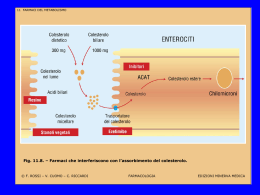
EDITORIAL Cholesterol Can be Lowered in Older Persons Should we care? Scarso/incerto valore predittivo del colesterolo e pochi dati da RCT nei vecchi. Pluripatologia e importanti “competing” cause di mortalità Scetticismo verso inquinanti “commerciali” della medicina JAGS 1990 Age and Ageing 1999; 28: 313-315 Cholesterol and long-term mortality after acute myocardial infarction in elderly patients Mario Bo, Umberto Fiandra, Gianfranco Fonte, Marco Bobbio, Fabrizio Fabris No. (%) by total cholesterol, mg/dl Normo/Hyper cholesterolemia <164 165-188 189-220 >220 <230 >=230 p All-cause mortality 52 (67.5) 54 (72.0) 44 (57.9) 48 (63.2) 114 (69.5) 84 (60.0) <0.05 CHD mortality 23 (29.9) 26 (34.7) 20 (26.3) 21 (27.6) 53 (34.6) 37 (29.8) <0.05 304 patients (192 men, mean age 73.3+-5.7 years), mean survival time 1758.1+- 113.8 days Prospective Association Between Low and High Total and Low-Density Lipoprotein Cholesterol and Coronary Heart Disease in Elderly Men J.David Curb, MD et al. J Am Geriatr Soc 52:1975-1980, 2004 3 Age- and risk factor-adjusted RR of CHD 1.8 2 1.5 1 2.6 Total Cholesterol 1.1 1.5 LDL Cholesterol 1.2 1.0 0 <160 160-179 180-199 200-219 220-239 240+ <80 80-99 100-119 120-139 140-159 160+ CONCLUSION…the U-shaped associations between TC and LDL-C and CHD imply a complex relationship between lipids and CHD in late life…the results indicate that elevated lipid levels should continue to be treated in healthy elderly individuals, as they are in those who are younger J Am Geriatr Soc 52:1975-1980, 2004 BRIEF REPORTS Low-Density Lipoprotein Cholesterol and Mortality in Older People 1887 women and 1223 men 65 years+ (mean age 73.8); mean follow-up 11.1 years Death per 1000 patient-years 100 TOTAL CARDIOVASCULAR 40 MEN WOMEN 80 30 60 40 20 80 120 160 200 80 120 160 200 mg/dl LDL CONCLUSION: This study adds to the uncertainty of the role of elevated levels of LDL-C as a risk factor for mortality in old people. J. Am. Geriatr. Soc. 2005 Prospective population-based cohort study; 5750 adults aged 55 to 99; median follow up 13.9 years Leiden Plus Study on 599 patients aged >=85 years Conclusions. In old age, larger declines in BMI, total cholesterol levels, and blood pressure and weaker increases in HDL cholesterol levels associate with mortality. We identified distinct clustering in the dynamics of these traditional metabolic risk factors and indicators of health and disease in a profile that is suggestive of underlying wasting disease. <175 176-199 .5 Cumulative mortality 200-226 >226 .4 .3 CONCLUSION: Low cholesterol level is a robust predictor of mortality in the nondemented elderly and may be a surrogate of frailty or subclinical disease… Participants taking lipidlowering drugs were only one-quarter as likely to die as those not taking drugs .2 .1 0.0 2 4 6 8 years Lowest levels. Several prospective population studies have suggested that the mortality benefit associated with lower TC plateaus at levels around 180 mg/dl… Lowered by treatment. Lowered TC, either by behavioral intervention or – much more potently – by drug therapy, is a question distinct from naturally low TC. The evidence that pharmacologic therapy of dyslipidemia in higher risk middle-aged men results in a total mortality benefit is extensive and convincing…. The benefits of statins…appear proportional to the degree of improvement in the TC/HDL ratio, and by far the largest reductions in event rates reported occurred with combination statin and niacin therapy, with the attendant profound lowering of the TC/HDL ratio….Only consideration of HDL cholesterol allows much predictive power at middle or older ages. …all individuals presenting with an acute vascular event of any type in any arterial territory irrespective of age in a population of 91106 in Oxfordshire, UK, in 2002-05 …2024 acute vascular events occurred in 1657 individuals: 918 (45%) cerebrovascular (618 stroke, 300 TIA); 856 (42%) coronary vascular (159 STEMI, 316 NSTEMI, 218 UA, 163 SCD); 188 (9%) peripheral vascular (43 aortic, 53 embolic visceral or limb ischemia, 92 critical limb ischemia)…event and incidence rates rose steeply with age in all arterial territories, with 80% cerebrovascular, 73% coronary and 78% peripheral vascular events in 12886 (14%) individuals aged 65 years or older; and 54%, 47% and 56%, respectively, in the 5919 (6%) aged 75 years or older….although case fatality rates increased with age, 47% of non-fatal events occurred at age 75 years or older Lifetime risks of fatal and nonfatal events according to aggregate burden of risk factors in men and women Men Women 51° CONGRESSO NAZIONALE SIGG “La longevità del Paese: risorse e problema” Firenze, 29 novembre-3 dicembre 2006 PAZIENTE ANZIANO E DISLIPIDEMIE: QUALE TRATTAMENTO E’ PIU’ EFFICACE? L’evidenza che colesterolo totale ed LDL non sono predittivi di mortalità cardiovascolare e totale nell’insieme dei soggetti anziani non significa necessariamente che non vi sia spazio per i benefici di una terapia ipocolesterolemizzante in questi pazienti. Occorre quindi chiedersi se Vi sono evidenze che l’intervento ipocolesterolemizzante si associ ad un beneficio in termini di morbilità/mortalità negli anziani? In caso di risposta affermativa, quali sono le priorità per un trattamento ottimale in questa fascia di età? DISLIPIDEMIE FUMO DIABETE IPERTENSIONE ETA’ SESSO FAMILIARITA’ OBESITA’ SEDENTARIETA’ S.METABOLICA INFIAMMAZIONE IPERCOAGULABILITA’… …il punto quindi non è tanto l’ipercolesterolemia in sé quanto la possibilità della prevenzione delle manifestazioni cliniche aterosclerotiche attraverso l’impiego di farmaci ipocolesterolemizzanti che hanno dimostrato importanti benefici nei soggetti ad alto rischio CV…occorre quindi valutare se esistano delle evidenze in questo senso e quali siano gli interventi efficaci in questo ambito nell’anziano… 1250 women and 664 men 65 years and older (71.1); mean follow-up 7.3 years; 382 CV events and 362 deaths Association of drug therapy to lower cholesterol levels with incident CV events Association of drug therapy to lower cholesterol levels with mortality …statin use was associated with similar lower risk of incident CV events among participants 74 years and older and among participants aged 65 to 73 years… 1.5 million veterans in 10 hospitals Risk score (0-6): age>70; DM; previous MI; hypertension; LDL-C>100 mg/dl; current smoking statin nonusers statin users OR 0.54 (0.42-0.69) p<0.0001 Age distribution at death among statin users and nonusers. Age at death was 2.1 years older among statin users (p<0.0001) Graded relation between risk of death and benefit of statin therapy. For risk scores >1, reduction in death was highly significant Predictors of death STATINS Observational study in acute care hospitals in US from april 1998 to june 2001 23013 Medicare patients aged 65 and older who did and did not receive a discharge prescription for statin 8452 of patients (40%) were aged 80 and older 5513/23013 (24%) in the overall sample and 1310/8452 of those aged 80 and older (15.5%) received a statin at discharge NO STATINS 65-69 Unadjusted Kaplan Meier estimates of 3 year survival in patients prescribed statins at discharge versus patients not prescribed statins at discharge 70-74 75-79 CONCLUSION-Statin therapy is associated with lower mortality in older patients with AMI younger than 80 but not in those aged 80 and older, as a group. This finding questions whether statin efficacy data in younger patients can be broadly applied to the very old and indicated the need for further study of this group. 80-84 85+ Adjusted hazard ratio (HR) of 3 year mortality for patients prescribed statins at discharge versus patients not prescribed statins at discharge by 5-year age increments. 20536 pazienti (75% maschi), 40-80 anni (28%>70), col.tot.>134 mg/dl, alto rischio CV: storia di CAD; altre malattie ats ostruttive o precedenti rivascolarizzazioni; DM (tipo 1 e 2); ipertesi se maschi >65 anni ANY DEATH ANY MAJOR CV EVENT • • • 5804 patients (2804 men), 70-82 years with history of, or risk factors for, vascular disease Pravastatin 40 mg/day vs placebo, follow-up 3.2 years Primary end-point: composite of coronary death, non-fatal MI, fatal and non-fatal stroke Placebo (2913) Pravastatin (2891) Hazard ratio (95%CI) Primary end-point 473 (16.2%) 408 (14.1%) 0.85 (0.74-0.97) CHD death or non-fatal MI 356 (12.2%) 292 (10.1%) 0.81 (0.69-0.94) Fatal/non-fatal stroke 131 (4.5%) 135 (4.7) 1.03 (0.81-1.31) All CV end-points 523 (18%) 454 (15.7%) 0.85 (0.75-0.97) CHD deaths 122 (4.2%) 94 (3.3%) 0.76 (0.58-0.99) Cancer 91 (3.1%) 115 (4%) 1.28 (0.97-1.68) 306 (10.5%) 298 (10.3%) 0.97 (0.83-1.14) All-cause mortality CHD, non-fatal MI, fatal/non fatal stroke CHD death or non-fatal MI Fatal/non-fatal stroke Studio osservazionale su 7220 pazienti con CAD definita angiograficamente, seguiti per un periodo di 3.3 anni in relazione all’uso di statine in rapporto all’età Mortalità in pazienti che assumevano (colonne bianche) e non assumevano (colonne nere) statine Analisi multivariata dell’effetto delle statine sulla mortalità complessiva nei pazienti di 80+ anni 9 trials, 19569 pazienti, range età basale 65-82 anni (A) (C) RRR 22%, NNT 28 RRR 26% , NNT 28 (D) (B) RRR 25%, NNT 58 RRR 30%, NNT 34 Bayesian Forest Plot for Mortality (A) Bayesian Forest PlotAll-Cause for Non-Fatal MI (C) and Coronary (B) Bayesian Heart ForestDisease Plot forMortality Stroke (D) Studio osservazionale su pazienti >80 anni con diagnosi di IMA tra il 1999 e il 2003. Analisi di sopravvivenza ed eventi in relazione all’uso di statine sul campione totale (popolazione A, 14907 pazienti) e dopo aver escluso quelli deceduti entro 14 giorni (popolazione B) ed entro un anno (popolazione C) 51351 pazienti >60 anni in RCT con statine, prevenzione primaria e secondaria EDITORIAL Statin Therapy in Older Persons Pertinent Issues LDL lowering therapy undoubtedly should be one therapeutic modality for secondary prevention in older persons with CHD The issue of LDL lowering drugs for older persons without CHD is more problematic. LDL lowering drugs should be reserved for persons who are deemed to be at higher risk. In younger elderly (65-75 years) use of statin therapy even in primary prevention is justifiable; in the older persons (>75 years) statins should be used more cautiously (Grundy S., Arch.Intern. Med. 2002, 162, 1329) ..il rischio di rabdomiolisi è principalmente determinato dalla dose di statina piuttosto che dall’entità della riduzione del colesterolo LDL… .. il maggior determinante del beneficio associato all’uso delle statine è l’entità della riduzione del colesterolo LDL piuttosto che il tipo o la dose di statina usata… il maggior determinante della tossicità (peraltro assai modesta) delle statine non è l’entità della riduzione del colesterolo LDL quanto la dose di statina usata… sembra pertanto prudente non usare dosi di statine superiori a quelle necessarie a raggiungere l’obiettivo LDL desiderato ..l’insieme delle evidenze rassicura sul fatto che l’impiego delle statine non è associato ad un maggior rischio di cancro rispetto al placebo… Major CV events In-hospital death CYP3A4 Amiodarone Clarithromicin, Erythromicin Cyclosporine Diltiazem, Nifedipine, Verapamile, Lacidipine Itraconazole, Ketoconazole Bioav Lipophil Protein Midazolam %Nefazodone bind. Quinidine Sildenafil Warfarin Clinical Pharmacokinetics of STATINS Tmax hours ATORVA 2-3 Metab. pathw. Active metab. T 1/2 hours Urinary/ Fecal excret. 12 Yes 80-90 CYP 3A4 Yes 15-30 2/70 FLUVA 0.5-1 20-30 Yes >99 CYP 2C9 No 0.5-2 6/90 PRAVA 1-1.5 18 No 43-55 Sulfation No 1-3 20/71 SIMVA 1-2.5 5 Yes 94-98 CYP 3A4/5 Yes 2-3 13/58 3 20 No 88 CYP 2C9 Yes (minor) 21 10/90 ROSUVA CYP2C9 Alprenolol Diclofenac Fluvastatin Phenitoin Tolbutamide Warfarin Pharmacol.Ther. 1999, 84, 413-428 J.Clin.Pharmacol. 2002, 42, 963-970 ELDERLY & SAFETY OF STATINS Patients at highest risk for CHD include older individuals, patients after transplantation and patients with hypertension, diabetes or multivessel disease…who are also the most likely to need multiple medications and thus are at greatest risk for drug-drug interaction FACTORS INCREASING THE RISK OF MYOPATHY • • Patient characteristics: older age; female sex; renal insufficiency; hepatic disease; hypothyroidism; grapefruit juice; polypharmacy Statin properties: high systemic exposure; lipophilicity; high bioavailability; limited protein binding; potential for drug-drug interactions metabolized by CYP pathways (CYP3A4) WHEN PRESCRIBING STATINS CONSIDER: • • • • Personal characteristics: advanced age (women and patients >80 years), frailty, small body frame, alcohol abuse, muscle disorders, grapefruit juice Disease burden: multisystem disease (chronic RF with diabetes), hypothyroidism, antecedent liver or muscle disease High-risk clinical situations: perioperative period Medication burden poiché l’anziano è estremamente sensibile e vulnerabile agli effetti avversi delle terapie mediche, la prevenzione cardiovascolare nel vecchio non può prescindere dal •Mantenimento e miglioramento dell’autonomia funzionale •Mantenimento della performance psico-cognitiva •Prevenzione del danno iatrogeno •Prevenzione delle cadute Età estremamente avanzata e/o ridotta spettanza di vita Dipendenza e non autonomia Estrema fragilità Severe comorbilità irreversibili Valutazione rischio CV globale FRAIL /DISABLE Isolati fdr dopo i 75 anni Valutazione spettanza di vita, comorbilità e politerapia, stato funzionale e cognitivo, fragilità, tono dell’umore, volontà individuale… DM e/o plurimi fdr dopo i 75 anni DM e/o plurimi fdr prima dei 75 anni Precedenti clinici CV FIT In sintesi: • La terapia con statine non ha indicazione razionale negli anziani con ridotta spettanza di vita, dipendenza funzionale, fragilità o severe comorbilità croniche irreversibili. • Negli anziani «robusti» la terapia con statine può essere utile e dovrebbe essere impiegata per ridurre le recidive vascolari dopo un evento coronarico. • Negli anziani «robusti» ad alto rischio di ma senza precedenti CV una terapia con statine già in atto e ben tollerata può essere continuata fino ai 75 – 80 anni con le più basse dosi efficaci a condizione che non vi sia rischio di interazioni e tossicità. Non vi sono invece sostanziali evidenze circa l’opportunità di iniziare una prevenzione primaria con statine dopo i 75 anni.
Scarica