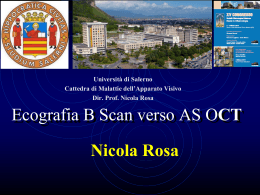
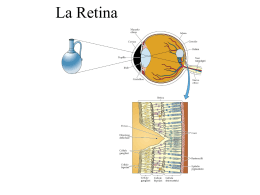
CASO CLINICO Tomografia ottica a radiazione coerente in un caso di Multiple Evanescent White Dot Syndrome Optical Coherence Tomography in a case of Multiple Evanescent White Dot Syndrome M. Nicolò, M. Badino Riassunto La Multiple Evanescent White Dot Syndrome (MEWDS) è una patologia a eziologia sconosciuta che colpisce tipicamente donne tra la seconda e quinta decade di vita. L’esame oftalmoscopico mostra molteplici chiazzette color giallo delle dimensioni di 100-200 μm situati negli strati retinici più profondi così come una tipica sgranatura della regione foveale. La fluorangiografia (FAG) e gli studi elettrofunzionali suggeriscono che la sede del processo patologico è nella retina esterna e/o a livello dell’epitelio pigmentato retinico (EPR). All’angiografia con verde indocianina (ICG), le lesioni della MEWDS appaiono ipofluorescenti e scompaiono una volta che si è verificato il recupero clinico, suggerendo una ipoperfusione della coroide o l’infiammazione dell’EPR come base patogenetica. Le alterazioni del campo visivo sono in correlazione con l’ICG. Recentemente alcuni autori hanno dimostrato che la risoluzione assiale di 3 μm che è possibile con l’ultra-high resolution OCT (UHR-OCT) consente di visualizzare in vivo la microstruttura della retina quasi come una sezione istologica. Sebbene l’UHR-OCT offra un significativo miglioramento rispetto alla risoluzione di 10 μm dello Stratus OCT, riportiamo e correliamo il recupero dell’acuità visiva con la stato della giunzione tra segmento esterno e interno dei fotorecettori, utilizzando lo Stratus OCT. Dipartimento di Neuroscienze, Oftalmologia e Genetica, Istituto di Clinica Oculistica, Università di Genova Summary Multiple evanescent white dot syndrome (MEWDS) is a disease of unknown aetiology that characteristically occurs in women in the second to fifth decades. Ophthalmoscopic examination typically reveals multiple, 100- to 200-μm yellow-white dots deep on the retina as well as a unique foveal granularity. Fluorescein angiography (FA) and electrophysiologic studies suggest that the location of the disease process is in the outer retina and/or the retinal pigment epithelium (RPE). Upon indocyanine green angiography (ICG), MEWDS lesions are hypofluorescent and disappear with clinical recovery, suggesting pathologic choroidal nonperfusion or RPE inflammation. Visual field alterations correlate well with ICG findings. It has been recently reported that 3 μm axial resolution of the ultrahigh resolution optical coherence tomography (UHR-OCT) offers the possibility to visualize detailed retinal microstructure in vivo, with a resolution approaching that of histology. Although UHR-OCT offers significant improvement over the 10 μm resolution available with a StratusOCT (Carl Zeiss Meditec, Inc., Dublin, CA, USA), we report and correlate the recovery of visual acuity with the status of the junction between inner and outer segments of the photoreceptor using StratusOCT. Indirizzo per la corrispondenza: Dott. M. Nicolò, Dipartimento di Neuroscienze, Oftalmologia e Genetica, Istituto di Clinica Oculistica, Università di Genova Viale Benedetto XV, Genova. E-mail: [email protected] 41 M. Nicolò, et al. Descrizione del caso clinico Donna di 33 anni con storia di repentino calo del visus, scotoma paracentrale e annebbiamento visivo nell’occhio di sinistra insorto da due giorni. La paziente è stata sottoposta a misurazione della acuità visiva con migliore correzione, esame biomicroscopico del segmento anteriore, esame oftalmoscopico indiretto, FA, ICG, campo visino e OCT, all’esordio e alla fine delle manifestazioni cliniche. L’acuità visiva era 10/10 in OD e 5/10 in OS. Il segmento anteriore era nella norma in entrambi gli occhi. L’esame del fundus dell’occhio sinistro mostrava sgranatura della regione maculare e molteplici lesioni giallobianche delle dimensioni di 100-200 μm situate in profondità nella retina. Nelle fasi precoci della FA le lesioni erano iperfluorescenti e si impregnavano nelle fasi tardive dell’esame. La FA mostra inoltre edema della papilla. All’ICG le lesioni apparivano ipofluorescenti. L’esame del campo visivo mostrava un allargamento della macchia cieca. L’esame OCT mostrava attenuazione del segnale proveniente dalla giunzione tra segmento esterno e interno dei fotorecettori e l’impossibilità di individuare la sottile linea che corrisponde a tale giunzione. Il segmento posteriore dell’occhio destro era normale. Due settimane dopo l’acuità visiva nell’occhio sinistro era 10/10. La FA e l’ICG mostravano la completa regressione delle lesioni retiniche e la granularità 2 3 Figg. 2-3. La fluorangiografia mostra precoce iperfluorescenza e impregnazione tardiva delle lesioni – Fluorescein angiography showing early hyperfluorescence and late staining of the lesions. della macula era notevolmente regredita. L’esame OCT mostrava chiaramente la linea di giunzione del segmento esterno e interno dei fotorecettori. Fig. 1. La fotografia a colori del fondo oculare mostra la sgranatura della macula e le molteplici lesioni giallo-bianche delle dimensioni di 100-200 μm situate in profondità nella retina – Colour fund photograph showing macular granularity and the yellow-white 100 to 200 μm lesions deep on the retina. 42 Fig. 4. L’angiografia con verde indocianina mostra ipofluorescenza della lesioni – Indocyanine green angiography showing hypofluorescence of the lesions. CASO CLINICO Discussione Nel 1984, Jampol et al. descrissero la MEWDS come una malattia infiammatoria intraoculare idiopatica, caratterizzata dalla formazione transitoria di lesioni giallo-bianche, la cui localizzazione presunta era a livello dello strato dei fotorecettori o dell’EPR 1. Le lesioni sono meglio descritte come aree puntiformi iperfluorescenti alla FA. Al contrario all’ICT tali lesioni appaiono ipofluorescenti e molto più numerose rispetto alla FA. Precedenti studi hanno tentato di localizzare e interpretare le lesioni della MEWDS sulla base dei dati oftalmoscopici e fluorangiografici. Usando lo Stratus OCT siamo stati in grado di visualizzare la giunzione tra segmento interno ed esterno dei fotorecettori sia prima che dopo il recupero della malattia. L’OCT consente di visualizzare la microstrut- tura della retina in corso di patologia. Studi basati sulla Fa e ICG suggeriscono che le anomalie dei fotorecettori nella MEWDS siano conseguenza o di ischemia della coroide o di infiammazione dell’EPR 2. Tuttavia l’esame OCT evidenzia che la MEWDS è più probabilmente associata a infiammazione dell’EPR. Cellule dell’EPR rigonfie ma integre appaiono normali all’esame OCT. L’infiammazione dell’EPR potrebbe essere in grado di interrompere in modo acuto l’orientamento del segmento esterno dei fotorecettori, causando l’attenuazione del segnale OCT che corrisponde alla giunzione tra segmento esterno e interno dei fotorecettori. Inoltre, dato che la sottile linea di giunzione tra segmento interno ed esterno dei fotorecettori ricompare dopo che la malattia è regredita, l’OCT può essere usato come metodo non invasivo di follow-up in patologie di questo tipo. Fig. 5. L’esame OCT mostra rarefazione della giunzione tra segmento interno ed esterno dei fotorecettori – Optical Coherence Tomography (OCT) showing the reduction of the junction between the inner and outer segments of the photoreceptor. Fig. 6. L’esame OCT eseguito 2 settimane dopo mostra la riformazione della giunzione tra segmento interno ed esterno dei fotorecettori – Optical Coherence Tomography (OCT) two weeks later showing the recovery of the junction between the inner and outer segments of the photoreceptor. Report of the clinical case sibility to discern the thin reflection line that represents that junction. The posterior segment of the right eye was unremarkable. Two weeks later, BCVA in the left eye was 20/20. FA and ICG-A showed complete disappearance of the spots, although there was still a minimal foveal granularity. However, OCT showed a clearly discernible reflection line between inner and outer photoreceptor segments. A 33-year-old woman presented with a rapid onset (2 days) history of photopsias, paracentral scotoma and blurred vision in the left eye. Best-corrected visual acuity exam (BCVA), complete slit lamp anterior segment examination, indirect ophtalmoscopic exam, FA, ICG-A, visual field test and OCT were performed at the onset and at the end of clinical manifestations. BCVA was 20/20 in the right eye and 20/40 in the left eye. Anterior segment exam was unremarkable in both eyes. In the left eye, fundus examination revealed foveal granularity and multiple, yellow-white 100 to 200 μm lesions deep on the retina. FA showed typical early hyperfluorescence and late staining of these lesions as well as disk leakage. ICG-A showed hypofluorescence of the spots. Visual field testing showed an enlargement of blind spots. OCT imaging demonstrated attenuation of the signal from the photoreceptors inner/outer segment junction and the impos- Discussion In 1984, Jampol et al. described MEWDS as an idiopathic intraocular inflammatory disorder, characterized by the development of transient small white-yellowish lesions, presumed to occur at the level of the retinal photoreceptors or RPE 1. The lesions are best characterized as wreathlike punctuate areas of early hyperfluorescence on FA. In contrast, ICG-A in patients 43 M. Nicolò, et al. with MEWDS reveals numerous hypofluorescent lesions that significantly outnumber their counterparts seen by clinical examination and FA. Previous studies have attempted to localize and interpret the lesions of MEWDS on a clinical and angiographic basis. Using StratusOCT, capable of 10 μm axial resolution, we were still able to visualize the photoreceptor IS/OS junction of this patient with MEWDS before and after recovery of the disease. OCT offers a unique opportunity to visualize the retinal microstructure in the disease. FA and ICG-A reviews suggest that photoreceptor abnormalities of MEWDS are due to either choroidal ischaemia or RPE inflammation 2. However, OCT images suggest that MEWDS is more likely associated with RPE inflammation. Swollen but intact RPE cells would likely appear normal on OCT imaging. Inflammation of RPE cells could interrupt the orientation of photoreceptor outer segments acutely, causing attenuation of OCT signal from the junction between photoreceptors inner/outer segments, that becomes misaligned. Since there are no reports of other conditions causing similar changes in the outer retina, we believe that OCT represents a useful adjunct to diagnosis. Moreover, because the thin reflection line of junction between photoreceptors inner and outer segments reappears at the disappearance of clinical picture, OCT may be used as non-invasive exam during follow-up. References 2 1 Jampol LM, Sieving PA, Pugh D, Fishman GA, Gilbert H. Multiple evanescent white dot syndrome. I. Clinical findings. Arch Ophthalmol 1984;102:671-4. 44 Nguyen MH, Witkin AJ, Reichel E, Ko TH, Fujimoto JG, Schuman JS, et al. Microstructural abnormalities in MEWDS demonstrated by ultrahigh resolution optical coherence tomography. Retina 2007;27:414-8.
Scaricare