A, Sarwar N, Willeit P, Ridker PM, Barr EL, Khaw KT, Psaty BM, Brenner H, Balkau B, Dekker JM, Lawlor DA, Daimon M, Willeit J, Njolstad I, Nissinen A, Brunner EJ, Kuller LH, Price JF, Sundstrom J, Knuiman MW, Feskens EJ, Verschuren WM, Wald N, Bakker SJ, Whincup PH, Ford I, Goldbourt U, Gomez-de-la-Camara A, Gallacher J, Simons LA, Rosengren A, Sutherland SE, Bjorkelund C, Blazer DG, Wassertheil-Smoller S, Onat A, Marin IA, Casiglia E, Jukema JW, Simpson LM, Giampaoli S, Nordestgaard BG, Selmer R, Wennberg P, Kauhanen J, Salonen JT, Dankner R, Barrett-Connor E, Kavousi M, Gudnason V, Evans D, Wallace RB, Cushman M, D’Agostino RB Sr, Umans JG, Kiyohara Y, Nakagawa H, Sato S, Gillum RF, Folsom AR, van der Schouw YT, Moons KG, Griffin SJ, Sattar N, Wareham NJ, Selvin E, Thompson SG, Danesh J. Glycated hemoglobin measurement and prediction of cardiovascular disease. JAMA 2014;311:1225 –1233. 3. Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Bigger JT, Buse JB, Cushman WC, Genuth S, Ismail-Beigi F, Grimm RH Jr, Probstfield JL, Simons-Morton DG, Friedewald WT. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008;358:2545 –2559. 4. Patel A, MacMahon S, Chalmers J, Neal B, Billot L, Woodward M, Marre M, Cooper M, Glasziou P, Grobbee D, Hamet P, Harrap S, Heller S, Liu L, Mancia G, Mogensen CE, Pan C, Poulter N, Rodgers A, Williams B, Bompoint S, de Galan BE, Joshi R, Travert F. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560 –2572. 5. Gerstein HC, Bosch J, Dagenais GR, Diaz R, Jung H, Maggioni AP, Pogue J, Probstfield J, Ramachandran A, Riddle MC, Ryden LE, Yusuf S. Basal insulin and cardiovascular and other outcomes in dysglycemia. N Engl J Med 2012;367: 319 –328. 6. White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, Perez AT, Fleck PR, Mehta CR, Kupfer S, Wilson C, Cushman WC, Zannad F. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 2013;369: 1327 –1335. 7. Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman P, Frederich R, Wiviott SD, Hoffman EB, Cavender MA, Udell JA, Desai NR, Mosenzon O, McGuire DK, Ray KK, Leiter LA, Raz I. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013;369: 1317 –1326. 8. Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, Lafont S, Bergeonneau C, Kassai B, Erpeldinger S, Wright JM, Gueyffier F, Cornu C. Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials. BMJ 2011;343:d4169. 9. Ray KK, Seshasai SR, Wijesuriya S, Sivakumaran R, Nethercott S, Preiss D, Erqou S, Sattar N. Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: a meta-analysis of randomised controlled trials. Lancet 2009;373:1765 –1772. 10. Turnbull FM, Abraira C, Anderson RJ, Byington RP, Chalmers JP, Duckworth WC, Evans GW, Gerstein HC, Holman RR, Moritz TE, Neal BC, Ninomiya T, Patel AA, Paul SK, Travert F, Woodward M. Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia 2009;52:2288 –2298. 11. Gerstein HC, Miller ME, Ismail-Beigi F, Largay J, McDonald C, Lochnan HA, Booth GL. Effects of intensive glycaemic control on ischaemic heart disease: analysis of data from the randomised, controlled ACCORD trial. Lancet 2014;384: 1936 –1941. 12. Smith GD, Ebrahim S. ‘Mendelian randomization’: can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol 2003;32: 1–22. 13. Timpson NJ, Wade KH, Smith GD. Mendelian randomization: application to cardiovascular disease. Curr Hypertens Rep 2012;14:29– 37. 14. Do R, Willer CJ, Schmidt EM, Sengupta S, Gao C, Peloso GM, Gustafsson S, Kanoni S, Ganna A, Chen J, Buchkovich ML, Mora S, Beckmann JS, Bragg-Gresham JL, Chang HY, Demirkan A, Den Hertog HM, Donnelly LA, Ehret GB, Esko T, Feitosa MF, Ferreira T, Fischer K, Fontanillas P, Fraser RM, Freitag DF, Gurdasani D, Heikkila K, Hypponen E, Isaacs A, Jackson AU, Johansson A, Johnson T, Kaakinen M, Kettunen J, Kleber ME, Li X, Luan J, Lyytikainen LP, Magnusson PK, Mangino M, Mihailov E, Montasser ME, Muller-Nurasyid M, Nolte IM, O’Connell JR, Palmer CD, Perola M, Petersen AK, Sanna S, Saxena R, Service SK, Shah S, Shungin D, Sidore C, Song C, Strawbridge RJ, Surakka I, Tanaka T, Teslovich TM, Thorleifsson G, Van den Herik EG, Voight BF, Volcik KA, Waite LL, Wong A, Wu Y, Zhang W, Absher D, Asiki G, Barroso I, Been LF, Downloaded from by guest on April 20, 2015 before the effects of glycaemic intervention on CVD events may be observed. There are several limitations in our study. First, the definition of diabetes used in the DIAGRAM consortium was specific to each cohort, which might introduce heterogeneity into results. Second, estimates obtained from the DIAGRAM and CARDIOGRAMplusC4D consortia consist of both incident and prevalent cases from prospective and case –control studies. Third, owing to a lack of genetic data, we were only able to explore the genetic effect of glucose traits and diabetes in predominantly European populations and we were also unable to account for other confounders that might influence the effect of SNPs associated with glycaemia traits and diabetes on the risk of CAD, such as smoking and waist-to-hip ratio. Fourth, due to the lack of statistical power, we were limited in our ability to evaluate associations with FG. Fifth, we were unable to assess whether there was a non-linear trend for glycaemia traits and the risk of CAD using Mendelian randomization since we did not have individual level data.30 Finally, we were not able to assess the mechanism of action for all SNPs included in this analysis owing to a lack of functional data in the literature. In summary, our genetic analysis provides further insight into the causal role of glucose levels, diabetes, and the risk of CAD. Our results support that diabetes has an independent and causal effect on the risk of major cardiovascular events. Thus improved glycaemic control among diabetic patients and prevention of diabetes may reduce the risk of CAD outcomes. Our results emphasize the need to further explore the benefits of long-term glucose lowering on CAD. S. Ross et al. Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes Bennett AJ, Bergmann S, Bochud M, Boerwinkle E, Bonnefond A, Bonnycastle LL, Borch-Johnsen K, Bottcher Y, Brunner E, Bumpstead SJ, Charpentier G, Chen YD, Chines P, Clarke R, Coin LJ, Cooper MN, Cornelis M, Crawford G, Crisponi L, Day IN, de Geus EJ, Delplanque J, Dina C, Erdos MR, Fedson AC, Fischer-Rosinsky A, Forouhi NG, Fox CS, Frants R, Franzosi MG, Galan P, Goodarzi MO, Graessler J, Groves CJ, Grundy S, Gwilliam R, Gyllensten U, Hadjadj S, Hallmans G, Hammond N, Han X, Hartikainen AL, Hassanali N, Hayward C, Heath SC, Hercberg S, Herder C, Hicks AA, Hillman DR, Hingorani AD, Hofman A, Hui J, Hung J, Isomaa B, Johnson PR, Jorgensen T, Jula A, Kaakinen M, Kaprio J, Kesaniemi YA, Kivimaki M, Knight B, Koskinen S, Kovacs P, Kyvik KO, Lathrop GM, Lawlor DA, Le BO, Lecoeur C, Li Y, Lyssenko V, Mahley R, Mangino M, Manning AK, Martinez-Larrad MT, McAteer JB, McCulloch LJ, McPherson R, Meisinger C, Melzer D, Meyre D, Mitchell BD, Morken MA, Mukherjee S, Naitza S, Narisu N, Neville MJ, Oostra BA, Orru M, Pakyz R, Palmer CN, Paolisso G, Pattaro C, Pearson D, Peden JF, Pedersen NL, Perola M, Pfeiffer AF, Pichler I, Polasek O, Posthuma D, Potter SC, Pouta A, Province MA, Psaty BM, Rathmann W, Rayner NW, Rice K, Ripatti S, Rivadeneira F, Roden M, Rolandsson O, Sandbaek A, Sandhu M, Sanna S, Sayer AA, Scheet P, Scott LJ, Seedorf U, Sharp SJ, Shields B, Sigurethsson G, Sijbrands EJ, Silveira A, Simpson L, Singleton A, Smith NL, Sovio U, Swift A, Syddall H, Syvanen AC, Tanaka T, Thorand B, Tichet J, Tonjes A, Tuomi T, Uitterlinden AG, van Dijk KW, van Hoek M, Varma D, Visvikis-Siest S, Vitart V, Vogelzangs N, Waeber G, Wagner PJ, Walley A, Walters GB, Ward KL, Watkins H, Weedon MN, Wild SH, Willemsen G, Witteman JC, Yarnell JW, Zeggini E, Zelenika D, Zethelius B, Zhai G, Zhao JH, Zillikens MC, Borecki IB, Loos RJ, Meneton P, Magnusson PK, Nathan DM, Williams GH, Hattersley AT, Silander K, Salomaa V, Smith GD, Bornstein SR, Schwarz P, Spranger J, Karpe F, Shuldiner AR, Cooper C, Dedoussis GV, Serrano-Rios M, Morris AD, Lind L, Palmer LJ, Hu FB, Franks PW, Ebrahim S, Marmot M, Kao WH, Pankow JS, Sampson MJ, Kuusisto J, Laakso M, Hansen T, Pedersen O, Pramstaller PP. New genetic loci implicated in fasting glucose homeostasis and their impact on type 2 diabetes risk. Nat Genet 2010;42:105–116. 17. Soranzo N, Sanna S, Wheeler E, Gieger C, Radke D, Dupuis J, Bouatia-Naji N, Langenberg C, Prokopenko I, Stolerman E, Sandhu MS, Heeney MM, Devaney JM, Reilly MP, Ricketts SL, Stewart AF, Voight BF, Willenborg C, Wright B, Altshuler D, Arking D, Balkau B, Barnes D, Boerwinkle E, Bohm B, Bonnefond A, Bonnycastle LL, Boomsma DI, Bornstein SR, Bottcher Y, Bumpstead S, Burnett-Miller MS, Campbell H, Cao A, Chambers J, Clark R, Collins FS, Coresh J, de Geus EJ, Dei M, Deloukas P, Doring A, Egan JM, Elosua R, Ferrucci L, Forouhi N, Fox CS, Franklin C, Franzosi MG, Gallina S, Goel A, Graessler J, Grallert H, Greinacher A, Hadley D, Hall A, Hamsten A, Hayward C, Heath S, Herder C, Homuth G, Hottenga JJ, Hunter-Merrill R, Illig T, Jackson AU, Jula A, Kleber M, Knouff CW, Kong A, Kooner J, Kottgen A, Kovacs P, Krohn K, Kuhnel B, Kuusisto J, Laakso M, Lathrop M, Lecoeur C, Li M, Li M, Loos RJ, Luan J, Lyssenko V, Magi R, Magnusson PK, Malarstig A, Mangino M, Martinez-Larrad MT, Marz W, McArdle WL, McPherson R, Meisinger C, Meitinger T, Melander O, Mohlke KL, Mooser VE, Morken MA, Narisu N, Nathan DM, Nauck M, O’Donnell C, Oexle K, Olla N, Pankow JS, Payne F, Peden JF, Pedersen NL, Peltonen L, Perola M, Polasek O, Porcu E, Rader DJ, Rathmann W, Ripatti S, Rocheleau G, Roden M, Rudan I, Salomaa V, Saxena R, Schlessinger D, Schunkert H, Schwarz P, Seedorf U, Selvin E, Serrano-Rios M, Shrader P, Silveira A, Siscovick D, Song K, Spector TD, Stefansson K, Steinthorsdottir V, Strachan DP, Strawbridge R, Stumvoll M, Surakka I, Swift AJ, Tanaka T, Teumer A, Thorleifsson G, Thorsteinsdottir U, Tonjes A, Usala G, Vitart V, Volzke H, Wallaschofski H, Waterworth DM, Watkins H, Wichmann HE, Wild SH, Willemsen G, Williams GH, Wilson JF, Winkelmann J, Wright AF, Zabena C, Zhao JH, Epstein SE, Erdmann J, Hakonarson HH, Kathiresan S, Khaw KT, Roberts R, Samani NJ, Fleming MD, Sladek R, Abecasis G, Boehnke M, Froguel P, Groop L, McCarthy MI, Kao WH, Florez JC, Uda M, Wareham NJ, Barroso I, Meigs JB. Common variants at 10 genomic loci influence hemoglobin A(1)(C) levels via glycemic and nonglycemic pathways. Diabetes 2010;59:3229 –3239. 18. Morris AP, Voight BF, Teslovich TM, Ferreira T, Segre AV, Steinthorsdottir V, Strawbridge RJ, Khan H, Grallert H, Mahajan A, Prokopenko I, Kang HM, Dina C, Esko T, Fraser RM, Kanoni S, Kumar A, Lagou V, Langenberg C, Luan J, Lindgren CM, Muller-Nurasyid M, Pechlivanis S, Rayner NW, Scott LJ, Wiltshire S, Yengo L, Kinnunen L, Rossin EJ, Raychaudhuri S, Johnson AD, Dimas AS, Loos RJ, Vedantam S, Chen H, Florez JC, Fox C, Liu CT, Rybin D, Couper DJ, Kao WH, Li M, Cornelis MC, Kraft P, Sun Q, van Dam RM, Stringham HM, Chines PS, Fischer K, Fontanillas P, Holmen OL, Hunt SE, Jackson AU, Kong A, Lawrence R, Meyer J, Perry JR, Platou CG, Potter S, Rehnberg E, Robertson N, Sivapalaratnam S, Stancakova A, Stirrups K, Thorleifsson G, Tikkanen E, Wood AR, Almgren P, Atalay M, Benediktsson R, Bonnycastle LL, Burtt N, Carey J, Charpentier G, Crenshaw AT, Doney AS, Dorkhan M, Edkins S, Emilsson V, Eury E, Forsen T, Gertow K, Gigante B, Grant GB, Groves CJ, Guiducci C, Herder C, Hreidarsson AB, Hui J, James A, Jonsson A, Rathmann W, Downloaded from by guest on April 20, 2015 Bolton JL, Bonnycastle LL, Brambilla P, Burnett MS, Cesana G, Dimitriou M, Doney AS, Doring A, Elliott P, Epstein SE, Eyjolfsson GI, Gigante B, Goodarzi MO, Grallert H, Gravito ML, Groves CJ, Hallmans G, Hartikainen AL, Hayward C, Hernandez D, Hicks AA, Holm H, Hung YJ, Illig T, Jones MR, Kaleebu P, Kastelein JJ, Khaw KT, Kim E, Klopp N, Komulainen P, Kumari M, Langenberg C, Lehtimaki T, Lin SY, Lindstrom J, Loos RJ, Mach F, McArdle WL, Meisinger C, Mitchell BD, Muller G, Nagaraja R, Narisu N, Nieminen TV, Nsubuga RN, Olafsson I, Ong KK, Palotie A, Papamarkou T, Pomilla C, Pouta A, Rader DJ, Reilly MP, Ridker PM, Rivadeneira F, Rudan I, Ruokonen A, Samani N, Scharnagl H, Seeley J, Silander K, Stancakova A, Stirrups K, Swift AJ, Tiret L, Uitterlinden AG, van Pelt LJ, Vedantam S, Wainwright N, Wijmenga C, Wild SH, Willemsen G, Wilsgaard T, Wilson JF, Young EH, Zhao JH, Adair LS, Arveiler D, Assimes TL, Bandinelli S, Bennett F, Bochud M, Boehm BO, Boomsma DI, Borecki IB, Bornstein SR, Bovet P, Burnier M, Campbell H, Chakravarti A, Chambers JC, Chen YD, Collins FS, Cooper RS, Danesh J, Dedoussis G, de Faire U, Feranil AB, Ferrieres J, Ferrucci L, Freimer NB, Gieger C, Groop LC, Gudnason V, Gyllensten U, Hamsten A, Harris TB, Hingorani A, Hirschhorn JN, Hofman A, Hovingh GK, Hsiung CA, Humphries SE, Hunt SC, Hveem K, Iribarren C, Jarvelin MR, Jula A, Kahonen M, Kaprio J, Kesaniemi A, Kivimaki M, Kooner JS, Koudstaal PJ, Krauss RM, Kuh D, Kuusisto J, Kyvik KO, Laakso M, Lakka TA, Lind L, Lindgren CM, Martin NG, Marz W, McCarthy MI, McKenzie CA, Meneton P, Metspalu A, Moilanen L, Morris AD, Munroe PB, Njolstad I, Pedersen NL, Power C, Pramstaller PP, Price JF, Psaty BM, Quertermous T, Rauramaa R, Saleheen D, Salomaa V, Sanghera DK, Saramies J, Schwarz PE, Sheu WH, Shuldiner AR, Siegbahn A, Spector TD, Stefansson K, Strachan DP, Tayo BO, Tremoli E, Tuomilehto J, Uusitupa M, van Duijn CM, Vollenweider P, Wallentin L, Wareham NJ, Whitfield JB, Wolffenbuttel BH, Altshuler D, Ordovas JM, Boerwinkle E, Palmer CN, Thorsteinsdottir U, Chasman DI, Rotter JI, Franks PW, Ripatti S, Cupples LA, Sandhu MS, Rich SS. Common variants associated with plasma triglycerides and risk for coronary artery disease. Nat Genet 2013;45: 1345– 1352. 15. Scott RA, Lagou V, Welch RP, Wheeler E, Montasser ME, Luan J, Magi R, Strawbridge RJ, Rehnberg E, Gustafsson S, Kanoni S, Rasmussen-Torvik LJ, Yengo L, Lecoeur C, Shungin D, Sanna S, Sidore C, Johnson PC, Jukema JW, Johnson T, Mahajan A, Verweij N, Thorleifsson G, Hottenga JJ, Shah S, Smith AV, Sennblad B, Gieger C, Salo P, Perola M, Timpson NJ, Evans DM, Pourcain BS, Wu Y, Andrews JS, Hui J, Bielak LF, Zhao W, Horikoshi M, Navarro P, Isaacs A, O’Connell JR, Stirrups K, Vitart V, Hayward C, Esko T, Mihailov E, Fraser RM, Fall T, Voight BF, Raychaudhuri S, Chen H, Lindgren CM, Morris AP, Rayner NW, Robertson N, Rybin D, Liu CT, Beckmann JS, Willems SM, Chines PS, Jackson AU, Kang HM, Stringham HM, Song K, Tanaka T, Peden JF, Goel A, Hicks AA, An P, Muller-Nurasyid M, Franco-Cereceda A, Folkersen L, Marullo L, Jansen H, Oldehinkel AJ, Bruinenberg M, Pankow JS, North KE, Forouhi NG, Loos RJ, Edkins S, Varga TV, Hallmans G, Oksa H, Antonella M, Nagaraja R, Trompet S, Ford I, Bakker SJ, Kong A, Kumari M, Gigante B, Herder C, Munroe PB, Caulfield M, Antti J, Mangino M, Small K, Miljkovic I, Liu Y, Atalay M, Kiess W, James AL, Rivadeneira F, Uitterlinden AG, Palmer CN, Doney AS, Willemsen G, Smit JH, Campbell S, Polasek O, Bonnycastle LL, Hercberg S, Dimitriou M, Bolton JL, Fowkes GR, Kovacs P, Lindstrom J, Zemunik T, Bandinelli S, Wild SH, Basart HV, Rathmann W, Grallert H, Maerz W, Kleber ME, Boehm BO, Peters A, Pramstaller PP, Province MA, Borecki IB, Hastie ND, Rudan I, Campbell H, Watkins H, Farrall M, Stumvoll M, Ferrucci L, Waterworth DM, Bergman RN, Collins FS, Tuomilehto J, Watanabe RM, de Geus EJ, Penninx BW, Hofman A, Oostra BA, Psaty BM, Vollenweider P, Wilson JF, Wright AF, Hovingh GK, Metspalu A, Uusitupa M, Magnusson PK, Kyvik KO, Kaprio J, Price JF, Dedoussis GV, Deloukas P, Meneton P, Lind L, Boehnke M, Shuldiner AR, van Duijn CM, Morris AD, Toenjes A, Peyser PA, Beilby JP, Korner A, Kuusisto J, Laakso M, Bornstein SR, Schwarz PE, Lakka TA, Rauramaa R, Adair LS, Smith GD, Spector TD, Illig T, de Faire U, Hamsten A, Gudnason V, Kivimaki M, Hingorani A, Keinanen-Kiukaanniemi SM, Saaristo TE, Boomsma DI, Stefansson K, van der Harst P, Dupuis J, Pedersen NL, Sattar N, Harris TB, Cucca F, Ripatti S, Salomaa V, Mohlke KL, Balkau B, Froguel P, Pouta A, Jarvelin MR, Wareham NJ, Bouatia-Naji N, McCarthy MI, Franks PW, Meigs JB, Teslovich TM, Florez JC, Langenberg C, Ingelsson E, Prokopenko I, Barroso I. Large-scale association analyses identify new loci influencing glycemic traits and provide insight into the underlying biological pathways. Nat Genet 2012;44:991–1005. 16. Dupuis J, Langenberg C, Prokopenko I, Saxena R, Soranzo N, Jackson AU, Wheeler E, Glazer NL, Bouatia-Naji N, Gloyn AL, Lindgren CM, Magi R, Morris AP, Randall J, Johnson T, Elliott P, Rybin D, Thorleifsson G, Steinthorsdottir V, Henneman P, Grallert H, Dehghan A, Hottenga JJ, Franklin CS, Navarro P, Song K, Goel A, Perry JR, Egan JM, Lajunen T, Grarup N, Sparso T, Doney A, Voight BF, Stringham HM, Li M, Kanoni S, Shrader P, Cavalcanti-Proenca C, Kumari M, Qi L, Timpson NJ, Gieger C, Zabena C, Rocheleau G, Ingelsson E, An P, O’Connell J, Luan J, Elliott A, McCarroll SA, Payne F, Roccasecca RM, Pattou F, Sethupathy P, Ardlie K, Ariyurek Y, Balkau B, Barter P, Beilby JP, Ben-Shlomo Y, Benediktsson R, Page 7 of 9 Page 8 of 9 Roberts R, Thorsteinsdottir U, O’Donnell CJ, McPherson R, Erdmann J, Samani NJ. Large-scale association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat Genet 2011;43:333 –338. 21. Willer CJ, Schmidt EM, Sengupta S, Peloso GM, Gustafsson S, Kanoni S,Ganna A, Chen J, Buchkovich ML, Mora S, Beckmann JS, Bragg-Gresham JL, Chang HY, Demirkan A, Den Hertog HM, Do R, Donnelly LA, Ehret GB, Esko T, Feitosa MF, Ferreira T, Fischer K, Fontanillas P, Fraser RM, Freitag DF, Gurdasani D, Heikkila K, Hypponen E, Isaacs A, Jackson AU, Johansson A, Johnson T, Kaakinen M, Kettunen J, Kleber ME, Li X, Luan J, Lyytikainen LP, Magnusson PK, Mangino M, Mihailov E, Montasser ME, Muller-Nurasyid M, Nolte IM, O’Connell JR, Palmer CD, Perola M, Petersen AK, Sanna S, Saxena R, Service SK, Shah S, Shungin D, Sidore C, Song C, Strawbridge RJ, Surakka I, Tanaka T, Teslovich TM, Thorleifsson G, Van den Herik EG, Voight BF, Volcik KA, Waite LL, Wong A, Wu Y, Zhang W, Absher D, Asiki G, Barroso I, Been LF, Bolton JL, Bonnycastle LL, Brambilla P, Burnett MS, Cesana G, Dimitriou M, Doney AS, Doring A, Elliott P, Epstein SE, Eyjolfsson GI, Gigante B, Goodarzi MO, Grallert H, Gravito ML, Groves CJ, Hallmans G, Hartikainen AL, Hayward C, Hernandez D, Hicks AA, Holm H, Hung YJ, Illig T, Jones MR, Kaleebu P, Kastelein JJ, Khaw KT, Kim E, Klopp N, Komulainen P, Kumari M, Langenberg C, Lehtimaki T, Lin SY, Lindstrom J, Loos RJ, Mach F, McArdle WL, Meisinger C, Mitchell BD, Muller G, Nagaraja R, Narisu N, Nieminen TV, Nsubuga RN, Olafsson I, Ong KK, Palotie A, Papamarkou T, Pomilla C, Pouta A, Rader DJ, Reilly MP, Ridker PM, Rivadeneira F, Rudan I, Ruokonen A, Samani N, Scharnagl H, Seeley J, Silander K, Stancakova A, Stirrups K, Swift AJ, Tiret L, Uitterlinden AG, van Pelt LJ, Vedantam S, Wainwright N, Wijmenga C, Wild SH, Willemsen G, Wilsgaard T, Wilson JF, Young EH, Zhao JH, Adair LS, Arveiler D, Assimes TL, Bandinelli S, Bennett F, Bochud M, Boehm BO, Boomsma DI, Borecki IB, Bornstein SR, Bovet P, Burnier M, Campbell H, Chakravarti A, Chambers JC, Chen YD, Collins FS, Cooper RS, Danesh J, Dedoussis G, de Faire U, Feranil AB, Ferrieres J, Ferrucci L, Freimer NB, Gieger C, Groop LC, Gudnason V, Gyllensten U, Hamsten A, Harris TB, Hingorani A, Hirschhorn JN, Hofman A, Hovingh GK, Hsiung CA, Humphries SE, Hunt SC, Hveem K, Iribarren C, Jarvelin MR, Jula A, Kahonen M, Kaprio J, Kesaniemi A, Kivimaki M, Kooner JS, Koudstaal PJ, Krauss RM, Kuh D, Kuusisto J, Kyvik KO, Laakso M, Lakka TA, Lind L, Lindgren CM, Martin NG, Marz W, McCarthy MI, McKenzie CA, Meneton P, Metspalu A, Moilanen L, Morris AD, Munroe PB, Njolstad I, Pedersen NL, Power C, Pramstaller PP, Price JF, Psaty BM, Quertermous T, Rauramaa R, Saleheen D, Salomaa V, Sanghera DK, Saramies J, Schwarz PE, Sheu WH, Shuldiner AR, Siegbahn A, Spector TD, Stefansson K, Strachan DP, Tayo BO, Tremoli E, Tuomilehto J, Uusitupa M, van Duijn CM, Vollenweider P, Wallentin L, Wareham NJ, Whitfield JB, Wolffenbuttel BH, Ordovas JM, Boerwinkle E, Palmer CN, Thorsteinsdottir U, Chasman DI, Rotter JI, Franks PW, Ripatti S, Cupples LA, Sandhu MS, Rich SS, Boehnke M, Deloukas P. Discovery and refinement of loci associated with lipid levels. Nat Genet 2013;45: 1274–1283. 22. Speliotes EK, Willer CJ, Berndt SI, Monda KL, Thorleifsson G, Jackson AU, Lango AH, Lindgren CM, Luan J, Magi R, Randall JC, Vedantam S, Winkler TW, Qi L, Workalemahu T, Heid IM, Steinthorsdottir V, Stringham HM, Weedon MN, Wheeler E, Wood AR, Ferreira T, Weyant RJ, Segre AV, Estrada K, Liang L, Nemesh J, Park JH, Gustafsson S, Kilpelainen TO, Yang J, Bouatia-Naji N, Esko T, Feitosa MF, Kutalik Z, Mangino M, Raychaudhuri S, Scherag A, Smith AV, Welch R, Zhao JH, Aben KK, Absher DM, Amin N, Dixon AL, Fisher E, Glazer NL, Goddard ME, Heard-Costa NL, Hoesel V, Hottenga JJ, Johansson A, Johnson T, Ketkar S, Lamina C, Li S, Moffatt MF, Myers RH, Narisu N, Perry JR, Peters MJ, Preuss M, Ripatti S, Rivadeneira F, Sandholt C, Scott LJ, Timpson NJ, Tyrer JP, van Wingerden S, Watanabe RM, White CC, Wiklund F, Barlassina C, Chasman DI, Cooper MN, Jansson JO, Lawrence RW, Pellikka N, Prokopenko I, Shi J, Thiering E, Alavere H, Alibrandi MT, Almgren P, Arnold AM, Aspelund T, Atwood LD, Balkau B, Balmforth AJ, Bennett AJ, Ben-Shlomo Y, Bergman RN, Bergmann S, Biebermann H, Blakemore AI, Boes T, Bonnycastle LL, Bornstein SR, Brown MJ, Buchanan TA, Busonero F, Campbell H, Cappuccio FP, Cavalcanti-Proenca C, Chen YD, Chen CM, Chines PS, Clarke R, Coin L, Connell J, Day IN, den Heijer M, Duan J, Ebrahim S, Elliott P, Elosua R, Eiriksdottir G, Erdos MR, Eriksson JG, Facheris MF, Felix SB, Fischer-Posovszky P, Folsom AR, Friedrich N, Freimer NB, Fu M, Gaget S, Gejman PV, Geus EJ, Gieger C, Gjesing AP, Goel A, Goyette P, Grallert H, Grassler J, Greenawalt DM, Groves CJ, Gudnason V, Guiducci C, Hartikainen AL, Hassanali N, Hall AS, Havulinna AS, Hayward C, Heath AC, Hengstenberg C, Hicks AA, Hinney A, Hofman A, Homuth G, Hui J, Igl W, Iribarren C, Isomaa B, Jacobs KB, Jarick I, Jewell E, John U, Jorgensen T, Jousilahti P, Jula A, Kaakinen M, Kajantie E, Kaplan LM, Kathiresan S, Kettunen J, Kinnunen L, Knowles JW, Kolcic I, Konig IR, Koskinen S, Kovacs P, Kuusisto J, Kraft P, Kvaloy K, Laitinen J, Lantieri O, Lanzani C, Launer LJ, Lecoeur C, Lehtimaki T, Lettre G, Liu J, Lokki ML, Lorentzon M, Luben RN, Ludwig B, Manunta P, Marek D, Marre M, Martin NG, McArdle WL, McCarthy A, McKnight B, Meitinger T, Melander O, Meyre D, Midthjell K, Montgomery GW, Morken MA, Morris AP, Mulic R, Ngwa JS, Nelis M, Neville MJ, Nyholt DR, O’Donnell CJ, O’Rahilly S, Ong KK, Oostra B, Pare G, Parker AN, Perola M, Pichler I, Pietilainen KH, Platou CG, Polasek O, Downloaded from by guest on April 20, 2015 Klopp N, Kravic J, Krjutskov K, Langford C, Leander K, Lindholm E, Lobbens S, Mannisto S, Mirza G, Muhleisen TW, Musk B, Parkin M, Rallidis L, Saramies J, Sennblad B, Shah S, Sigurethsson G, Silveira A, Steinbach G, Thorand B, Trakalo J, Veglia F, Wennauer R, Winckler W, Zabaneh D, Campbell H, van Duijn C, Uitterlinden AG, Hofman A, Sijbrands E, Abecasis GR, Owen KR, Zeggini E, Trip MD, Forouhi NG, Syvanen AC, Eriksson JG, Peltonen L, Nothen MM, Balkau B, Palmer CN, Lyssenko V, Tuomi T, Isomaa B, Hunter DJ, Qi L, Shuldiner AR, Roden M, Barroso I, Wilsgaard T, Beilby J, Hovingh K, Price JF, Wilson JF, Rauramaa R, Lakka TA, Lind L, Dedoussis G, Njolstad I, Pedersen NL, Khaw KT, Wareham NJ, Keinanen-Kiukaanniemi SM, Saaristo TE, Korpi-Hyovalti E, Saltevo J, Laakso M, Kuusisto J, Metspalu A, Collins FS, Mohlke KL, Bergman RN, Tuomilehto J, Boehm BO, Gieger C, Hveem K, Cauchi S, Froguel P, Baldassarre D, Tremoli E, Humphries SE, Saleheen D, Danesh J, Ingelsson E, Ripatti S, Salomaa V, Erbel R, Jockel KH, Moebus S, Peters A, Illig T, de Faire U, Hamsten A, Morris AD, Donnelly PJ, Frayling TM, Hattersley AT, Boerwinkle E, Melander O, Kathiresan S, Nilsson PM, Deloukas P, Thorsteinsdottir U, Groop LC, Stefansson K, Hu F, Pankow JS, Dupuis J, Meigs JB, Altshuler D, Boehnke M, McCarthy MI. Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nat Genet 2012;44:981 – 990. 19. Deloukas P, Kanoni S, Willenborg C, Farrall M, Assimes TL, Thompson JR, Ingelsson E, Saleheen D, Erdmann J, Goldstein BA, Stirrups K, Konig IR, Cazier JB, Johansson A, Hall AS, Lee JY, Willer CJ, Chambers JC, Esko T, Folkersen L, Goel A, Grundberg E, Havulinna AS, Ho WK, Hopewell JC, Eriksson N, Kleber ME, Kristiansson K, Lundmark P, Lyytikainen LP, Rafelt S, Shungin D, Strawbridge RJ, Thorleifsson G, Tikkanen E, Van ZN, Voight BF, Waite LL, Zhang W, Ziegler A, Absher D, Altshuler D, Balmforth AJ, Barroso I, Braund PS, Burgdorf C, Claudi-Boehm S, Cox D, Dimitriou M, Do R, Doney AS, El MN, Eriksson P, Fischer K, Fontanillas P, Franco-Cereceda A, Gigante B, Groop L, Gustafsson S, Hager J, Hallmans G, Han BG, Hunt SE, Kang HM, Illig T, Kessler T, Knowles JW, Kolovou G, Kuusisto J, Langenberg C, Langford C, Leander K, Lokki ML, Lundmark A, McCarthy MI, Meisinger C, Melander O, Mihailov E, Maouche S, Morris AD, Muller-Nurasyid M, Nikus K, Peden JF, Rayner NW, Rasheed A, Rosinger S, Rubin D, Rumpf MP, Schafer A, Sivananthan M, Song C, Stewart AF, Tan ST, Thorgeirsson G, van der Schoot CE, Wagner PJ, Wells GA, Wild PS, Yang TP, Amouyel P, Arveiler D, Basart H, Boehnke M, Boerwinkle E, Brambilla P, Cambien F, Cupples AL, de Faire U, Dehghan A, Diemert P, Epstein SE, Evans A, Ferrario MM, Ferrieres J, Gauguier D, Go AS, Goodall AH, Gudnason V, Hazen SL, Holm H, Iribarren C, Jang Y, Kahonen M, Kee F, Kim HS, Klopp N, Koenig W, Kratzer W, Kuulasmaa K, Laakso M, Laaksonen R, Lee JY, Lind L, Ouwehand WH, Parish S, Park JE, Pedersen NL, Peters A, Quertermous T, Rader DJ, Salomaa V, Schadt E, Shah SH, Sinisalo J, Stark K, Stefansson K, Tregouet DA, Virtamo J, Wallentin L, Wareham N, Zimmermann ME, Nieminen MS, Hengstenberg C, Sandhu MS, Pastinen T, Syvanen AC, Hovingh GK, Dedoussis G, Franks PW, Lehtimaki T, Metspalu A, Zalloua PA, Siegbahn A, Schreiber S, Ripatti S, Blankenberg SS, Perola M, Clarke R, Boehm BO, O’Donnell C, Reilly MP, Marz W, Collins R, Kathiresan S, Hamsten A, Kooner JS, Thorsteinsdottir U, Danesh J, Palmer CN, Roberts R, Watkins H, Schunkert H, Samani NJ. Large-scale association analysis identifies new risk loci for coronary artery disease. Nat Genet 2013;45:25 –33. 20. Schunkert H, Konig IR, Kathiresan S, Reilly MP, Assimes TL, Holm H, Preuss M, Stewart AF, Barbalic M, Gieger C, Absher D, Aherrahrou Z, Allayee H, Altshuler D, Anand SS, Andersen K, Anderson JL, Ardissino D, Ball SG, Balmforth AJ, Barnes TA, Becker DM, Becker LC, Berger K, Bis JC, Boekholdt SM, Boerwinkle E, Braund PS, Brown MJ, Burnett MS, Buysschaert I, Carlquist JF, Chen L, Cichon S, Codd V, Davies RW, Dedoussis G, Dehghan A, Demissie S, Devaney JM, Diemert P, Do R, Doering A, Eifert S, Mokhtari NE, Ellis SG, Elosua R, Engert JC, Epstein SE, de Faire U, Fischer M, Folsom AR, Freyer J, Gigante B, Girelli D, Gretarsdottir S, Gudnason V, Gulcher JR, Halperin E, Hammond N, Hazen SL, Hofman A, Horne BD, Illig T, Iribarren C, Jones GT, Jukema JW, Kaiser MA, Kaplan LM, Kastelein JJ, Khaw KT, Knowles JW, Kolovou G, Kong A, Laaksonen R, Lambrechts D, Leander K, Lettre G, Li M, Lieb W, Loley C, Lotery AJ, Mannucci PM, Maouche S, Martinelli N, McKeown PP, Meisinger C, Meitinger T, Melander O, Merlini PA, Mooser V, Morgan T, Muhleisen TW, Muhlestein JB, Munzel T, Musunuru K, Nahrstaedt J, Nelson CP, Nothen MM, Olivieri O, Patel RS, Patterson CC, Peters A, Peyvandi F, Qu L, Quyyumi AA, Rader DJ, Rallidis LS, Rice C, Rosendaal FR, Rubin D, Salomaa V, Sampietro ML, Sandhu MS, Schadt E, Schafer A, Schillert A, Schreiber S, Schrezenmeir J, Schwartz SM, Siscovick DS, Sivananthan M, Sivapalaratnam S, Smith A, Smith TB, Snoep JD, Soranzo N, Spertus JA, Stark K, Stirrups K, Stoll M, Tang WH, Tennstedt S, Thorgeirsson G, Thorleifsson G, Tomaszewski M, Uitterlinden AG, van Rij AM, Voight BF, Wareham NJ, Wells GA, Wichmann HE, Wild PS, Willenborg C, Witteman JC, Wright BJ, Ye S, Zeller T, Ziegler A, Cambien F, Goodall AH, Cupples LA, Quertermous T, Marz W, Hengstenberg C, Blankenberg S, Ouwehand WH, Hall AS, Deloukas P, Thompson JR, Stefansson K, S. Ross et al. Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes Pouta A, Rafelt S, Raitakari O, Rayner NW, Ridderstrale M, Rief W, Ruokonen A, Robertson NR, Rzehak P, Salomaa V, Sanders AR, Sandhu MS, Sanna S, Saramies J, Savolainen MJ, Scherag S, Schipf S, Schreiber S, Schunkert H, Silander K, Sinisalo J, Siscovick DS, Smit JH, Soranzo N, Sovio U, Stephens J, Surakka I, Swift AJ, Tammesoo ML, Tardif JC, Teder-Laving M, Teslovich TM, Thompson JR, Thomson B, Tonjes A, Tuomi T, van Meurs JB, van Ommen GJ. Association analyses of 249,796 individuals reveal 18 new loci associated with body mass index. Nat Genet 2010;42:937–948. 23. Johnson AD, Handsaker RE, Pulit SL, Nizzari MM, O’Donnell CJ, de Bakker PI. SNAP: a web-based tool for identification and annotation of proxy SNPs using HapMap. Bioinformatics 2008;24:2938 – 2939. 24. Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract 2014;103:137 –149. 25. Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ 2003;326:219. Page 9 of 9 26. Benn M, Tybjaerg-Hansen A, McCarthy MI, Jensen GB, Grande P, Nordestgaard BG. Nonfasting glucose, ischemic heart disease, and myocardial infarction: a Mendelian randomization study. J Am Coll Cardiol 2012;59:2356 –2365. 27. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:837–853. 28. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577 –1589. 29. Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, Raskin P, Zinman B. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005;353:2643 – 2653. 30. Silverwood RJ, Holmes MV, Dale CE, Lawlor DA, Whittaker JC, Smith GD, Leon DA, Palmer T, Keating BJ, Zuccolo L, Casas JP, Dudbridge F; Alcohol-ADH1B Consortium. Testing for non-linear causal effects using a binary genotype in a Mendelian randomization study: application to alcohol and cardiovascular traits. Int J Epidemiol 2014;43:1781 – 1790. Downloaded from by guest on April 20, 2015
Scaricare