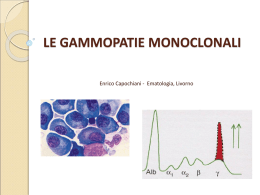
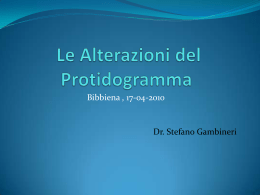
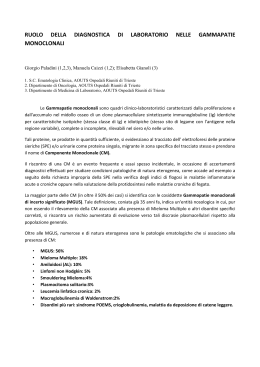
Original article The role of cytokines and adhesion molecules in the evolution of monoclonal gammopathy of undetermined significance into myeloma Saverio Misso1, Bianca Feola1, Marcello D'Onofrio2, Luigi Paesano2, Orlando Antonio Spada3, Lucia Bene3, Vincenzo Mettivier3, Giorgio Fratellanza2, Elio D'Agostino2, Antonio Minerva1, Salvatore Formisano2 Immunoematologia e Medicina Trasfusionale, Ospedale "San Sebastiano", Caserta Immunoematologia e Medicina Trasfusionale, Facoltà di Medicina, Università degli Studi di Napoli "Federico II" 3 2° Dipartimento di Ematologia, Ospedale A. Cardarelli, Napoli 1 2 The aim of this study was to evaluate the influence of some cytokines on the evolution of monoclonal gammopathies. Fifty-one patients with multiple myeloma (MM) divided into 3 groups according to disease stage (MM1, MM2, MM3), 60 with monoclonal gammopathy of undetermined significance (MGUS) and 50 healthy controls (C) were studied. The levels of sCD138 β1, sVCAM-1, IL-13, Fas/APO-1, IL-6, (Syndecan-1), TGF-β β2-microglobulin (β β2-M) and C-reactive protein (CRP) were assayed. Seven of the 60 cases of MGUS (11.6%) evolved into MM3 during the 5-year follow-up; these cases were studied in order to identify any changes in the cytokine network. β2-M and CRP concentrations increased significantly β1, through C, MGUS and the three stages of MM. TGF-β sVCAM-1, Fas/APO-1 and IL-6 levels were significantly higher, while IL-13 concentration was significantly lower, in MGUS and in MM than in C (p<0.001). The level of sCD138 was significantly lower in MGUS than in C and significantly higher in MM than in C (p<0.001). On the β1 concentration was significantly other hand, TGF-β higher, while IL-6 and sCD138 concentrations were significantly lower, in MGUS than in MM (p<0.001). Only sCD138 was significantly higher in MM3 than in MM1 and in MM2 (p<0.001), while the concentrations of all the other cytokines did not differ significantly between MM1, MM2, and MM3. There were no significant differences in cytokine values between MGUS which evolved into MM3 Received: 24 April 2003 - Revision accepted: 4 August 2003 Correspondence: Dott. Saverio Misso Servizio di Immunoematologia e Medicina Trasfusionale Azienda Ospedaliera "San Sebastiano" Via Tescione 1 81100 Caserta - Italy E-mail: [email protected] 388 Introduzione Le gammapatie monoclonali sono patologie linfoproliferative caratterizzate dalla produzione di immunoglobuline o solamente delle catene leggere o pesanti, conosciute come "componente M", da parte di un clone neoplastico di cellule B1. Le gammapatie sono classificate sulla base del grado di malignità e della componente M. La gammapatia monoclonale di significato non determinato (MGUS) è caratterizzata dall'assenza di sintomi, da una modesta componente M (<3 g/dL), da un'infiltrazione midollare <10%, da una bassa attività proliferativa, senza altre alterazioni tipiche del mieloma multiplo (MM)2. Il rischio di progressione del MGUS a MM o ad altre patologie correlate è circa dell'1% per anno3. Il MM è tipicamente caratterizzato da lesioni osteolitiche, presenza della proteina di Bence-Jones ed insufficienza renale, mentre l'infiltrazione plasmacellulare del midollo osseo è variabile4,5. I meccanismi di trasformazione neoplastica e l'evoluzione delle gammapatie monoclonali sono stati studiati da molti autori, i quali hanno focalizzato la loro attenzione prevalentemente sul coinvolgimento della morte cellulare programmata6,7, sulle anomalie dei meccanismi di adesione cellulare8,9 e sul ruolo delle citochine10. Lo scopo di questo studio è stato quello di valutare l'assetto citochinico in pazienti affetti da MGUS e da MM ed evidenziarne un eventuale cambiamento nei pazienti con MGUS che sviluppano il MM per accertarne un possibile coinvolgimento in questa evoluzione. Materiali e metodi Pazienti Sono stati studiati 51 pazienti (27 uomini, 24 donne) Blood Transfus 2003; 4: 388-99 Cytokines and monoclonal gammopathies and MGUS which did not evolve. Moreover, in the 7 cases of MGUS which did evolve into MM3, the cytokine levels were not significantly different between the start of the study and at the end of the follow-up. We conclude that syndecan-1, like the better recognised β2-M, CRP and IL6 markers, has a prognostic value for the evolution of monoclonal gammopathies. Key words: MGUS, myeloma, cytokine, IL-6, syndecan-1 Introduction Monoclonal gammopathies are lymphoproliferative diseases characterised by the production of immunoglobulins or only light or heavy chains, known as "M component", by a neoplastic B-cell clone1. Gammopathies are classified on the basis of their degree of malignancy and their M component. Monoclonal gammopathy of undetermined significance (MGUS) is characterised by being asymptomatic and having a modest M component (<3 g/dL), with bone marrow infiltration <10% and a low proliferative activity, without other alterations typical of multiple myeloma (MM)2. The risk of progression of MGUS to multiple myeloma or related disorders is about 1 percent per year3. MM is typically characterised by osteolytic lesions, the presence of Bence-Jones protein and kidney failure, while plasma cell infiltration of bone marrow is variable4,5. The mechanisms of neoplastic transformation and evolution of monoclonal gammopathies have been studied by many authors, who have predominantly focused their attention on an involvement of programmed cell death6,7, on anomalies of cell adhesion mechanisms8,9 and on the role of cytokines10. The aim of this study was to evaluate the cytokine network in patients with MGUS and MM and to identify any changes in cytokine concentrations in patients developing a MM from MGUS in order to establish whether the cytokines are involved in this evolution. Materials and methods Patients Fifty-one patients (27 males, 24 females) with MM, 60 (32 M, 28 F) with MGUS and 50 healthy adult subjects (29 M, 21 F) were studied. Blood Transfus 2003; 4: 388-99 affetti da MM, 60 (32 M, 28 F) da MGUS e 50 soggetti adulti in apparente buona salute (29 M, 21 F). La diagnosi di MM nei 51 pazienti, con un'età media di 62 ± 3,1 anni, è stata posta sulla base dei seguenti criteri: a) componente M sierica (IgG >3,5 g/dL o IgA >2 g/dL) e/o urinaria (catene κ o λ > 1 g/24h); b) lesioni osteolitiche; c) infiltrazione plasmacellulare del midollo ≥ 10%5. Questi pazienti sono stati ulteriormente divisi in 3 gruppi secondo la stadiazione del MM effettuata in base ai criteri di Durie e Salmon11. - Stadio I (13 pazienti, gruppo MM1): Hb >10 g/dL, normale concentrazione di Calcio, assenza di lesioni midollari alla radiografia, componente M: IgG <5 g/dL o IgA <3 g/dL, proteinuria di Bence-Jones <4 g/24h. - Stadio II (4 pazienti, gruppo MM2): pazienti non inclusi nello stadio I né nel III; - Stadio III (34 pazienti, gruppo MM3): Hb < 8,5 g/dL, ipercalcemia, estese lesioni scheletriche o fratture patologiche, componente M = IgG > 7 g/dL o IgA > 5 g/ dL, proteinuria di Bence-Jones > 12 g/24 ore. La diagnosi di MGUS è stata posta in 60 pazienti, con un'età media di 69 ± 4,3 anni, secondo i criteri accennati in precedenza. Pazienti HCV+ o HIV+, affetti da MGUS o MM, sono stati esclusi dallo studio per evitare interferenze nella determinazione delle citochine, in quanto le infezioni virali o batteriche possono stimolare un fisiologico sviluppo clonale delle cellule immunitarie. Sono stati studiati anche, come gruppo di controllo (C), 50 soggetti (22 - 49 anni) in apparente buona salute. Protocollo di studio Questo studio è stato articolato in 2 fasi: al tempo dell'arruolamento, le citochine sono state dosate nel siero di tutti i pazienti e dei controlli. Sono state dosate anche la β2-Microglobulina (β2-M) e la proteina C reattiva (CRP) come indicatori di malattia. Dopo un follow-up di 5 anni, 7 dei 60 pazienti, inizialmente affetti da MGUS, sono stati studiati nuovamente perchè la loro patologia era evoluta a MM al III stadio. Dosaggi Mediante test ELISA (Enzyme Linked-Immuno-Sorbent Assay) in fase solida sono stati dosati i livelli sierici di: tumor growth factor-beta1 (TGF-β1) (Biotrak human TGF-β1 ELISA system, Amersham International plc, Little Charlfort, Buckinghamshire, UK), interleuchina 13 (IL-13) (BioSource Cytoscreen human Interleukin-13, BioSource International, 389 S Misso et al. Table I - Serum cytokine levels in patients with monoclonal gammopathy of undetermined significance (MGUS), in patients with multiple myeloma (MM) and in healthy controls (C). Data are shown as mean ± SEM n° of subjects TGF-b1 (ng/mL) sVCAM-1 (ng/ mL) sCD138 (ng/mL) Fas/APO-1 (IU/mL) IL-13 (pg/mL) IL-6 (pg/mL) MGUS MM C 60 51 50 95.2 ± 12.1 § # 2456.5 ± 62.2 § 55.1 ± 18.8 § # 20.6 ± 1.9 § 0.9 ± 0.04 § 24.1 ± 0.5 § # 56.4 ± 2.8 § 2413.9 ± 39.3 § 186.3 ± 6.7 § 18.9 ± 0.5 § 0.86 ± 0.02 § 28.9 ± 0.7 § 4.7 ± 0.4 685.8 ± 68.9 76.4 ± 0.5 8.7 ± 0.4 1.5 ± 0.02 6.1 ± 0.3 § = p <0.001 versus C; # = p<0.001 versus MM The 51 patients with a diagnosis of MM had a mean age of 62 ± 3.1 years. The diagnosis of MM was made on the basis of the presence of following criteria: a) M-component in serum (IgG >3.5 g/dL or IgA >2 g/dL) and/or in urine (κ or λ chains >1 g/24 hr); b) osteolytic lesions; c) plasma cell bone marrow infiltration ≥ 10%5. These patients were further divided into 3 groups according to their stage of MM, as defined by Durie and Salmon's criteria11: - Stage I (13 patients, group MM1): Hb >10 g/dL, normal calcium concentration, absence of radiological bone lesions, M component: IgG <5 g/dL or IgA <3 g/dL, Bence-Jones protein <4 g/24h; - Stage II (4 patients, group MM2): patients not included in stage I or III; - Stage III (34 patients, group MM3): Hb <8.5 g/dL, hypercalcaemia, extensive skeletal injuries or pathological fracture, M component = IgG >7 g/dL or IgA >5 g/dL, Bence-Jones protein >12 g/24h. The 60 patients with MGUS had a mean age of 69 ± 4.3 years and the typical characteristics of the pathology. Patients with MGUS or MM and contemporary HCV or HIV infection were excluded from the study because viral and bacterial infections can cause physiological clonal development of immune cells and thus interfere with the determination of cytokine concentrations. Fifty healthy, sex-matched subjects (22 - 49 years) were also tested as the control group (C). Study protocol This study had two phases: at enrolment, cytokines were assayed in the sera of all patients and controls. β2-M and CRP were also assayed as indicators of disease. After a follow-up of 5 years, 7 of the 60 patients initially characterised as having MGUS were studied again because, in the meantime, their pathology had evolved into stage III MM. 390 Camarillo, CA, USA), interleuchina 6 (IL-6) (Quantikine HS human IL-6, R&D System Inc., Minneapolis, MN, USA), Fas/APO-1 (CD95) (Oncogene Research Products Fas/ APO-1 Assay, Calbiochem, San Diego, CA, USA), Syndecan-1 (SDC1/sCD138) (BioSource Cytoscreen Syndecan, BioSource International) e la forma solubile della vascular cell adhesion molecule (sVCAM1) (Parameter human sVCAM-1, R&D System Inc) [valori normali < 714 ng/mL]. I livelli di β2-M sono stati dosati con tecnica MEIA (Microparticle Enzyme Immunoassay) (AxSYM β2Microglobulin, Abbott Japan, Tokyo, Japan) [v.n. = 0,66 2,25 mg/L]. La CRP è stata determinata mediante dosaggio nefelometrico [v.n. = 0 5 mg/L]. Analisi statistica I dati sono espressi come media ± SEM (Errore Standard Medio). È stata eseguita l'analisi della varianza ad una via (ANOVA) seguita dal test di Newman-Keuls per l'analisi tra i gruppi e dal t-test di Student per i dati appaiati. Il livello di significatività è stato posto al 5% (p <0,05). Risultati I nostri risultati mostrano che i livelli sierici di TGF-β1, sVCAM 1, Fas/APO-1 e IL-6 erano significativamente più alti, mentre quelli dell'IL-13 più bassi, nei pazienti con MGUS o affetti da MM rispetto ai controlli (p <0,001); inoltre i livelli sierici di sCD138, comparati col gruppo di controllo, erano significativamente bassi nella MGUS e alti nel MM (p <0,001) (Tabella I). D'altra parte, il TGF-β1 era significativamente più alto, mentre l'IL-6 e il sCD138 significativamente più bassi nella MGUS rispetto al MM (p <0,001) (Tabella I). TGF-β1, sVCAM 1, Fas/APO-1, IL-13 and IL-6 non presentavano delle differenze statisticamente significative nei tre stadi di MM (Figura 1). Al contrario, i livelli sierici di Blood Transfus 2003; 4: 388-99 Cytokines and monoclonal gammopathies Assays Serum levels of tumour growth factor-beta 1 (TGF-β1) (Biotrak human TGF-β1 ELISA system, Amersham International plc, Little Chalfort, Buckinghamshire, UK), interleukin 13 (IL-13) (BioSource Cytoscreen human interleukin-13, BioSource International, Camarillo, CA, USA), interleukin 6 (IL-6) (Quantikine HS human IL-6, R&D System Inc., Minneapolis, MN, USA), Fas/APO-1 (CD95) (Oncogene Research Products Fas/APO-1 Assay, Calbiochem, San Diego, CA, USA), Syndecan1 (SDC1/sCD138) (BioSource Cytoscreen Syndecan, BioSource International) and the soluble form of vascular cell adhesion molecule (sVCAM1) (Parameter human sVCAM-1, R&D System Inc) [normal range <714 ng/mL] were determined by a solid phase sandwich enzyme linkedimmunosorbent assay (ELISA). β2-M levels were measured with a microparticle enzyme immunoassay (MEIA) (AxSYM β2-microglobulin, Abbott Japan, Tokyo, Japan) [normal range = 0.66 2.25 mg/L]. CRP was measured by a nephelometric assay [normal range = 0 5 mg/L]. Statistical analysis Data are shown as mean ± SEM. ANOVA followed by the Newman-Keuls test for intergroup analysis and Student's t-test for paired data were used. The level of statistical significance was set at 5% (p <0.05). Results Our results showed that serum levels of TGF-β1, sVCAM 1, Fas/APO-1 and IL-6 were significantly higher, while the level of IL-13 was significantly lower in the patients with MGUS or MM than in the controls (p <0.001); moreover, compared with its level in the control group, the serum level of sCD138 was significantly lower in MGUS and significantly higher in MM (p<0.001) (Table I). On the other hand, TGF-β1 concentration was significantly higher, while IL-6 and sCD138 concentrations were significantly lower, in MGUS than in MM (p < 0.001) (Table I). The levels of TGF-β1, sVCAM 1, Fas/APO-1, IL-13 and IL-6 were not significantly different between cases of MM1, MM2, and MM3 (Figure 1). In contrast, the serum level of syndecan-1 was significantly higher in MM3 than in MM1 and in MM2 (p < 0.001) (Figure 1). β2-M and CRP concentrations increased from their lowest levels in the healthy control subjects, intermediate levels in patients with MGUS, through to the highest levels Blood Transfus 2003; 4: 388-99 Syndecan-1 nel MM3 erano significativamente più elevati rispetto a MM1 e MM2 (p <0,001) (Figura 1). Le concentrazioni di β2-M e CRP mostravano livelli crescenti a partrire dai controlli, attraverso i pazienti con MGUS fino ai tre stadi di MM. In particolare la β2-M era statisticamente più elevata nella MGUS rispetto ai controlli (p <0,001), nell'MM1 rispetto a C e MGUS (p <0,001), nell'MM2 rispetto a C e MGUS (p <0,001) e rispetto a MM1 (p <0,05), nell'MM3 rispetto ai C e MGUS (p <0,001) e MM1 (p <0,01) (Figura 2). La CRP era significativamente aumentata nella MGUS, MM1, MM2 e MM3 se comparata con i controlli (p <0,001); inoltre la CRP era significativamente più alta nel MM2 (p <0,01) e nel MM3 (p <0,001) rispetto alla MGUS (Figura 2). Dopo un follow-up di 5 anni, abbiamo rivalutato i 60 pazienti inizialmente affetti da MGUS. Per 53 lo stato della malattia non era cambiato, mentre 7 su 60 (11,6%) sono stati riclassificati come affetti da MM allo stadio III. Abbiamo paragonato i livelli di citochine ottenuti dai risultati iniziali in questi 2 gruppi di pazienti per individuare un eventuale marcatore predittivo di evoluzione. I nostri dati mostravano differenze non statisticamente significative tra questi 2 gruppi (Figura 3). Inoltre, abbiamo paragonato i valori di citochine nei 7 pazienti evoluti a MM3, valutati al momento dell'arruolamento nello studio ed alla fine del follow-up, allo scopo di stabilire se esista una relazione tra evoluzione patologica e modificazione nei livelli di una o più citochine. Non è stata riportata nessuna differenza statisticamente significativa, sebbene il sCD138 fosse significativamente elevato nelle MGUS evolute a MM3 rispetto alle MGUS non evolute (p <0,05) (Figura 3). Discussione Lo scopo di questo studio è stato quello di indagare l'esistenza di un possibile coinvolgimento di TGF-β1, sVCAM-1, Syndecan-1 (sCD138), Fas/APO-1 (CD95), IL13 e IL-6 nell'evoluzione di patologie linfoproliferative da bassa (MGUS) ad alta invasività (MM). L'alterazione dell'assetto citochinico riveste, probabilmente, un importante ruolo nella patogenesi delle malattie linfoproliferative e delle gammapatie monoclonali10. Per tale motivo, lo studio delle citochine e di altre molecole, come i fattori di crescita12, le molecode di adesione9 e quelle coinvolte nell'apoptosi6, può dare preziose informazioni sulla fisiopatologia, diagnosi e prognosi di questi disordini. Nel nostro studio, in accordo con la letteratura, la β2-M e la CRP sono risultati importanti indici prognostici, essendo i loro valori in costante incremento dai controlli allo stadio 391 S Misso et al. Figure 1 - Serum cytokine levels in 51 patients with multiple myeloma (MM): 13 patients had stage I disease (MM1), 4 patients had stage II (MM2) and 34 patients had stage III (MM3). Data are shown as mean ± SEM 392 Blood Transfus 2003; 4: 388-99 Cytokines and monoclonal gammopathies Figure 2 - Serum levels of β2 microglobulin and C-reactive protein in 50 healthy controls (C), 60 patients with monoclonal gammopathy of undetermined significance (MGUS) and 51 patients with multiple myeloma (MM): 13 patients had stage I disease (MM1), 4 patients had stage II (MM2) and 34 patients had stage III (MM3). Data are expressed as mean ± SEM Blood Transfus 2003; 4: 388-99 393 S Misso et al. Figure 3 - Serum cytokine levels in 60 patients with monoclonal gammopathy of undetermined significance (MGUS) in follow-up for 5 years. The 1st column shows initial values in the 53 patients whose MGUS did not evolve during the follow-up. The 2nd and 3rd columns show levels at enrolment and at the end of the follow-up, respectively, in 7 patients whose MGUS evolved into stage III multiple myeloma (MM3). Data are shown as mean ± SEM 394 Blood Transfus 2003; 4: 388-99 Cytokines and monoclonal gammopathies in the three stages of MM. In particular, the level of β2-M was significantly higher in MGUS patients than in controls (p <0.001), in MM1 patients than in controls and MGUS patients (p < 0.001), in MM2 patients than in controls, MGUS patients (p <0.001) and MM1 patients (p <0.05), and finally, in MM3 patients than in controls, MGUS patients (p <0.001) and MM1 patients (p <0.01) (Figure 2). CRP was significantly higher in patients with MGUS, MM1, MM2 and MM3 than in controls (p<0.001); moreover CRP was significantly higher in MM2 (p<0.01) and MM3 (p < 0.001) patients than in patients with MGUS (Figure 2). After a follow-up of 5 years, we re-evaluated the 60 patients initially diagnosed as having MGUS. The state of disease had not changed in 53 of them, whereas the other 7 (11.6%) had developed stage III MM. We compared the cytokine levels obtained at enrolment in these two groups of patients in order to identify possible markers predictive of evolution. Our data showed that there were no significant differences between these two groups at enrolment (Figure 3). Furthermore, in the 7 patients whose MGUS evolved into MM3, we compared the cytokine levels assayed at the time of enrolment into the study and those at the end of the follow-up in order to establish whether there is a relationship between pathological evolution and modification in one or more cytokine levels. No significant modifications were recorded, although the level of sCD138 was significantly higher in MGUS that had evolved into MM3 than in MGUS which did not evolve (p<0.05) (Figure 3). Discussion The aim of this study was to investigate whether TGF-β1, sVCAM-1, syndecan-1 (sCD138), Fas/APO-1 (CD95), IL-13 and IL-6 are involved in the evolution of pathologies from low (MGUS) to high invasiveness (MM). Alterations in the cytokine network probably have an important role in the pathogenesis of lymphoproliferative diseases and monoclonal gammopathies10. For this reason, the study of cytokines and other molecules, such as growth factors12, adhesion9 and apoptosis6 molecules, can give precious information about the pathophysiology, diagnosis and prognosis of these disorders. In accordance with previously published data, we found that both β2-M and CRP were important prognostic indices, their levels increasing from lowest in controls to highest in patients with stage III MM. In fact, many authors have classified MM patients into 3 risk groups (low, intermediate and high) on the basis of CRP and β2-M serum levels13-15. Blood Transfus 2003; 4: 388-99 III del MM. Infatti, molti autori, sulla base dei livelli sierici di CRP e β2-M, classificano i pazienti con MM in 3 gruppi di rischio (basso, intermedio e alto)13-15. In particolare, la concentrazione sierica di CRP riflette l'attività dell'IL-6; questa citochina, infatti, stimola, a livello dell'epatocita, la sintesi delle proteine della fase acuta, tra cui la stessa CRP. Per tale motivo, la concentrazione della CRP risulta essere un fattore prognostico altamente significativo, indipendentemente dai livelli sierici di β2-M14. L'IL-6 è una citochina pleiotropica che stimola le cellule progenitrici emopoietiche e promuove la differenziazione dei linfociti B umani16. I nostri risultati mostrano livelli di IL-6 significativamente elevati sia nella MGUS che nel MM, rispetto ai soggetti sani. È stato dimostrato che l'IL-6 è il maggior fattore di crescita per il MM, sia con azione autocrina sia paracrina1719 . Infatti l'IL-6 e l'IGF-I, fattori di proliferazione e di sopravvivenza del mieloma, inducono la fosforilazione della caveolina-1 (implicata nella trasduzione del segnale e nel trasporto transmembrana)20 e regolano positivamente l'attività telomerasica (associata alla crescita cellulare, sopravvivenza e farmaco-resistenza delle cellule del MM)21. Inoltre, l'IL-6 può sia inibire l'apoptosi Fas-indotta sia modulare l'attività della protein-chinasi attivata dallo stress (SAPK)22. In questo studio, i livelli sierici di Fas/APO-1, appartenente alla famiglia delle proteine di membrana di tipo 1 che trasducono i segnali apoptotici, erano significativamente elevati nella MGUS e nei tre stadi del MM rispetto ai controlli (Tabella I e Figura 1). Un significativo aumento nella concentrazione del ligando di Fas si verifica nei MM negativi per la presenza del recettore di Fas oppure nei MM positivi per la presenza del recettore di Fas ma con la secrezione di varianti di splicing del ligando di Fas23; perciò, questo incremento è la manifestazione dell'evasione, da parte delle cellule mielomatose, dalla sorveglianza immunitaria dell'ospite24. TGF-β1 è prodotto nel MM sia dalle cellule tumorali che dalle cellule stromali midollari e può positivamente regolare la secrezione di IL-625. I nostri dati dimostrano, infatti, che la concentrazione di TGF-β1 è più alta sia nella MGUS che nel MM rispetto ai controlli (Tabella I). Alcuni autori suggeriscono che il TGF-β1 abbia un doppio ruolo: inibisce la proliferazione dei linfociti B normali e la secrezione di Ig e promuove la crescita neoplastica, probabilmente attraverso l'IL-6 e mediante la resistenza delle cellule tumorali ai suoi effetti inibitori25. VCAM-1, espresso dallo stroma midollare, appartiene alla famiglia delle molecole di adesione cellulare (CAM) e rappresenta un ligando per l'integrina VLA-4, la quale media l'attacco e, conseguentemente la localizzazione, delle cellule mielomatose allo stroma midollare26. I livelli di sVCAM-1 sono 395 S Misso et al. In particular, serum CRP concentration reflects IL-6 activity; in fact this cytokine stimulates hepatocytic synthesis of acute phase proteins, such as CRP. For this reason serum CRP level is a highly significant prognostic factor, independently of serum β2-M level14. IL-6 is a pleiotropic cytokine that stimulates haematopoietic progenitor cells and promotes differentiation of human B cells16. We found significantly higher levels of IL-6 in patients with MGUS and MM than in healthy subjects. It has been demonstrated that IL-6 is the major growth factor for MM, acting in either an autocrine or a paracrine fashion17-19. In fact IL-6 and IGF-I, proliferative and survival factors in MM, induce caveolin1 phosphorylation (implicated in signal transduction and transmembrane transport)20 and up-regulate telomerase activity (associated with cell growth, survival and drug resistance in MM cells)21. In addition, IL-6 may both inhibit Fas-induced apoptosis and modulate stress-activated protein kinase (SAPK) activity22. In this study, serum levels of Fas/APO-1, which belongs to the family of type-1 membrane proteins that transduce apoptotic signals, were significantly higher in MGUS and in the three stages of MM than in controls (Table I and Figure 1). Fas ligand concentration is significantly elevated in both Fas receptor-negative MM and in Fas receptorpositive MM with the secretion of Fas splicing variants23; it, therefore, represents the expression of myeloma cells escaping host immune surveillance24. TGF-β1 is produced in MM by both tumour cells and bone marrow stromal cells and can positively regulate IL-6 secretion25. In fact, our data demonstrate that TGF-β1 concentrations are higher in both MGUS and MM than in controls (Table I). Some authors suggest that TGF-β1 has a dual role: it inhibits normal B-cell proliferation and Ig secretion and promotes neoplastic growth, probably through IL-6 and by the fact that tumour cells are resistant to its inhibitory effects25. VCAM-1, expressed on bone marrow stroma, belongs to the family of cell adhesion molecules (CAM) and is a ligand for the integrin VLA-4, which mediates attachment, and consequently localisation, of myeloma cells to MM stroma26. We found increased levels of sVCAM-1 in all our patients (Table I): in both groups the sVCAM-1 concentrations exceeded 3.5 times the values observed in controls and the upper limit of the normal range. There are reports of a statistical relationship between sVCAM-1 and various elements of the cytokine network (IL-2, sIL-2R, sIL-6R, TNF-α, sICAM-1)27 and β2-M28, so soluble forms of adhesion molecules probably play a role in the 396 stati trovati aumentati in tutti i nostri pazienti (Tabella I): in entrambi i gruppi il sVCAM-1 superava di 3,5 volte il valore osservato nei C ed il limite superiore dei valori di riferimento. È stato dimostrato che esiste una correlazione tra sVCAM1 e vari elementi del network citochinico (IL-2, sIL-2R, sIL6R, TNF-α, sICAM-1)27 e con la β2-M28, perciò le forme solubili delle molecole di adesione probabilmente possono giocare un ruolo nella patogenesi del MM, ma a tutt'oggi la loro peculiare attività non è stata ancora chiarita. In aggiunta, l'espressione di VCAM-1 nelle cellule endoteliali è regolata dall'IL-13, una citochina multifunzionale elaborata dai linfociti T attivati29. Sulla base dei nostri risultati, il Syndecan-1 sembra un valido indice prognostico dell'evoluzione a MM. Infatti, la sua concentrazione è più alta nel MM rispetto alla MGUS e rispetto ai soggetti sani (Tabella I); inoltre, nell'ambito dei soggetti con MM, i più elevati valori di Syndecan-1 sono stati registrati nei pazienti allo stadio III (Figura 1). Questa molecola è espressa sulle cellule linfoidi B nei vari stadi di differenziazione30. Il CD138 è un proteoglicano eparan-solfato transmembrana31, capace di legare numerose molecole: componenti della matrice extra-cellulare (come il collagene di tipo I32, la fibronectina33 e la trombospondina34), citochine e fattori di crescita (come TGF-β1 e FGF-2)35. Il Syndecan-1 regola varie funzioni cellulari (adesione, proliferazione ed apoptosi) e probabilmente gioca un ruolo nell'oncogenesi36. Nei pazienti con MM, il CD138 è espresso, nel midollo osseo, solo sulle cellule mielomatose37 e, nel sangue periferico, sulle plasmacellule maligne38. I nostri risultati mostrano che la MGUS evolvente a MM presenta alte concentrazioni di sCD138 rispetto alla MGUS non evolvente, anche se questa differenza non è statisticamente significativa a causa della grande dispersione dei dati e, di conseguenza, per un ampio errore standard (Figura 3). D'altra parte, i livelli sierici di Syndecan-1 sono significativamente più elevati nel MM originatosi dalla MGUS rispetto alla MGUS non evolvente (Figura 3). I dati osservati possono essere spiegati dal fatto che le cellule mielomatose apoptotiche perdono rapidamente il Syndecan-139. Infine, alti livelli di Syndecan1 sono associati con un'alta percentuale di plasmocitosi midollare ed elevati livelli di β2-M40; per tale motivo, esso costituisce un parametro prognostico indipendente e potrebbe essere utile nella classificazione prognostica del MM41. In conclusione, al di là dell'ormai noto ruolo della β2-M, della CRP e dell'IL-6, possiamo affermare che il Syndecan-1 potrebbe avere un valore prognostico nell'evoluzione delle gammapatie monoclonali, sebbene non sia ancora chiaro se un'aumentata concentrazione di Syndecan-1 nel MM risulti critica per lo sviluppo della Blood Transfus 2003; 4: 388-99 Cytokines and monoclonal gammopathies pathogenesis of MM although their particular activities have not yet been clarified. In addition, VCAM-1 expression in endothelial cells is regulated by IL-13, a multifunctional cytokine produced by activated T cells29. On the basis of our results, syndecan-1 seems to be a valid prognostic indicator of the evolution to MM. In fact, its concentration in MM was higher than in MGUS and in healthy subjects (Table I); moreover, within the subsets of MM, the highest levels of syndecan-1 were recorded in patients with stage III disease (Figure 1). This molecule is expressed on lymphoid B cells at various stages of differentiation30. CD138 is a transmembrane heparan sulfate proteoglycan31 able to link numerous molecules: extracellular matrix components (such as type I collagen32, fibronectin33 and thrombospondin34), cytokines and growth factors (such as TGF-β1 and FGF-2)35. Syndecan-1 regulates various cell functions (adhesion, proliferation and apoptosis) and probably plays a role in oncogenesis36. In MM patients, CD138 is expressed, in bone marrow, only on myeloma cells37 and, in peripheral blood, on malignant plasma cells38. Our results show that the concentration of sCD138 in cases of MGUS evolving into MM was higher than in the not evolving cases although this difference was not statistically significant because of a large dispersion of data and, consequently, a large SEM (Figure 3). Nevertheless, serum syndecan-1 levels were significantly higher in MM that had evolved from MGUS than in not evolving MGUS (Figure 3). These observations can be explained by a rapid lost of syndecan-1 by apoptotic myeloma cells39. Finally, high levels of syndecan-1 are associated with a high percentage of bone marrow plasmocytosis and β2-M levels40; indeed, syndecan1 is an independent prognostic parameter and should be useful in the prognostic classification of MM41. In conclusion, besides confirming the well known role of β2-M, CRP and IL-6, the results of our study suggest that syndecan-1 levels may have a prognostic value for the evolution of monoclonal gammopathies, although it is not yet clear whether the increased serum level of syndecan-1 in MM is critical for the development of disease or whether it is a secondary characteristic related to the pathological progression of the disease. Acknowledgements The authors have the pleasure of thanking Dr. Francesca Giordano for editing the text. malattia o rappresenti una caratteristica secondaria correlata alla progressione patologica. Riassunto Scopo di questo studio è stato quello di valutare l'influenza di alcune citochine nell'evoluzione delle gammapatie monoclonali. Sono stati studiati 51 pazienti affetti da mieloma multiplo (MM), suddivisi in 3 gruppi in base alla stadiazione (MM1, MM2, MM3), 60 pazienti con gammapatia monoclonale di significato non determinato (MGUS) e 50 soggetti di controllo in apparente buona salute (C). Abbiamo testati i livelli sierici di sCD138 (Syndecan-1), TGF-β1, sVCAM-1, IL-13, Fas/APO-1, IL-6,β2-Microglobulina (β2-M) e proteina C reattiva (CRP). In un follow-up di 5 anni, la MGUS è evoluta a MM3 in 7 pazienti su 60 (11,6%); questi sono stati ri-esaminati per evidenziare un eventuale modifica nell'assetto citochinico. Le concentrazioni della β2-M e della CRP mostravano livelli significativamente crescenti dai C, ai MGUS ed ai 3 stadi di MM. I livelli di TGF-β1, sVCAM-1, Fas/APO-1 e IL-6 erano significativamente più alti, mentre quello dell'IL-13 più basso, nei pazienti con MGUS e con MM rispetto a C (p<0,001). sCD138 era significativamente più basso nei MGUS e più alto nei MM, a paragone con C (p<0,001). D'altronde, il TGF-β1 era significativamente più alto, mentre l'IL-6 e il sCD138 erano significativamente più bassi, nei MGUS rispetto ai MM (p<0,001). Nei pazienti con MM al 3° stadio, solo il Syndecan-1 era significativamente elevato rispetto agli altri stadi (p<0,001), mentre tutte le altre citochine non mostravano delle differenze significative tra i 3 stadi di malattia. Tra gli MGUS evoluti a MM3 e gli MGUS stabili, non evoluti, non abbiamo trovato differenze significative nei valori delle citochine. Inoltre, nei 7 pazienti con MGUS evoluta a MM3 non c'erano modificazioni significative nei livelli citochinici registrati all'inizio dello studio ed alla fine del follow-up. Al di là del ruolo già conosciuto della β2-M, della CRP e dell'IL-6, possiamo concludere che anche il Syndecan-1 ha un valore prognostico per l'evoluzione delle gammapatie monoclonali. Parole chiave: MGUS, mieloma, citochine, IL-6, syndecan-1 Ringraziamenti Gli autori hanno il piacere di ringraziare la Dott.ssa Francesca Giordano per l'editing dell'articolo. Blood Transfus 2003; 4: 388-99 397 S Misso et al. References 1) Kyle RA, Rajkumar SV. Monoclonal gammopathies of undetermined significance: a review. Immunol Rev 2003; 194: 112-39. 2) Kyle RA, Rajkumar SV. Monoclonal gammopathies of undetermined significance. Rev Clin Exp Hematol 2002; 6: 225-52. 3) Kyle RA, Therneau TM, Rajkumar SV, et al. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med 2002; 346: 564-9. 4) Harris NL, Jaffe ES, Diebold J, et al. The World Health Organization classification of neoplastic diseases of the haematopoietic and lymphoid tissues: Report of the Clinical Advisory Committee Meeting, Airlie House, Virginia, November 1997. Histopathology 2000; 36: 69-86. 5) Kyle RA. Diagnosis of multiple myeloma. Semin Oncol 2002; 29: 2-4. 6) Witzig TE, Timm M, Larson D, et al. Measurement of apoptosis and proliferation of bone marrow plasma cells in patients with plasma cell proliferative disorders. Br J Haematol 1999, 104: 131-7. 7) Hata H, Matsuzaki H, Takeya M, et al. Expression of Fas/Apo-1 (CD95) and apoptosis in tumor cells from patients with plasma cell disorders. Blood 1995; 86: 1936-45. 8) Luque R, Brieva JA, Moreno A, et al. Normal and clonal B lineage cells can be distinguished by their differential expression of B cell antigens and adhesion molecules in peripheral blood from multiple myeloma (MM) patients diagnostic and clinical implications. Clin Exp Immunol 1998; 112: 410-8. 9) Verfaillie CM. Adhesion receptors as regulators of the hematopoietic process. Blood 1998; 92: 2609-12. 10) Lauta VM. A review of the cytokine network in multiple myeloma: diagnostic, prognostic, and therapeutic implications. Cancer 2003; 97: 2440-52. 11) Durie BG, Salmon DE. A clinical staging system for multiple myeloma: correlation of measured myeloma cell mass with presenting clinical features, response to treatment and survival. Cancer 1975 36: 842-54. 12) Anderson KC, Jones RM, Morimoto C, et al. Response patterns of purified myeloma cells to hematopoietic growth factors. Blood 1989; 73: 1915-24. 13) Greipp PR, Katzmann JA, OFallon WM, Kyle RA. Value of beta 2-microglobulin level and plasma cell labelling indices as prognostic factors in patients with newly diagnosed myeloma. Blood 1988; 72: 219-23. 14) Bataille R, Boccadoro M, Klein B, et al. C-reactive protein and beta-2 microglobulin produce a simple and powerful myeloma staging system. Blood 1992; 80: 733-7. 15) Greipp PR, Lust JA, OFallon WM, et al. Plasma cell labelling index and beta 2-microglobulin predict survival independent of thymidine kinase and C-reactive protein in multiple myeloma. Blood 1993; 81: 3382-7. 16) Klein B, Zhang XG, Lu ZY, Bataille R. Interleukin-6 in human multiple myeloma. Blood 1995; 85: 863-72. 17) Klein B, Zhang XG, Jourdan M, et al. Paracrine rather than autocrine regulation of myeloma-cell growth and differentiation by interleukin-6. Blood 1989; 73: 517-26. 18) Barut BA, Zon LI, Cochran MK, et al. Role of interleukin 6 in the growth of myeloma-derived cell lines. Leuk Res 1992; 16: 951-9. 19) Urashima M, Ogata A, Chauhan D, et al. Interleukin-6 promotes multiple myeloma cell growth via phosphorylation of retinoblastoma protein. Blood 1996; 88: 2219-27. 20) Podar K, Tai YT, Cole CE, et al. Essential role of caveolae in interleukin-6- and insulin-like growth factor I-triggered Akt-1mediated survival of multiple myeloma cells. J Biol Chem 2003; 278: 5794-801. 21) Akiyama M, Hideshima T, Hayashi T, et al. Cytokines modulate telomerase activity in a human multiple myeloma cell line. Cancer Res 2002; 62: 3876-82. 22) Chauhan D, Kharbanda S, Ogata A, et al. Interleukin-6 inhibits Fas-induced apoptosis and stress-activated protein kinase activation in multiple myeloma cells. Blood 1997; 89: 227-34. 23) Frassanito MA, Silvestris F, Silvestris N, et al. Fas/Fas ligand (FasL)-deregulated apoptosis and IL-6 insensitivity in highly malignant myeloma cells. Clin Exp Immunol 1998; 114: 179-88. 24) Villunger A, Egle A, Marschitz I, et al. Constitutive expression of Fas (Apo-1/CD95) ligand on multiple myeloma cells: a potential mechanism of tumor-induced suppression of immune surveillance. Blood 1997; 90: 12-20. 25) Urashima M, Ogata A, Chauhan D, et al. Transforming growth factor-beta1: differential effects on multiple myeloma versus normal B cells. Blood 1996; 87: 1928-38. 398 Blood Transfus 2003; 4: 388-99 Cytokines and monoclonal gammopathies 26) Sanz-Rodriguez F, Ruiz-Velasco N, Pascual-Salcedo D, Teixido J. Characterization of VLA-4-dependent myeloma cell adhesion to fibronectin and VCAM-1. Br J Haematol 1999; 107: 825-34. 27) Scudla V, Budikova M, Bacovsky J, et al. Relation of serum levels of the soluble cytoadhesion molecules sVCAM-1 and sICAM1 to selected factors in the cytokine network in multiple myeloma. Cas Lek Cesk 2000; 139: 401-6. 28) Scudla V, Budikova M, Bacovsky J, et al. Relation of the soluble cytoadhesion molecules VCAM-1 and ICAM-1 to selected clinical and laboratory indicators in multiple myeloma. Vnitr Lek 1999; 45: 583-90. 29) Rifas L, Cheng SL. IL-13 regulates vascular cell adhesion molecule-1 expression in human osteoblasts. J Cell Biochem 2003; 89: 213-9. 30) Sanderson RD, Lalor P, Bernfield M. B lymphocytes express and lose syndecan at specific stages of differentiation. Cell Regul 1989; 1: 27-35. 31) Carey DJ. Syndecans: multifunctional cell-surface co-receptors. Biochem J 1997; 327: 1-16. 32) Ridley RC, Xiao H, Hata H, et al. Expression of syndecan regulates human myeloma plasma cell adhesion to type I collagen. Blood 1993; 81: 767-74. 33) Saunders S, Bernfield M. Cell surface proteoglycan binds mouse mammary epithelial cells to fibronectin and behaves as a receptor for interstitial matrix. J Cell Biol 1988; 106: 423-30. 34) Sun X, Mosher DF, Rapraeger A. Heparan sulfate-mediated binding of epithelial cell surface proteoglycan to thrombospondin. J Biol Chem 1989; 264: 2885-9. 35) Filla MS, Dam P, Rapraeger AC. The cell surface proteoglycan syndecan-1 mediates fibroblast growth factor-2 binding and activity. J Cell Physiol 1998; 174: 310-21. 36) Holen I, Drury NL, Hargreaves PG, Croucher PI. Evidence of a role for a non-matrix-type metalloproteinase activity in the shedding of syndecan-1 from human myeloma cells. Br J Haematol 2001; 114: 414-21. 37) Wijdenes J, Vooijs WC, Clement C, et al. A plasmocyte selective monoclonal antibody (B-B4) recognizes syndecan-1. Br J Haematol 1996; 94: 318-23. 38) Witzig TE, Kimlinger T, Stenson M, Therneau T. Syndecan-1 expression on malignant cells from the blood and marrow of patients with plasma cell proliferative disorders and B-cell chronic lymphocytic leukemia. Leuk Lymphoma 1998; 31: 167-75. 39) Jourdan M, Ferlin M, Legouffe E, et al. The myeloma cell antigen syndecan-1 is lost by apoptotic myeloma cells. Br J Haematol 1998; 100: 637-46. 40) Dhodapkar MV, Kelly T, Theus A, et al. Elevated levels of shed syndecan-1 correlate with tumour mass and decreased matrix metalloproteinase-9 activity in the serum of patients with multiple myeloma. Br J Haematol 1997; 99: 368-71. 41) Seidel C, Sundan A, Hyorth M, et al. Serum syndecan-1: a new independent prognostic marker in multiple myeloma. Blood 2000, 95: 388-92. Blood Transfus 2003; 4: 388-99 399
Scaricare