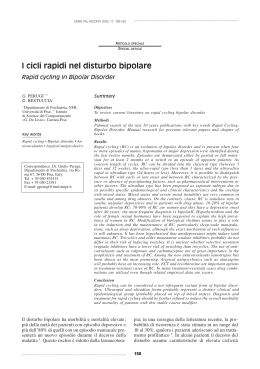
14/04/2014 Firenze, 11 aprile 2014 Disturbo Bipolare e Demenza: una Relazione Complessa Claudio Vampini Dipartimento per la Salute Mentale e Università di Verona Disturbo Bipolare e Demenza: una Relazione Complessa Disturbo Bipolare Litio / Valproato? Demenza 1 14/04/2014 Prevalence of Dementia in Europe Pooled analyses of 11 studies from the EURODEM group (Lobo et al., 2000) \ Ott A, et al. Incidence and risk of dementia. The Rotterdam Study. Am J Epidemiol 1998; 147(6): 574-580 Hebert R, Brayne C. Epidemiology of vascular dementia. Neuroepidemiology 1995; 14: 240-257 2 14/04/2014 Prevalence of Bipolar Disorder in Older Adults in Various Setting Setting N° of Studies Prevalence (Gen Pop: 0.5 – 6%) Community studies 4 0.08% - 0.46% Inpatients psychiatry 11 8 - 10 % Outpatients psychiatry Long-term care istitutions Psychiatric emergency rooms 3 2 - 8% 3 3 - 17.4% 2 14 - 17% Depp & Jeste, Bipolar Disord 2004; 6(5): 343–67 Sajatovic et Al, Am J Geriatr Psychiatry 2005;13:282-289 Depression (D) Early-onset D: 2X Dementia Risk Late-onset D: most studies support an association (> severity, male g, education) Dementia 3 14/04/2014 Disturbo Bipolare e Demenza: una Relazione Complessa Disturbo Bipolare Early-onset Late-onset Demenza Disturbo Bipolare e Demenza: una Relazione Complessa Disturbo Bipolare Early-onset Demenza 4 14/04/2014 Deficit Cognitivo nel Disturbo Bipolare • Presente già in fase premorbosa e poi in eutimia. • Apprendimento, memoria verbale, funzione • • • esecutiva. Peggiora nel follow-up (>> funzione esecutiva) Predittori di gravità: n° episodi di malattia n° episodi maniacali sintomi depressivi residui durata di malattia Stile di vita, malattie fisiche/SNC, terapie? Robinson & Ferrier. Bipol Dis, 2006;8:103-116; Torrent et al, J Clin Psych, 2012;73 e899-e905 •Does Rate the of dementia increased 13% with every episode forthe risk of developing dementia increase with patients with Depressive and 6% with Bipolar n° of episodes in patientsDisorder with Depressive Disorder and in patients with Bipolar Disorder ? (1970 -1999) Disorder, when adjusted for differences in age and sex. HR disturbo depressivo; n 18726 HR disturbo bipolare; n 4248 IC 95% 1 episodio* 2 episodi 3 episodi 4 episodi Tipo ≥5 episodi di disturbo§ *Tasso di diagnosi di demenza per i pazienti con un certo numero di episodi rispetto al tasso per i pazienti con un episodio precedente. §L’effetto del tipo di disturbo per i pazienti con un episodio Kessing et al. Neurol Neurosurg Psychiatry 2004;75:1662-1666 5 14/04/2014 3.2 • N: 13 DB, 70.8 (± 7.7) a. • Demenza dopo 29.1 (± 10.1) a. da esordio di DB. MMSE medio 24.0 (± 4.3) • Follow-up 6.1 a. (± 2.8) MMSE medio: 23.5 (± 3.2) modesta sindrome comportamentale frontale SPECT: ipocaptazione FT (PAR) bilaterale non soddisfatti criteri per AD, VaD, FTD, LBD • Possibile “Demenza post-DB” ? BvFTD and Primary Mania: Overlap in Symptoms • Euphoria: inappropriate childlike jocularity (e.g. repetitive phrases and jokes), vs. pressured speech and sustained emotional intensity. • Disinhibition: undue familiarity, carelessly voicing insulting observations, petty theft, sexual acting out, or poor financial decisions. • Complex stereotyped movements, vocalizations, and other compulsions may resemble agitation seen in BD. • Mindless habits are invariant, vs. variable, impulsive expressions of intense emotion, as seen in true mania. • BvFTD vs. BD: insidious onset and progressive nature, stereotyped movement and speech, disinhibition without remorse, profound loss of empathy and social sensitivity, overeating or compulsive eating, lack of insight and concern, absence of periodicity. Woolley et Al, J Clin Psychiatry. 2011 February ; 72(2): 126–133. 6 14/04/2014 Disturbo Bipolare e Demenza: una Relazione Complessa Disturbo Bipolare Late-onset Demenza Late-onset Bipolar Disorder: a Distinct Subtype? Age at first admission in patients with and without family psychiatric history. 30 n=277 Number of cases (%) p: 0.029 Familial by set criteria Non-familial 20 10 p: 0.007 “Mixed Features” 0 12 17 22 27 32 37 42 47 52 57 62 72 77 82 87 Age of first admission (years) All patients discharged from a district in-patient service diagnosed with Bipolar Disorder in a 7-year period were ascertained from a case register Moorhead SRJ, Young AH. J Affect Disord 2003;73:271-277 7 14/04/2014 Mixed States and “Pseudodementia” Mood disorder: from the sixth to seventh decade of life and onward. Attention and concentration problems. MIXED features: mood instability, irritability, agitation, irregular drive and sleep. “Strong” temperament, extremely active life earlier, often with a charismatic style, but more manifest in strong sexual indiscretions in recent months. Possible evolution in dementia. Akiskal et al, 2011; Perugi, SOPSI, 2014, mod “Vascular Mania” 8 14/04/2014 Iperintensità della sostanza bianca nei gangli della base e in regione frontale e parietale in p.ti anziani con DB ad esordio precoce e tardivo (>60 a.) # # L.O. *p=0,018; +p=0,027; §p=0,006; ^p=0,045 #PV-WMH=iperintensità della sostanza bianca periventricolare ##D-WMH=iperintensità della sostanza bianca profondaa ## E.O. Tamashiro et al. Bipolar Disorders 2008:10:765-775 • Later age of first manic episode and greater vascular disease burden were related to lower memory performance. • There is arguably a BD “vascular subtype”, where vascular brain changes are related to mania and cognitive decrements in late life. Gildengers et al, 2010 9 14/04/2014 Proposed predominant pathways linking Depression (Bipolar Disorder?) to the onset of Dementia Bipolar Disorder The pathways linking depression and dementia are likely to be multifactorial and probably not sequential. Byers, A. L. & Yaffe, K. Nat. Rev. Neurol. 7, 323–331 (2011) Disturbo Bipolare e Demenza: una Relazione Complessa Disturbo Bipolare Demenza 10 14/04/2014 Bipolar Type VI ?: "Bipolarity" in the Setting of Dementia • Demenza conclamata, senza storia di DB • «Mixed Features» BPSD: instabilità umorale, disforia, agitazione, ansia, irritabilità, CNS Spectr. 2008;13(9):796-803 disinibizione, aggressività • Temperamento ipertimico, ciclotimico, irritabile • Familiarità per DB formale o spettro bipolare • Peggio con AD; meglio con basse dosi di SU o SGA Disturbo Bipolare e Demenza: una Relazione Complessa Disturbo Bipolare Litio / Valproato? Demenza 11 14/04/2014 Litio negli Anziani con Mania Acuta • Nessun RCT • Dosi ridotte del 25-50% vs. adulti giovani • Range terapeutico consigliato: 0.5 - 0.8 mEq/L 65 – 75 anni: 300 - 600 mg/d ≥ 80 anni: 150 - 300 (450) mg/d • Elevata variabilità interindividuale • Possibili litiemie elevate a basso dosaggio per modificazioni e/o interazioni cinetiche • Valutare età, tollerabilità, fragilità Sproule et al, Drugs & Aging, 2000, 16, 3, 165-177 Aziz et al, Am J Geriatr Pharmacotherapy, 2006, 4, 347-364 Young et al. Am J Ger Psychiatry 2004;12:342-357 Brain Lithium Levels and Effects on Cognition and Mood in Geriatric Bipolar Disorder: A Lithium - 7 Magnetic Resonance Spectroscopy Study • Brain Li levels do not correlated with serum Li for subjects ≥ 50 yo •• The absence a Elevations in of brain predictable (but not serum) Li relationship between levels were associated serum and brain with frontal lobe Li makes specific dysfunction and individual predictions higher HDRS scores about the “ideal” Li serum level in an older adult with BD difficult. N 26 (50 - 85 years old: N 10) • Li crosses the BBB with a mean ratio of serum to CSF Li of 3.6 : 1 Forester et Al, Am J Geriatr Psychiatry 2009; 17:13–23 12 14/04/2014 Litio: Neurotossicità negli Anziani • • • • Confusione, atassia, acatisia, delirium Anche con litiemia in range per possibile incremento del Li intracellulare* Più frequente nelle manie "secondarie” Favorita da: sofferenza SNC clinica o subclinica associazione con AP (FGA > SGA) SMN associazione con SSRI/SNRI Sindrome Serotoninergica Young et al, 2004; Sajatovic et al, 2005; Aziz et al, 2006; *Forester et al, 2009 Valproato negli Anziani con Mania Acuta • Dosaggi: 125 >> 250 - 2.250 mg/die • Efficacia indipendente dal livello plasmatico • Mania late-onset • Mania secondaria a: patologie mediche patologie neurologiche – 1 RCT nella mania in corso di demenza Young et al. 2004, Am J Ger Psychiatry 12,342-357;Tariot et al, 2001, Curr Ther Res, 62, 51-67 13 14/04/2014 Valproato: Neurotossicità negli Anziani • • • • Tremore fine Sedazione Atassia, parkinsonismo Delirium ↑ Rapido dosi ? non iperammoniemico ↑ Frazione libera ? iperammoniemico • M Alzheimer: studio a 1 anno a gruppi paralleli vs. placebo > atrofia cerebrale (RMN) con accelerato decadimento cognitivo? Young et al, 2004; Sajatovic et al, 2005; Aziz et al, 2006; *Fleisher et al, Neurology, 2011;77:1263–1271 14 14/04/2014 Fountoulakis et al, International Journal of Neuropsychopharmacology (2008), 11, 269–287 Litio e Valproato: Neuroprotezione ? potenziale apoptosi Destabilizzazione e degradazione della β - catenina P + + + β - catenina + GSK - 3 β P P Tau + - P - Li- VPA + PEBP2 β + Bcl2 “grovigli” neurofibrillari 15 14/04/2014 • The classification of the data suggests that the evidence is of level C, that is ‘unclear or conflicting’. Does Lithium Protect Against Dementia? Authors Study Results Brinkman et al, 1984 Open – 5 weeks N 14 SDAT Li+ with mean serum concentrations up to 0.6 meq/liter did not alter memory scores significantly. Hampel et al, 2009 Single blind – 10 weeks N 71 SDAT Li+ did not lead to change in the ADAS-Cog subscale or in depressive symptoms No effect on GSK-3 activity or CSF-based biomarker concentrations. Terao et al, 2006 Retrospective N 1423 BD Those who had previously received Li+ and/or were currently prescribed Li+ had significantly better MMSE scores than the control patients. Nunes et al, 2007 Cross-sectional N 118 older BD Kessing et al, 2010 Retrospective N 4856 BD Forlenza et al, 2011 RCT – 12 months N 45 MCI Li+ treatment reduced the prevalence of AD in patients with BD to levels in the general elderly population. Continued treatment with Li+ was associated with a reduced rate of dementia in patients with BD. Li+ treatment was associated with a significant decrease in CSF concentrations of P-Tau and better performance on the cognitive subscale of the AD Assessment Scale and in attention tasks. C. Vampini, F. Nifosì, NOOS, VOL 19 N 3, 2013 16 14/04/2014 Conclusioni • Il Disturbo Bipolare è associato, nel follow-up, ad incremento della diagnosi di demenza. • La diagnosi differenziale è più complessa per DFT che per AD o VaD. • Fattori patogenetici comuni o associazione casuale? • Late-onset «vascular mania»: quale rischio di evoluzione in VaD? • DB tipo VI con «mixed features»: slatentizzazione di diatesi bipolare in corso di AD? • • Litio e valproato: neurotossici, neuroprotettivi ? Future ricerche: batterie di test, brain imaging, biomarkers di AD nella fase precoce del DB. 17
Scarica